

Summary
Immune checkpoint inhibitors (ICIs) are being increasingly studied and used as therapy for a growing number of malignancies. ICIs work by blocking inhibitory pathways of T-cell activation, leading to an immune response directed against tumors. Such nonspecific immunologic activation can lead to immune-related adverse events (IRAE). Some IRAE including inflammatory arthritis, sicca syndrome, myositis and vasculitis are of special interest to rheumatologists. As use of ICIs increases, recognition of these IRAEs and developing treatment strategies will become important. In this review, the current literature on rheumatic and musculoskeletal IRAEs is summarized. The incidence, clinical presentations, and treatment considerations are highlighted.
Keywords: arthritis, sicca syndrome, immune checkpoint inhibitors, malignancy, immune related adverse events
Introduction
Interactions between the immune system and cancer are complex, dynamic and bidirectional1. One of the primary roles of the immune system is to recognize and eliminate cells that have undergone malignant transformation, often before a developing tumor can become clinically apparent2. In some instances, successful tumor elimination does not occur, and a malignancy may be held in equilibrium where further tumor growth is prevented. Cancers that grow and reach clinical detection, however, have often developed successful strategies to evade naturally occurring host immune responses. To combat this, immunotherapeutic agents are being utilized to harness the power of the immune system, by increasing the quality or quantity of immune effector cells, eliciting immune responses to specific tumor antigens, or inhibiting mechanisms that cancers develop to evade immunological surveillance and killing mechanisms2.
Immunotherapy approaches to cancer began in the 1980s, when recombinant interleukin 2 (IL-2) was administered for metastatic melanoma with tumor regression seen in a subset of patients3. Since then, cancer vaccines and T-cell infusions have also been used successfully to treat a variety of malignancies. IL-2, T-cell infusions and cancer vaccines all work by directly activating the immune system, thus augmenting host immune responses against malignancies. Another class of cancer therapies, the main focus of this chapter, work differently. These therapies, known as immune checkpoint inhibitors (ICI), work in part by targeting immunoregulatory pathways exploited by some cancers. A number of inhibitory pathways, known as immunologic checkpoints, play critical roles in maintaining self-tolerance and preventing autoimmunity. Multiple tumor types, however, can appropriate immune checkpoint pathways to increase immune resistance in the tumor microenvironment4. T-cells require both the interaction of the MHC molecule on an APC with the T-cell receptor and the second signal of another ligand-receptor interaction to become activated. An example of this is the interaction between B7 molecules (CD80/86) on APCs with CD28 on T cells. B7 can also bind instead to an inhibitory receptor, cytotoxic lymphocyte antigen 4 (CTLA-4) or CD154 (Figure 1A). When this engagement occurs, the T-cell does not become activated. Other immune checkpoints have also been identified and are targets for cancer immunotherapy. Another major immune checkpoint pathway is mediated through the programmed death protein-1 (PD-1) expressed on T-cells and programmed death ligand (PD-L1) expressed on APCs and also on many tumors, where it serves as to dampen the T-cell mediated response and facilitate immunologic evasion5 (Figure 1A). ICIs non-specifically activate T-cells by blocking negative co-stimulatory ligands or receptors on T-cells, antigen presenting cells (APC), and/or tumor cells6.
Figure 1.
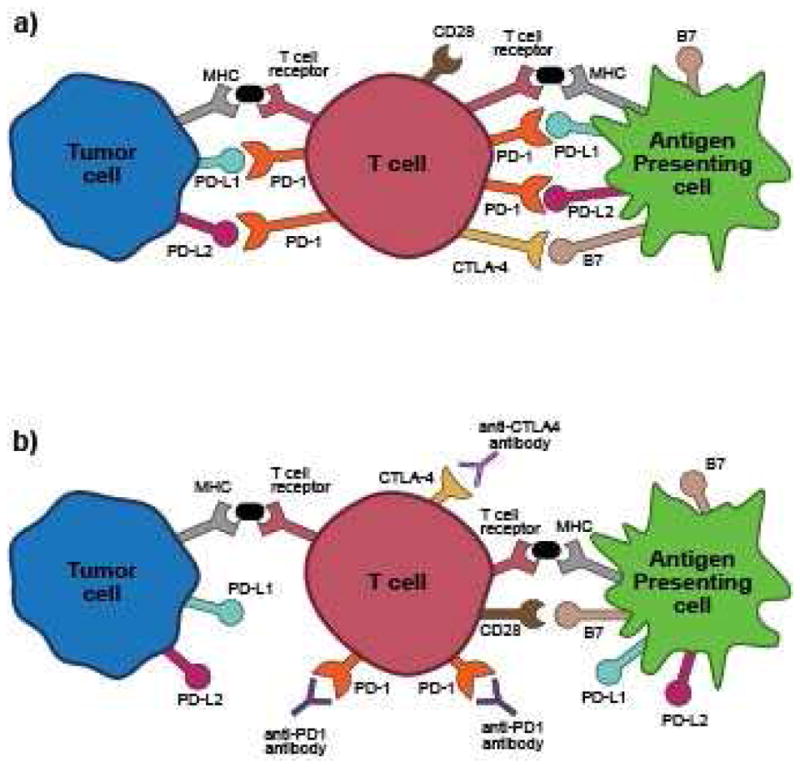
Mechanism of action for immune checkpoint inhibition targeting CTLA-4 and PD-1. A) Inhibition of T-cell activation by interactions with tumor cells and antigen presenting cells (APC). PD-L1 and PD-L2 on tumor cells and APCs bind to PD-1 on the T-cell and B7 on APCs binds to CTLA-4 on the T-cell. B) Antibodies to PD-1 or CTLA-4 block inhibitory interactions, allowing for positive co-stimulation (B7 binds CD28)
Ipilimumab, a monoclonal antibody to CTLA-4, works by blocking the B7 binding to this down-regulatory receptor, thus leading to its unopposed engagement with the positive co-stimulatory receptor, CD28, and subsequent T-cell activation7 (Figure 1B). Agents such as nivolomab and pembrolizumab, antibodies directed against PD-1, and atezolizumab, directed against PD-L1, block this additional inhibitory pathway leading to increased T-cell activation, and can also interrupt down-regulatory signaling mediated through direct tumor-T-cell interactions (Figure 1B). The enhanced activation of T-cells can enhance tumor targeting and killing, but is not specific to only an anti-tumor response
Currently, ICIs with three targets, CTLA-4, PD-1 and PD-L1, are FDA approved (Table 1). Ipilimumab, a CTLA-4 inhibitor, was the first approved for metastatic melanoma in 2011. Nivolumab, targeting PD-1, is approved for metastatic melanoma, non-small cell lung cancer (NSCLC), renal cell carcinoma (RCC), and Hodgkin’s lymphoma. Pembrolizumab, also a PD-1 inhibitor, is approved for metastatic melanoma and a subset of NSCLC. Atezolizumab, which blocks PD-L1, is approved for urothelial carcinoma. A combination regimen of ipilimumab and nivolumab is also approved for metastatic melanoma.
