

Abstract
Third generation quinolones are extensively used to treat a variety of common bacterial infections. Due to their extensive use in clinical practice, an increase in neuropsychiatric events has been reported. We report the case of psychotic symptoms occurs after three doses of moxifloxacin in a healthy adult male with no underlying risk factors. After the discontinuation of moxifloxacin treatment, there was a complete resolution of patient's symptoms. The case draws attention to a rare side effect of a commonly use drug and alert the clinicians to be cautious in those patients that have a baseline risk factors which makes the patient more susceptible to such adverse drug effect.
Keywords: Anxiety, hallucination, insomnia, Moxifloxacin
INTRODUCTION
Moxifloxacin is a third generation quinolone which has a broad antibacterial spectrum. It is used in the treatment of respiratory, intra-abdominal, urinary tract, skin and soft tissue infections. Overall, it has a low rate of adverse reactions, 2% compared to other quinolones having about 10%. According to pharmacovigilance studies moxifloxacin along with levofloxacin, are quinolones that have less central nervous system (CNS) adverse effects (1% or less of the overall rate).[1] Most of the reported cases of CNS adverse effects of quinolones are of second-generation (ciprofloxacin, norfloxacin, and ofloxacin).
In general, quinolones have a good safety profile, and they are well tolerated, but sometimes can produce adverse drug reactions (ADRs). The most common adverse effects of quinolones are gastrointestinal (up to 20% according to the literature). CNS ADR was also reported and mentioned in product monograph, which is less frequent, around 3%.[2,3] There is one reported a case of moxifloxacin-induced hallucination in a patient with severe sepsis secondary to community-acquired pneumococcal pneumonia.[4]
Here, we describe a case of a young healthy adult male patient treated with moxifloxacin who developed symptoms of acute psychosis. As of the writing of this case, to our best knowledge, there are no previously published case reports related to moxifloxacin-induced visual and auditory hallucination, especially in a healthy individual with no underlying disease or risk factor.
CASE REPORT
A 40-year-old man was seen in an emergency department with a 2-day history of increasing productive cough, malaise, wheezing, and fever. He had no known allergies or illnesses and not taking any medications at present. On examination, he was febrile at a temperature of 102.3°F, respiratory rate 22 breaths/min, blood pressure 120/78 mm Hg, and heart rate 90 beats/min. Routine hematological investigations and chest X-ray were essentially normal. After the relevant examination, he was diagnosed with acute bronchitis and discharged with a prescription of moxifloxacin 400 mg (MOXIGET™, Getz Pharma) OD for 5 days and paracetamol (Panadol®, GlaxoSmithKline Pharmaceuticals Ltd.) 500 mg q 6 h.
After 72 h, the patient was returned to the hospital accompanied by his wife with the symptomatic improvement of the respiratory condition, which was confirmed by the physical examination. This time, the patient chief complaint was “he is anxious, unable to sleep the whole night, and some scary thing starts to follow him and calling his name.” He was referred to psychiatry.
The same day, he was consulted on psychiatry outpatient department. Initial psychiatric work-up revealed that the patient had no previous psychiatry history, nor any family history of the neuropsychiatric disorder. During the interview, her wife told that he was worrying about various day to day things in the night and irritable toward her and child. The patient stated to a psychiatrist that “I see the devil. I've been seeing and hearing him. I can't take it anymore! Please help me!” His physical examination was unremarkable. Laboratory test results were within normal limits, including CHEM-7, complete blood count, liver function tests, thyroid-stimulating hormone, and lipid panel, which ruled out metabolic causes of his symptoms. The drug screen was found negative. It establishes a clear temporal relation between the onset of moxifloxacin treatment with the onset of persistent insomnia and impaired visual and auditory perceptions in the external environment and awareness of unreality. While establishing this relationship, we decide to conduct a literature review to find similar cases reported in young and healthy patients as presented in this case.
