

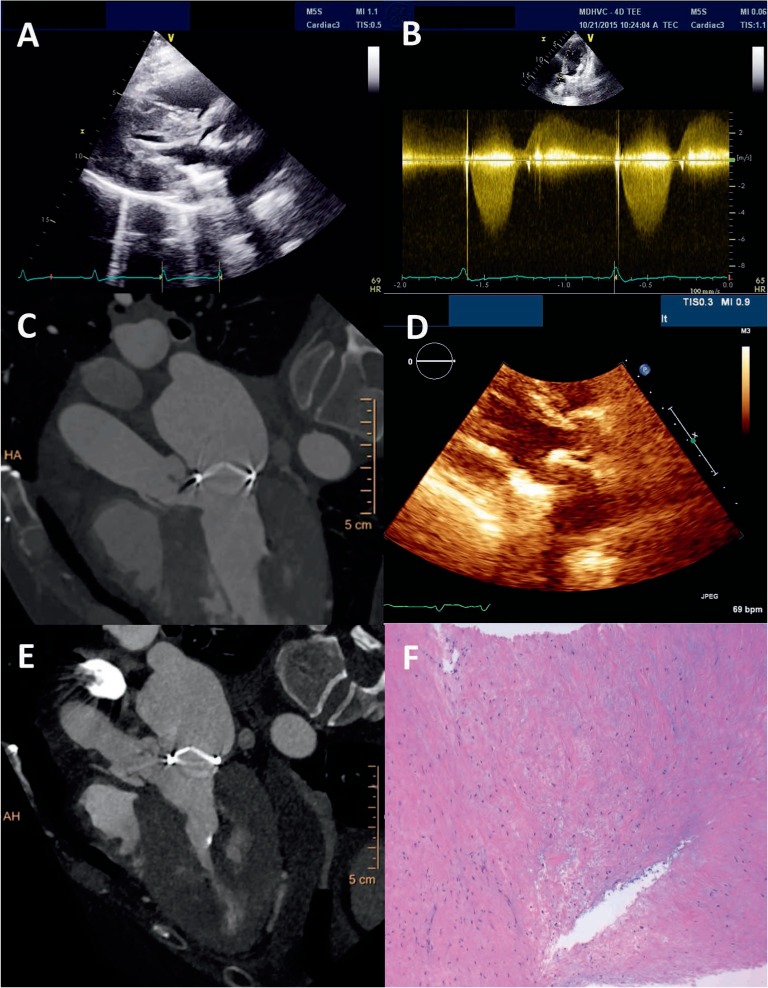
A 54-year-old female with mitral valve replacement presented to the Houston Methodist Hospital with chest pain and dyspnea. (A) Transthoracic echocardiography (TTE) demonstrated marked left ventricular outflow tract (LVOT) narrowing and a frozen aortic valve (AV) cusp (Video 1). (B) Spectral Doppler by TTE across the AV revealed high velocity with rounded contour. (C) Cardiac computed tomography (CT) confirmed suspicion that these findings were referable to extensive pannus formation involving the bioprosthetic mitral valve (Video 2). (D) Following surgical resection, the LVOT appeared normal on TTE. (E) Postoperative cardiac CT also showed return of normal AV leaflet excursion. (F) Pathology of the resected tissue was consistent with pannus, evidenced by fibrous tissue with hypocellular proliferation of bland spindle cells, abundant collagen, and scattered capillaries. TTE also revealed mild stenosis of the mitral prosthesis, with a mean diastolic gradient of 6 mm Hg.
While pannus can develop on both bioprosthetic and mechanical valves in the mitral position,1 extension into either adjoining cavity is unusual, typically involves only the left atrium, and is more typical of thrombosis.2 This is an interesting presentation since LVOT obstruction due to pannus of a mitral prosthesis is rarely seen.
References
- 1. Pibarot P, Dumesnil JG. Prosthetic heart valves: selection of the optimal prosthesis and long-term management. Circulation. 2009. February 24; 119( 7): 1034– 48. [DOI] [PubMed] [Google Scholar]
- 2. Barbetseas J, Nagueh SF, Pitsavos C, Toutouzas PK, Quinones MA, Zoghbi WA.. Differentiating thrombus from pannus formation in obstructed mechanical prosthetic valves: an evaluation of clinical, transthoracic and transesophageal echocardiographic parameters. J Am Coll Cardiol. 1998. November; 32( 5): 1410– 7. [DOI] [PubMed] [Google Scholar]