Table 1.
Approved immune checkpoint inhibitors and indications, targets of investigational drugs
| Target | FDA-approved drugs | Drugs in development (partial list) |
|---|---|---|
| CTLA-4 | Ipilimumab (Yervoy)- metastatic melanoma | Tremelimumab |
| PD-1 | Nivolumab (Opdivo)- metastatic melanoma, non small cell lung cancer, renal cell carcinoma, Hodgkin’s lymphoma Pembrolizumab (Keytruda)- metastatic melanoma, PD-L1 positive non small cell lung cancer |
Pidilizumab, AMP-224 |
| PD-L1 | Atezolizumab (Tecentriq)- urothelial carcinoma | Avelumab, Durvalumab |
| LAG-3 | None | BMS-986016, IMP321 |
| B7 | None | Enoblituzumab, MGD009 |
| TIM-3 | None | MBG453 |
| CD137 | None | Urelumab |
Currently approved ICIs provide a more effective therapeutic option for a variety of advanced stage cancers. In metastatic melanoma, ipilimumab, pembrolizumab and nivolumab have shown significant survival benefits when compared to traditional chemotherapy, with five year survival rates up to 25 to 31%7,8. In NSCLC, those treated with nivolumab had a 51% survival at 12 months, compared to 39% with docetaxel9. In RCC, there was nearly a six month survival benefit for nivolumab over chemotherapy10. Combination therapy targeting different checkpoints can be even more effective; treatment with ipilimumab and nivolumab for metastatic melanoma had a partial or total response rate of 60% in one study11 compared to 11% with ipilimumab alone.
Due to these successes in melanoma, NSCLC and RCC, there are many other ICI drugs currently in clinical trials, including drugs targeting programmed death ligand (PD-L1), T-cell immunoglobulin and mucin domain 3 (TIM-3), and lymphocyte activation gene 3 (LAG-3)6, which represent other checkpoint pathways (Table 1). In addition, these and currently approved ICIs are being studied in clinical trials alone and in combination, for a wide variety of cancers, from solid tumors to hematologic malignancies, and for cancer at various stages as part of initial regimens in addition to treatment of refractory disease6,12. With reports of efficacy in trials for diverse tumors like Merkel-cell carcinoma13 and a subset of colorectal cancer14, the approved indications of ICIs are likely to expand in the near future. With this expected increase in indications, many more people will be exposed to these therapies.
Why is this growth in the use of ICIs significant to the rheumatologist? ICIs can cause adverse effects through immune-mediated tissue damage known as immune-related adverse events (IRAE). These events vary widely in severity and can affect nearly any organ system. The incidence of IRAE varies by type of therapy and underlying malignancy15,16. Rash has been the most commonly reported event, in up to 30–35% of patients treated with PD-1 inhibitors for melanoma8. Cutaneous manifestations include vitiligo, neutrophilic dermatoses, pruritus, and toxic epidermal necrolysis17. Colitis and pneumonitis are less common, with incidence ranging from 1% to 5% in patients treated with anti-PD-19,10,18 or anti-CTLA-4 19,20 monotherapy. Both of these IRAEs can be severe, however, even resulting in death. Hepatitis, uveitis, pancreatitis, central nervous system disease, and peripheral neuropathies have also been reported21. Clinical manifestations of these IRAEs are described in Table 2. The time course for developing IRAE is variable and can occur after one dose or after several months of therapy22. Skin manifestations and colitis tend to present early in therapy, while pneumonitis and endocrinopathies occur later22. As IRAE are increasingly appreciated, musculoskeletal and rheumatic presentations are beginning to be described. These events, most likely to be seen by rheumatologists, are the focus of this chapter.
Table 2.