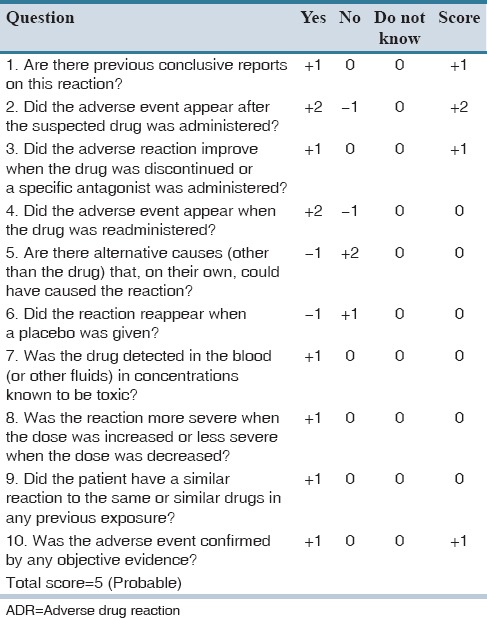
A suspected diagnosis of the moxifloxacin-induced acute psychotic episode was made, and it was decided to discontinue moxifloxacin and start azithromycin with 24 hr. of in-patient monitoring. Twelve hours after discontinuation of moxifloxacin, there was an absolute resolution of patient's symptoms as evident by repeat psychiatric evaluation which revealed him to be alert and oriented with no further anxiety, insomnia, and hallucinations. Since the Naranjo ADR probability scale score[5] for this association was “probable” (score 5), this further supports our hypothesis [Table 1].
Table 1.
Naranjo adverse drug reaction probability scale
DISCUSSION
The main adverse effects of moxifloxacin are related to gastrointestinal system (5%). The CNS represents a low percentage about 0.2–1.1%.[2] The package insert of moxifloxacin listed variety of neurological (headache, dizziness/vertigo, drowsiness, insomnia, paresthesia, tremor, confusion, convulsions, hypoesthesia, visual and hearing disorders, somnolence, peripheral neuropathy, and polyneuropathy) and psychiatric (potentially culminating in self-injurious behavior such as suicidal ideation/thoughts or suicide attempts,) side effects. In general, these adverse effects occurring at very low frequency. These symptoms are among those that were experienced by our patient; these include anxiety, nervousness, and insomnia (uncommon; 0.1-1%) and a rare agitation, hallucinations and depersonalization (<0.1%).[2] Of note, the use moxifloxacin in our patient is most likely empiric as it is difficult to differentiate between viral or bacterial infection because the symptoms are often similar.
Many of the reported cases of quinolones-induced neuropsychiatric events are those in which these drugs have been used in a specific patient profile and/or with concomitant interacting drugs. In certain conditions, there is an increased the risk of adverse effects, and more cases of quinolones-induced-neurotoxicity have been reported these includes elderlies, patients with underlying neurological diseases such as epilepsy, head trauma, cerebrovascular disease, and anxiety.[6]
The product description monograph of moxifloxacin also mentioned that there is an increased risk of psychotic reaction in a patient with baseline psychiatric illness.[7] In addition, the risk also appears greater with concomitant use of penicillins, cephalosporins, carbapenems, theophylline, warfarin, and nonsteroidal anti-inflammatory drug.[6,8,9]
The mechanism of moxifloxacin-induced acute psychosis and other quinolones appear to be related to interaction with neurotransmitters, particularly their structural similarity with the gamma-aminobutyric acid (GABA) ergic agonist. Quinolones act on the inhibitory pathway of nerve stimulation, and they produce an antagonizing effect on the GABA-A receptor in the brain and prevent binding of the inhibitory neurotransmitter (GABA) to its receptor. Thus, preventing the inhibition via the opening of chloride channels, thereby perpetuate CNS stimulation.[6,10,11] Other studies report that quinolones, by its structure, act directly on excitatory brain pathways on N-methyl-D-aspartate (NMDA) and α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic (AMPA) acid receptors.[12] These CNS effects of quinolones appear to be a class effect since. Several similar cases have been reported the emergence of anxiety, agitation, and insomnia with levofloxacin. These cases were reported in young and healthy patients, as the patient described in this case, without prior mental history or emergence of these symptoms in the following months and the absence of organic disease and concomitant psychiatric condition.[13] Tasleem and Viswanathan report moxifloxacin-induced delirium and visual hallucination in an elderly patient with a history of drug abuse.[4,14] From these reports, it seems that these CNS effects of quinolones appear to be a class effect.
Other reported cases describe severe neuropsychiatric effects including confusion, agitation and behavioral disorders, the spectrum of delirium and acute psychosis,[15] mostly in elderly patients or patients with underlying organic disease and concomitant treatment with other drugs that might have interacted.
