
Fig. 1.
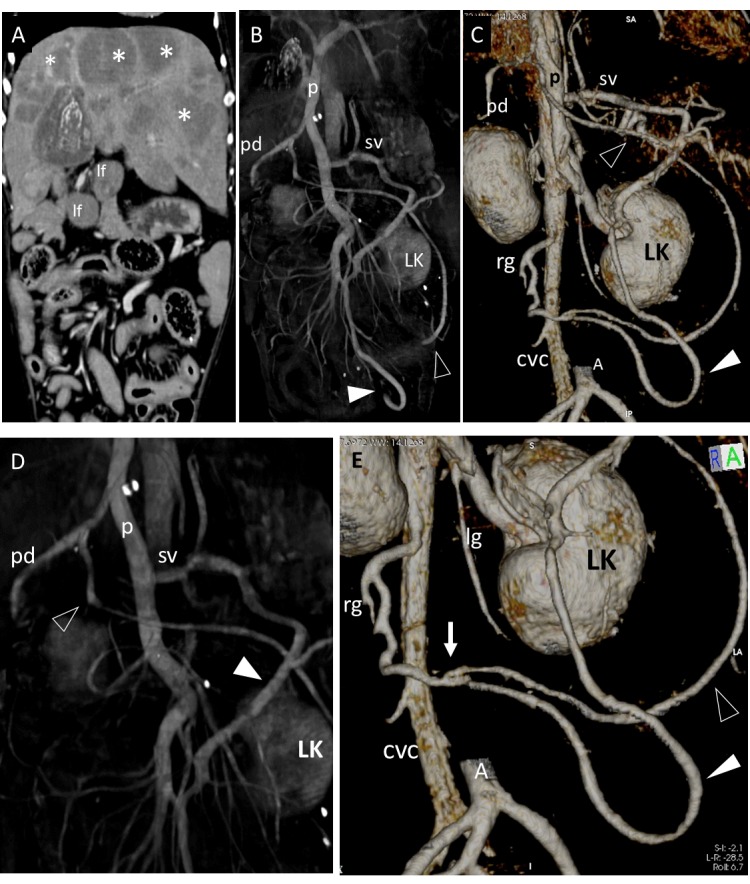
Dog 5 of PH group. (A) Dorsal contrast-enhanced multiplanar reformatted CT image of the abdomen. There are multiple hepatic neoformations (asterisks) ipoattenuating to hepatic parenchyma, periportal lymph nodes enlargement (lf) and no abdominal effusion. (B,C,D,E) Three-dimensional volume rendered image of the portal vein (p) and caudal vena cava (CVC) – ventral views. Two large vessels (empty and full arrowheads) originate respectively from the pancreaticoduodenal vein (pd) and from splenic vein (sv), run caudally and join in a single vessel draining into the caudal vena cava at level of right gonadal vein (rg). (B) whole portal vein, ventral view; (C) detail of the entire PSS from its double portal origin to its caval termination; (D) detail of origins of the anomalous vessels from pancreaticoduodenal vein (empty arrowhead) and splenic vein (full arrowhead); (E) detail of connection (arrow) of the two shunts in one vessel which enters caudal vena cava at level of right gonadal vein. These vessels appeared suggestive of APSS because they were associated with a visible cause of PH (diffuse hepatic neoplasia) and other classical APSS (see Fig. 5). The absence of ascites could be explained by a complete effectiveness of these APSS in alleviating portal pressure. LK, left kidney; lg, left gonadal vein; A, caudal abdominal aorta (sectioned and partially removed).