Other (non-rheumatic or musculoskeletal) IRAEs and clinical descriptions.
| IRAE | Clinical characteristics |
|---|---|
| Colitis | Diarrhea, in severe cases causing perforation or death. Usually develops earlier in therapy. |
| Rash | Vitiligo, neutrophilic dermatoses, and other skin manifestations reported. Develops early in therapy. |
| Thyroiditis | Usually resulting in hypothyroidism. Can be a late manifestation. |
| Pneumonitis | Ranges from mild dyspnea and cough, to hypoxic respiratory failure. |
| Hypophysitis | Can affect all hormonal axes of anterior pituitary or can be selective. Patients may need permanent hormone replacement. |
| Hepatitis | Transaminitis, with or without elevated bilirubin. |
| Central nervous system | Encephalopathy responsive to steroids has been reported. |
| Peripheral nervous system | Peripheral neuropathy, Guillain-Barre syndrome reported. |
Spectrum and incidence of currently described rheumatic and musculoskeletal IRAE in clinical trials
Arthralgia and arthritis are the most commonly reported rheumatic and musculoskeletal IRAEs in ICI clinical trials to date. The incidence of arthralgia secondary to nivolumab in phase III trials ranges from 5 to 16%9. Similar rates have been reported with ipilimumab monotherapy23,24. Like other IRAE, the incidence of arthralgia appears to be higher in combination ICI therapy, as was seen in a trial for melanoma where the ipilimumab group had a rate of arthralgia of 6.1%, the nivolumab group had an incidence of 7.7 %, and the combination therapy group receiving ipilimumab and nivolumab was 10.5%23. When immunotherapy is combined with other modalities like peptide vaccines, rates of arthralgia have been as reported to be as high as 43% 25.
The incidence of true inflammatory arthritis is less clear. Arthritis is not always reported in publications of clinical trials, and there are several mutually exclusive ways to code musculoskeletal adverse events in the current systems used. For example, arthralgia, arthritis, joint effusion, and musculoskeletal pain are all potential options for coding an adverse event relating to the joint, thus without any standardization in place, the same symptom may be coded differently. This is illustrated in a phase I trial for nivolumab for advanced solid tumors, where two patients were reported as having “arthralgia”, yet they were treated with corticosteroids raising suspicion that these patients actually had inflammatory arthritis26.
Another issue that may contribute to lower reporting of musculoskeletal IRAE is the adverse event grading system used in oncologic trials. Many clinical trial reports only report adverse events of grade 3 or higher and do not mention events of lower severity. In the Oncology Common Terminology Criteria for Adverse Events (CTCAE), for arthritis, joint effusion, or arthralgia to reach a grade 3 for reporting would require hospitalization for the joint symptoms or for the patient to be nearly completely disabled. A working group within Outcome Measures in Rheumatology (OMERACT) evaluated the oncologic CTCAE for its applicability in rheumatology settings27. In this exercise, adverse events coded in CTCAE were re-graded, such that events causing impairment of function were upcoded to more severe ratings. Were such a schema in place, it is likely that the musculoskeletal and rheumatic AEs in oncology trials would become more apparent and recognized in terms of their frequency and severity.
There are no observational studies of large cohorts that have systematically monitored patients for inflammatory arthritis with confirmation by rheumatologists. In one observational study, CT and PET/CT before and after therapy with CTLA-4 inhibitors were reviewed. Four of 119 (3.4%) were reported as having arthritis on imaging28. Unfortunately, additional clinical information concerning the arthritis was limited. Further research is needed to identify how prevalent inflammatory arthritis is with different types of ICIs. We recently reported nine cases of inflammatory arthritis secondary to treatment of nivolumab and/or ipilimumab, but an appropriate denominator for incidence was difficult to calculate given the population of clinical trial participants and patients receiving therapy as standard of care, and not all cases occurring in patients in clinical trials could be reported due to publication embargoes29.
ICI-induced sicca syndrome has only been recently described as a clinical entity29. Dry mouth was reported in 24% of patients in a phase one trial of nivolumab and peptide vaccine for metastatic melanoma25; in a phase two trial of nivolumab for RCC, dose-related dry mouth occurred in 3 to 11% of patients 30. In a trial of pembrolizumab versus ipilimumab in advanced melanoma, rates of dry mouth were 4 and 7% in the two dosing regimens of Pembrolizumab18. Dry eyes were noted in two phase I trials of ipilimumab in combination with other therapies in 3%31 and 4% of participants 32. Neither the severity of symptoms nor treatment is apparent from the clinical trials.
Vasculitis has been rarely described in the ICI clinical trial literature. In a phase II trial of ipilimumab with and without dacarbazine for melanoma, one case of grade four “autoimmune vasculitis” was reported among 74 patients treated, but no further clinical description is provided33. In a phase I trial of ipilimumab with and without bevacizumab for metastatic melanoma, one case of giant cell arteritis developed among 46 patients treated32.
Myalgia and muscle weakness have been reported as adverse events in clinical trials. Myalgia was seen in 2 to 18% of participants in trials of nivolumab25,34 and ipilimumab32, while muscle weakness was reported in 1% of patients in a phase II trial of ipilimumab with and without sargramostim32 and 12% of patients in a phase I trial of nivolumab and peptide vaccine25. The clinical descriptions of these events cannot be discerned from the clinical trials to determine if these could have potentially been related to inflammatory muscle disease. Cases of inflammatory myositis have been subsequently reported and are discussed in more detail below.
A single case of lupus nephritis after treatment with ipilimumab has been reported, but no cases of ICI-induced Systemic Lupus Erythematous (SLE) affecting other organ systems have been noted. Scleroderma secondary to ICIs has also not been reported.
