
Figure 1. Dysbiosis of the subepidermal compartments from skin of AD patients.
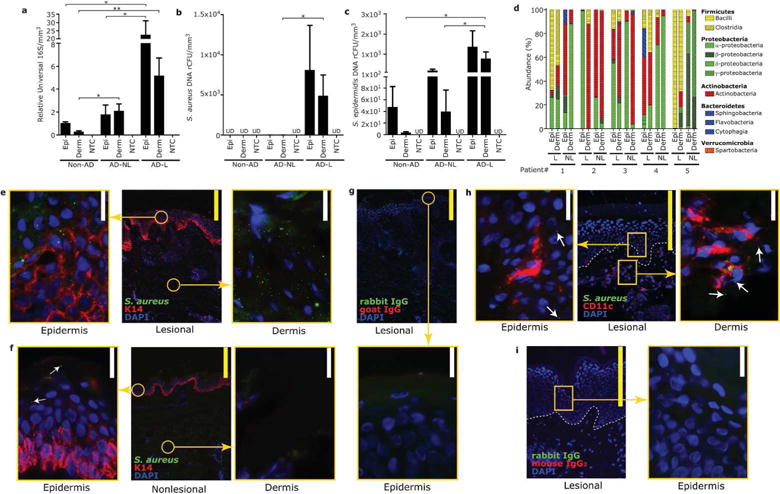
(a) qPCR results for relative abundance of DNA for 16S rRNA, (b) S. aureus (c) and S. epidermidis detected in epidermal or dermal compartments, isolated by laser-capture microdissection (LCM), of skin from normal skin of non-AD subjects, nonlesional and lesional skin of patients with AD. Non-tissue controls (NTC) were simultaneously processed. Data represent mean ± SEM of 11 subjects. *P<0.05, **P<0.01. Epi=epidermis, Derm=dermis, UD=undetectable. (d) 16S rRNA pyrosequencing results from samples isolated by LCM of the epidermis and dermis of nonlesional (NL) and lesional (L) skin of AD subjects. Each bacterial phylum is shown in different color. (e–g) Immunofluorescence for S. aureus and keratin-14 in lesional (e) or nonlesional (f) skin of AD subject. Staining with isotype control (g). (h,i) Immunofluorescense for S. aureus and CD11c in lesional skin of AD subject. Staining with isotype control (i). Arrows indicate S. aureus staining detected outside of CD11c+ immune cells. Immunostaining shown is a representative of 3 biopsies from different donors. Scale bar= 20μm (white) or 200μm (yellow).