An important finding of our case is the occurrence of the acute psychotic episode in a healthy young person with no kidney and/or liver dysfunction, no drug abuse history, absence of polypharmacy, and no previous personal and family history of psychological illness that would have put him at an increased risk of drug-induced psychosis.
The case and review presented here is intended to: (a) Aware clinicians about the potentially serious and reversible adverse effect of moxifloxacin; (b) to alert the clinician when using moxifloxacin in patients which have baseline risk factors such as patients with underlying psychiatric disease and concomitant use of drugs that may interact and increase the likelihood of adverse effect; (c) and actively participate in pharmacovigilance.
AUTHORS' CONTRIBUTION
Faizan Mazhar: Literature search, case writing. Shahzad Akram: Case follow-up, wiring and manuscript review. Nafis Haider: Manuscript review.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Douros A, Grabowski K, Stahlmann R. Safety issues and drug-drug interactions with commonly used quinolones. Expert Opin Drug Metab Toxicol. 2015;11:25–39. doi: 10.1517/17425255.2014.970166. [DOI] [PubMed] [Google Scholar]
- 2.Bayer Corporation. Avelox ® (Package Insert) 2015. [Last accessed on 2016 Apr]. Available from: http://omr.bayer.ca/omr/online/avelox-pm-en.pdf .
- 3.Clinical Pharmacology. Tampa, Florida: Gold Standard; 2016. [Last accessed on 2015 Dec]. Moxifloxacin. Available from: http://www.clinicalpharmacology.com . [Google Scholar]
- 4.Higdon E, Twilla JD, Sands C. Moxifloxacin-induced visual hallucinations: A case report and review of the literature. J Pharm Pract. 2016:pii: 0897190016637987. doi: 10.1177/0897190016637987. [DOI] [PubMed] [Google Scholar]
- 5.Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30:239–45. doi: 10.1038/clpt.1981.154. [DOI] [PubMed] [Google Scholar]
- 6.Fish DN. Fluoroquinolone adverse effects and drug interactions. Pharmacotherapy. 2001;21(10 Pt 2):253S–72S. doi: 10.1592/phco.21.16.253s.33993. [DOI] [PubMed] [Google Scholar]
- 7.Stahlmann R, Lode H. Safety considerations of fluoroquinolones in the elderly: An update. Drugs Aging. 2010;27:193–209. doi: 10.2165/11531490-000000000-00000. [DOI] [PubMed] [Google Scholar]
- 8.Carbon C. Comparison of side effects of levofloxacin versus other fluoroquinolones. Chemotherapy. 2001;47(Suppl 3):9–14. doi: 10.1159/000057839. [DOI] [PubMed] [Google Scholar]
- 9.Elbe DH, Chang SW. Moxifloxacin-warfarin interaction: A series of five case reports. Ann Pharmacother. 2005;39:361–4. doi: 10.1345/aph.1E179. [DOI] [PubMed] [Google Scholar]
- 10.De Sarro A, De Sarro G. Adverse reactions to fluoroquinolones. an overview on mechanistic aspects. Curr Med Chem. 2001;8:371–84. doi: 10.2174/0929867013373435. [DOI] [PubMed] [Google Scholar]
- 11.Mandell L, Tillotson G. Safety of fluoroquinolones: An update. Can J Infect Dis. 2002;13:54–61. doi: 10.1155/2002/864789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Rubio-Nazabal E, Alvarez-Pérez P, Sánchez-Vidal E. Acute confusional syndrome due to levofloxacin. Enferm Infecc Microbiol Clin. 2013;31:704–5. doi: 10.1016/j.eimc.2013.04.011. [DOI] [PubMed] [Google Scholar]
- 13.Kandasamy A, Srinath D. Levofloxacin-induced acute anxiety and insomnia. J Neurosci Rural Pract. 2012;3:212–4. doi: 10.4103/0976-3147.98256. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Tasleem H, Viswanathan R. Moxifloxacin-induced delirium with hallucinations. Psychosomatics. 2011;52:472–4. doi: 10.1016/j.psym.2011.01.037. [DOI] [PubMed] [Google Scholar]
- 15.Pedrós A, Emilio Gómez J, Angel Navarro L, Tomás A. Levofloxacin and acute confusional syndrome. Med Clin (Barc) 2002;119:38–9. doi: 10.1016/s0025-7753(02)73307-1. [DOI] [PubMed] [Google Scholar]