Clinical features of rheumatic IRAE
Inflammatory arthritis
Two cases of inflammatory arthritis and tenosynovitis after pembrolizumab therapy have been reported35. Both patients were seronegative (for rheumatoid factor (RF) and anti-cyclic citrullinated peptide (CCP) antibodies and had involvement of large joints. One patient also had involvement of the proximal interphalageal (PIP) joints. MRI of these two patients showed synovitis in the ankle and wrist with enhancement in the tendons consistent with tenosynovitis. For one patient pembrolizumab was held and non-steroidal anti-inflammatory drugs (NSAIDs) used with improvement of the arthritis; the other was managed with pembrolizumab cessation and NSAIDs and hydroxychloroquine.
A case of Jaccoud’s arthropathy and uveitis after treatment with nivolumab for RCC has been described36. The patient initially developed uveitis, which responded to intraocular steroids. This was followed by morning stiffness and reducible swan neck deformities in the hands. No erosions were seen on radiographs of the hands, and ANA was negative. Treatment for the arthropathy was not described.
We have recently reported three subtypes of inflammatory arthritis 29 in nine patients treated with ipilimumab, nivolumab or combination therapy. These subtypes are a polyarthritis similar to rheumatoid arthritis (RA), true reactive arthritis with conjunctivitis, urethritis and oligoarthritis, and a subtype similar to seronegative spondyloarthritis with inflammatory back pain and predominantly larger joint involvement. The arthritis was often additive; patients would start with one or two affected joints and progress to a highly inflammatory polyarthritis. Though most patients have been seronegative, one patient had a positive RF, and three patients had positive anti-nuclear antibodies (ANA), most of low titer. MRI and ultrasound confirmed synovitis in several patients. Four patients had synovial fluid analysis, all of which was inflammatory with 9000–30000 white blood cells/mL and a neutrophilic predominance. In contrast to the patients previously described who experienced polyarthritis from pembrolizumab that responded to NSAIDS and hydroxychloroquine, eight out of nine of this group of patients required systemic corticosteroids for improvement in their symptoms. Doses of steroids were as high as 120 mg daily. Three patients required TNF-inhibitors to control their symptoms.
Sicca syndrome
The only report of sicca syndrome secondary to ICIs to date is four cases of severe salivary hypofunction after treatment with nivolumab, ipilimumab or combination therapy29. The dry mouth symptoms were more severe than dry eyes in all four patients. All patients were negative for Ro antibodies, while one patient was positive for La/SS-B antibodies and had parotitis with a parotid ultrasound showing hypoechoic foci. The patient with parotitis was treated with six weeks of Prednisone, tapering from 40 mg daily that resulted in resolution of parotid swelling.
Myositis
Two cases of inflammatory myopathy from ICIs have been reported. One case was more consistent with dermatomyositis37, where the patient had proximal muscle weakness, a heliotrope rash and “V-neck sign” (erythematous rash of the chest), and an elevated creatinine kinase (CK) level of 1854 U/L. She was treated with Prednisone 80 mg/daily with normalization of her CK. The Prednisone was tapered off after eight weeks and ipilimumab was discontinued. The other case occurred after nivolumab therapy for metastatic melanoma38. This patient had respiratory muscle involvement along with proximal muscle weakness and an elevated CK of 2812 U/L. Nivolumab was stopped, and he received five days of Prednisone 30 mg/daily with eventual improvement. There is also a case of eosinophilic fasciitis, which can be a myositis mimic, secondary to pembrolizumab39.
Vasculitis
Two cases of giant cell arteritis/polymyalgia rheumatica following ipilimumab for metastatic melanoma have been described40. Both patients had temporal artery biopsies confirming the diagnosis and responded to treatment with Prednisone at 50 to 60 mg daily. Single organ vasculitis from ICIs is also possible as retinal41 vasculitis and uterine42 vasculitis have been seen after pembrolizumab and ipilimumab respectively.
Lupus nephritis
One case of lupus nephritis associated with ICI treatment has been reported in a patient treated with ipilimumab for metastatic melanoma 43. When new nephrotic range proteinuria developed, a kidney biopsy was performed with immunofluorescence positive for IgM, IgG, C3 and C1q in the mesangial space. Antibodies to double-stranded DNA were positive initially and negative when checked after discontinuation of ipilimumab. Proteinuria persisted, however, and a venous thrombosis of the left kidney was discovered. After anticoagulation and Prednisone therapy, the patient improved.
Evaluation of suspected rheumatic IRAEs
For patients with suspected rheumatic IRAE, we recommend a full evaluation with a rheumatologist focusing on clinical characteristics, laboratory testing, imaging and other specific tests as outlined in Table 3. As the phenotypes of rheumatic IRAE are not fully understood, learning about which ways IRAE are similar to or different from autoimmune diseases not related to ICIs can potentially be helpful in guiding treatment. Since autoantibody formation is a possible mechanism for the development of IRAE as shown in hypophysitis44, relevant autoantibodies should be evaluated for suspected inflammatory arthritis, sicca syndrome, vasculitis or myositis (Table 3). We recommend evaluating for autoantibodies, though in our own experience to date and in the cases reported, traditional serological markers may be negative. The lack of traditional autoantibodies may suggest a unique mechanism for rheumatic IRAE. Also, the highly inflammatory nature of the syndromes seems to be distinct raising the question of non-specific activation of both immunologic and inflammatory cascades.
Table 3.
Recommendations for evaluation of patients with suspected rheumatic IRAE
| Suspected IRAE | Clinical Exam | Laboratory Studies | Imaging, Other Studies |
|---|---|---|---|
| Inflammatory arthritis | Full joint exam Schober’s test |
ESR, CRP, RF, CCP, ANA, HLA B27 | Synovial fluid analysis Joint ultrasound or MRI |
| Sicca syndrome | Schirmer’s test Palpation of parotid glands Unstimulated salivary flow assessment |
ESR, CRP, ANA, Ro, La | Parotid gland ultrasound Salivary scintigram Minor salivary gland biopsy |
| Myositis | Manual strength testing Dynamometry |
CK, aldolase, ESR, CRP, ANA Myositis panel (Jo-1, PL-7, PL-12, EJ, OJ, Mi-2, SRP) |
Electromyography (EMG) MRI of affected muscle |
| Vasculitis | GCA: palpation of temporal arteries Palpation and auscultation of arteries Skin examination (purpura) Evaluation for mononeuritis multiplex |
ESR, CRP, cANCA, pANCA, MPO, PR3, urinalysis | For GCA: temporal artery biopsy MRI or PET of suspected affected area |
Treatment considerations
No treatment algorithms currently exist for treatment of rheumatic and musculoskeletal IRAEs. For other IRAE, like colitis, pneumonitis, dermatologic manifestations, and hepatitis, treatment recommendations have been developed based on clinical experience15,45. These treatment algorithms give recommendations based on the grade of adverse event about treating with corticosteroids, TNF-inhibitors, and holding or stopping the ICI.
Extrapolating from these algorithms, we suggest basing treatment on symptom severity and functional consequences (Figure 2). NSAIDs and low dose corticosteroids can be used for patients with milder symptoms, with intra-articular corticosteroids also an option for significantly symptomatic joints. Increased dose of corticosteroids, up to 1–1.5 mg/kg daily of Prednisone, may be needed for severe cases. In those who are refractory to Prednisone or who cannot be tapered, starting TNF-inhibitors would be the next recommendation. Based on the responses seen with TNFi for ICI-related colitis, and our own experience, TNF-inhibitors seem to be a reasonable next step in those who have failed steroid tapers. There are some hypothetical concerns about long-term effects of these medications on cancer progression given their association with non-melanoma skin cancer and possible association with melanoma in rheumatoid arthritis46 and the association with solid tumors seen in a trial of etanercept for granulomatosis with polyangiitis47. Infliximab has been used over short periods of time to treat ICI-induced colitis in metastatic melanoma with no ill effects48, but has not been used in extended courses. We would not recommend using abatacept as it directly opposes the mechanism of ICIs. Given the colitis that is possible with ICIs, there are considerable concerns about using tocilizumab and tofacitinib given the concerns of colonic perforation with IL-6 and JAK inhibition. The introduction of biologic agents requires careful evaluation of benefits versus potential risks in consultation with the patient’s treating oncologist.
Figure 2.
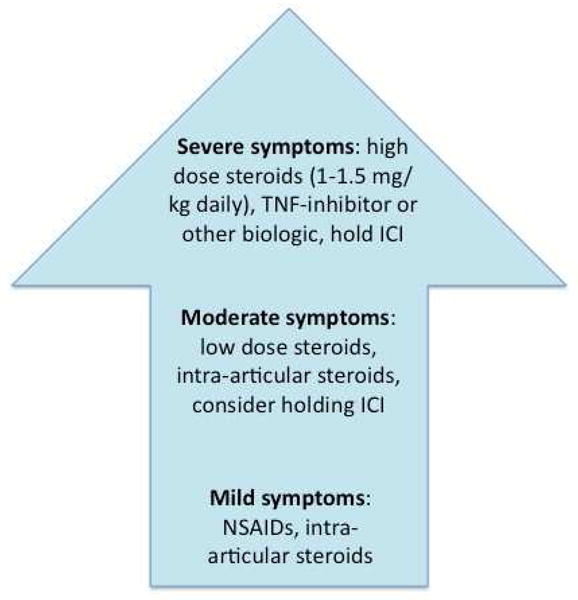
Proposed treatment algorithm. If patients do not respond within 4 to 6 weeks of therapy, escalate to next level of treatment.
Hydroxychloroquine, sulfasalazine, methotrexate or other non-biologic DMARDs can be considered as they are less likely to raise tumor risk or interfere with therapy (Table 4). One consideration with these therapies, however, is their slow onset of action (given the relatively fulminant articular presentations we have seen thus far). In patients with a potentially limited life expectancy, they may fail to achieve optimal effect quickly enough to improve the impairments in quality of life. Similarly, any treatment that is started in patients with rheumatic IRAE should be re-evaluated for response, in about 4 to 6 weeks, and switched to a different modality if there is not improvement.
Table 4.
Potential immunosuppressive therapy for ICI-induced rheumatic IRAE. Drugs to avoid are listed in red.
| Drug options | Likelihood of efficacy | Anticipated time of onset | Effect on cancer risk/cancer response | Potential side effects (overlap w/ICI) |
|---|---|---|---|---|
| HCQ | low | months | Likely no effect | None |
| Sulfasalazine | low | weeks- months | Likely no effect | Allergic reaction/rash? |
| Methotrexate | moderate | weeks- months | Likely no effect | Liver toxicity |
| Leflunomide | moderate | weeks- months | Possible- T cell target | Liver toxicity |
| TNF inhibitors | high | days- weeks | Possible melanoma risk | None |
| Abatacept | high | weeks | Likely impaired response | None |
| Tocilizumab | high | weeks | Unclear | GI issues, colitis |
| Tofacitinib (JAK inhibitors) | high | weeks | Possible- NK cell target | GI issues, colitis |
| Azathioprine | moderate | months | Possible- T cell target | GI issues? |
| Mycophenolate | moderate | weeks- months | Possible- T cell target | GI issues? |
| Anakinra | moderate | days | Likely no effect | None |
| Secukinumab | moderate | weeks | Likely no effect | None |
Other considerations
Metastatic disease: For patients with inflammatory arthritis, if a single joint is disproportionately affected or not improving with therapy, imaging to evaluate for bony metastasis should be performed. This has been reported in a patient with elbow arthritis29.
Treatment length: There is uncertainty about how long to continue treatment in patients with rheumatic IRAE. In other non-rheumatic IRAE, some are self-limited or respond quickly to treatment while others can be persistent22.
Relationship between IRAE and tumor response: The relationship between development of an IRAE secondary to ICI therapy has not been definitively linked to improved tumor regression. It has been appreciated, however, that those treated with interferon for melanoma who exhibit signs of autoimmunity have an improvement in survival49, so this association is theoretically possible.
Quality of life: Patients have been very disabled as a result of rheumatic and musculoskeletal IRAE. Having discussions with patients about their goals and wishes is paramount, especially given that many will have a limited life span.
Immune checkpoint inhibition in patients with known autoimmune disease
The initial trials of ICIs excluded patients with pre-existing autoimmune disease, so there is limited data on how these drugs affect this group of patients. Now that several therapies are approved, case reports and one observational study of patients can provide some guidance on how to manage patients with pre-existing autoimmune disease. For inflammatory bowel disease (IBD), pre-treatment endoscopy to confirm that the IBD was not active allowed for successful use of ipilimumab for metastatic melanoma in one case report50. Another patient with ulcerative colitis was treated with ipilimumab for metastatic melanoma and developed severe colitis requiring colectomy51.
An observational study of 30 patients with various autoimmune diseases (RA, psoriasis, IBD, systemic lupus erythematosus, multiple sclerosis, autoimmune thyroid disease, sarcoidosis and others) who received ipilimumab as standard of care was published in 201552. Of the 30 patients, eight had a flare of their underlying autoimmune disease that could be managed with corticosteroids. Ten patients had a “conventional” IRAE like colitis or hyophysitis, and one patient died of presumptive ICI-induced colitis. Fifteen of the 30 did not have an IRAE or flare of their underlying disease. Six of the patients had a complete or partial response of their malignancy to therapy. From these data, it seems that it is possible to treat patients with a history of autoimmune disease with ICIs, but with careful monitoring as the rate of flare and conventional IRAEs is substantial.
Future directions for clinical practice and research
There are several features of rheumatic IRAEs that merit further study. Pathogenesis of rheumatic IRAE is unclear and will likely differ from classical autoimmune diseases. The optimal timing of treatment (e.g. induction, tapering) is unknown, as are the true clinical spectrum of illness and risk factors for developing IRAE. Concerns with immunosuppressive agents increasing risk of tumor recurrence must also be evaluated. Addressing these issues will require a concerted effort involving rheumatology and oncology investigators, well-characterized patient phenotypes, and examination of potential mechanisms for the development of these events. Understanding risk factors for developing an IRAE the events can help risk-stratify individuals at the start of therapy and influence clinical monitoring. Optimal treatment will require in-depth discussions between rheumatology and oncology concerning the risks versus benefits, likelihood of success for treatment of the underlying malignancy, and with the patient concerning overall quality of life. The advances in immunological understanding related to the bidirectional relationships between autoimmunity and cancer53,54 provide an important basis for investigation and should help to further our understanding of the immunological continuum to develop optimal strategies.
Summary
ICIs will be increasingly used as they are approved for more tumor types, for use in combination, and as novel therapies targeting other immune checkpoint molecules are also approved. As use increases, there is a great likelihood that patients will be referred to rheumatology for evaluation and longitudinal management. Recognizing these syndromes and rapidly initiating therapy may help improve quality for life for affected patients. With careful evaluation of larger cohorts of patients, the incidence of rheumatic and musculoskeletal IRAE will be better defined and the mechanisms may be better understood.
Key Points.
By blocking inhibitory pathways of T-cell activation, Immune checkpoint inhibitors (ICIs) can cause immune-related adverse events (IRAE) including inflammatory arthritis, myositis, vasculitis and sicca syndrome.
Treatment of ICI-induced rheumatic IRAE requires different considerations than treatment of classic rheumatic conditions.
Using ICIs in those with pre-existing autoimmunity is possible but with risk of causing a disease flare or a different IRAE.
Acknowledgments
Funding sources: Dr. Cappelli is supported by the Jerome L. Greene Foundation Scholar Award. Dr. Shah is supported by grant K23-AR061439. Additional support was provided by a Jerome L. Greene Foundation Discovery Award and by RDRCC P30AR053503
Footnotes
Conflicts of interest: Dr. Bingham has served as a consultant for Bristol-Myers-Squibb.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Shah AA, Casciola-Rosen L, Rosen A. Review: cancer-induced autoimmunity in the rheumatic diseases. Arthritis Rheumatol. 2015;67(2):317–326. doi: 10.1002/art.38928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Schreiber RD, Old LJ, Smyth MJ. Cancer immunoediting: integrating immunity’s roles in cancer suppression and promotion. Science. 2011;331(6024):1565–1570. doi: 10.1126/science.1203486. [DOI] [PubMed] [Google Scholar]
- 3.Rosenberg SA. IL-2: the first effective immunotherapy for human cancer. J Immunol. 2014;192(12):5451–5458. doi: 10.4049/jimmunol.1490019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12(4):252–264. doi: 10.1038/nrc3239. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Brahmer JR, Hammers H, Lipson EJ. Nivolumab: targeting PD-1 to bolster antitumor immunity. Future Oncol. 2015;11(9):1307–1326. doi: 10.2217/fon.15.52. [DOI] [PubMed] [Google Scholar]
- 6.Topalian SL, Drake CG, Pardoll DM. Immune checkpoint blockade: a common denominator approach to cancer therapy. Cancer Cell. 2015;27(4):450–461. doi: 10.1016/j.ccell.2015.03.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Buchbinder EI, McDermott DF. Cytotoxic T-lymphocyte antigen-4 blockade in melanoma. Clin Ther. 2015;37(4):755–763. doi: 10.1016/j.clinthera.2015.02.003. [DOI] [PubMed] [Google Scholar]
- 8.Ivashko IN, Kolesar JM. Pembrolizumab and nivolumab: PD-1 inhibitors for advanced melanoma. Am J Health Syst Pharm. 2016;73(4):193–201. doi: 10.2146/ajhp140768. [DOI] [PubMed] [Google Scholar]
- 9.Brahmer J, Reckamp KL, Baas P, et al. Nivolumab versus Docetaxel in Advanced Squamous-Cell Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373(2):123–135. doi: 10.1056/NEJMoa1504627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Motzer RJ, Escudier B, McDermott DF, et al. Nivolumab versus Everolimus in Advanced Renal-Cell Carcinoma. N Engl J Med. 2015;373(19):1803–1813. doi: 10.1056/NEJMoa1510665. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Postow MA, Chesney J, Pavlick AC, et al. Nivolumab and ipilimumab versus ipilimumab in untreated melanoma. N Engl J Med. 2015;372(21):2006–2017. doi: 10.1056/NEJMoa1414428. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/831/CN-01074831/frame.html. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.NIH. [Accessed December 27, 2015];2015 ClinialTrials.gov website.
- 13.Nghiem PT, Bhatia S, Lipson EJ, et al. PD-1 Blockade with Pembrolizumab in Advanced Merkel-Cell Carcinoma. N Engl J Med. 2016 doi: 10.1056/NEJMoa1603702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Le DT, Uram JN, Wang H, et al. PD-1 Blockade in Tumors with Mismatch-Repair Deficiency. N Engl J Med. 2015;372(26):2509–2520. doi: 10.1056/NEJMoa1500596. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Weber JS, Yang JC, Atkins MB, Disis ML. Toxicities of Immunotherapy for the Practitioner. J Clin Oncol. 2015;33(18):2092–2099. doi: 10.1200/JCO.2014.60.0379. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Naidoo J, Page DB, Li BT, et al. Toxicities of the anti-PD-1 and anti-PD-L1 immune checkpoint antibodies. Ann Oncol. 2015;26(12):2375–2391. doi: 10.1093/annonc/mdv383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Spain L, Diem S, Larkin J. Management of toxicities of immune checkpoint inhibitors. Cancer Treat Rev. 2016;44:51–60. doi: 10.1016/j.ctrv.2016.02.001. [DOI] [PubMed] [Google Scholar]
- 18.Robert C, Schachter J, Long GV, et al. Pembrolizumab versus Ipilimumab in Advanced Melanoma. N Engl J Med. 2015;372(26):2521–2532. doi: 10.1056/NEJMoa1503093. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/119/CN-01083119/frame.html. [DOI] [PubMed] [Google Scholar]
- 19.Wolchok JD, Neyns B, Linette G, et al. Ipilimumab monotherapy in patients with pretreated advanced melanoma: a randomised, double-blind, multicentre, phase 2, dose-ranging study. Lancet Oncol. 2010;11(2):155–164. doi: 10.1016/S1470-2045(09)70334-1. [DOI] [PubMed] [Google Scholar]
- 20.Hodi FS, O’Day SJ, McDermott DF, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–723. doi: 10.1056/NEJMoa1003466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Postow MA. Managing immune checkpoint-blocking antibody side effects. Am Soc Clin Oncol Educ Book. 2015;35:76–83. doi: 10.14694/EdBook_AM.2015.35.76. [DOI] [PubMed] [Google Scholar]
- 22.Weber JS, Kahler KC, Hauschild A. Management of immune-related adverse events and kinetics of response with ipilimumab. J Clin Oncol. 2012;30(21):2691–2697. doi: 10.1200/JCO.2012.41.6750. [DOI] [PubMed] [Google Scholar]
- 23.Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med. 2015;373(1):23–34. doi: 10.1056/NEJMoa1504030. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Kwon ED, Drake CG, Scher HI, et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(7):700–712. doi: 10.1016/S1470-2045(14)70189-5. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/659/CN-00992659/frame.html. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Gibney GT, Kudchadkar RR, DeConti RC, et al. Safety, correlative markers, and clinical results of adjuvant nivolumab in combination with vaccine in resected high-risk metastatic melanoma. Clin Cancer Res. 2015;21(4):712–720. doi: 10.1158/1078-0432.CCR-14-2468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Brahmer JR, Drake CG, Wollner I, et al. Phase I study of single-agent anti-programmed death-1 (MDX-1106) in refractory solid tumors: safety, clinical activity, pharmacodynamics, and immunologic correlates. J Clin Oncol. 2010;28(19):3167–3175. doi: 10.1200/JCO.2009.26.7609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Woodworth T, Furst DE, Alten R, et al. Standardizing assessment and reporting of adverse effects in rheumatology clinical trials II: the Rheumatology Common Toxicity Criteria v.2.0. J Rheumatol. 2007;34(6):1401–1414. [PubMed] [Google Scholar]
- 28.Bronstein Y, Ng CS, Hwu P, Hwu WJ. Radiologic manifestations of immune-related adverse events in patients with metastatic melanoma undergoing anti-CTLA-4 antibody therapy. AJR Am J Roentgenol. 2011;197(6):W992–w1000. doi: 10.2214/AJR.10.6198. [DOI] [PubMed] [Google Scholar]
- 29.Capozzi V, Makhoul S, Aprea E, et al. PTR-MS Characterization of VOCs Associated with Commercial Aromatic Bakery Yeasts of Wine and Beer Origin. Molecules. 2016;21(4) doi: 10.3390/molecules21040483. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Motzer RJ, Rini BI, McDermott DF, et al. Nivolumab for Metastatic Renal Cell Carcinoma: Results of a Randomized Phase II Trial. J Clin Oncol. 2015;33(13):1430–1437. doi: 10.1200/JCO.2014.59.0703. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/593/CN-01074593/frame.html. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Le DT, Lutz E, Uram JN, et al. Evaluation of ipilimumab in combination with allogeneic pancreatic tumor cells transfected with a GM-CSF gene in previously treated pancreatic cancer. J Immunother. 2013;36(7):382–389. doi: 10.1097/CJI.0b013e31829fb7a2. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/236/CN-00918236/frame.html. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Hodi FS, Lee S, McDermott DF, et al. Ipilimumab plus sargramostim vs ipilimumab alone for treatment of metastatic melanoma: a randomized clinical trial. JAMA. 2014;312(17):1744–1753. doi: 10.1001/jama.2014.13943. http://onlinelibrary.wiley.com/o/cochrane/clcentral/articles/960/CN-01021960/frame.html. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Hersh EM, O’Day SJ, Powderly J, et al. A phase II multicenter study of ipilimumab with or without dacarbazine in chemotherapy-naive patients with advanced melanoma. Invest New Drugs. 2011;29(3):489–498. doi: 10.1007/s10637-009-9376-8. [DOI] [PubMed] [Google Scholar]
- 34.Borghaei H, Paz-Ares L, Horn L, et al. Nivolumab versus Docetaxel in Advanced Nonsquamous Non-Small-Cell Lung Cancer. N Engl J Med. 2015;373(17):1627–1639. doi: 10.1056/NEJMoa1507643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Chan MM, Kefford RF, Carlino M, Clements A, Manolios N. Arthritis and tenosynovitis associated with the anti-PD1 antibody pembrolizumab in metastatic melanoma. J Immunother. 2015;38(1):37–39. doi: 10.1097/CJI.0000000000000060. [DOI] [PubMed] [Google Scholar]
- 36.de Velasco G, Bermas B, Choueiri TK. Auto-immune arthropathy and uveitis as complications from PD-1 inhibitor. Arthritis Rheumatol. 2015 doi: 10.1002/art.39406. [DOI] [PubMed] [Google Scholar]
- 37.Sheik Ali S, Goddard AL, Luke JJ, et al. Drug-associated dermatomyositis following ipilimumab therapy: a novel immune-mediated adverse event associated with cytotoxic T-lymphocyte antigen 4 blockade. JAMA Dermatol. 2015;151(2):195–199. doi: 10.1001/jamadermatol.2014.2233. [DOI] [PubMed] [Google Scholar]
- 38.Yoshioka M, Kambe N, Yamamoto Y, Suehiro K, Matsue H. Case of respiratory discomfort due to myositis after administration of nivolumab. J Dermatol. 2015;42(10):1008–1009. doi: 10.1111/1346-8138.12991. [DOI] [PubMed] [Google Scholar]
- 39.Khoja L, Maurice C, Chappell M, et al. Eosinophilic fasciitis and acute encephalopathy toxicity from pembrolizumab treatment of a patient with metastatic melanoma. Cancer Immunol Res. 2016 doi: 10.1158/2326-6066.CIR-15-0186. [DOI] [PubMed] [Google Scholar]
- 40.Goldstein BL, Gedmintas L, Todd DJ. Drug-associated polymyalgia rheumatica/giant cell arteritis occurring in two patients after treatment with ipilimumab, an antagonist of ctla-4. Arthritis Rheumatol. 2014;66(3):768–769. doi: 10.1002/art.38282. [DOI] [PubMed] [Google Scholar]
- 41.Manusow JS, Khoja L, Pesin N, Joshua AM, Mandelcorn ED. Retinal vasculitis and ocular vitreous metastasis following complete response to PD-1 inhibition in a patient with metastatic cutaneous melanoma. J Immunother Cancer. 2014;2(1):41. doi: 10.1186/s40425-014-0041-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Minor DR, Bunker SR, Doyle J. Lymphocytic vasculitis of the uterus in a patient with melanoma receiving ipilimumab. J Clin Oncol. 2013;31(20):e356. doi: 10.1200/JCO.2012.47.5095. [DOI] [PubMed] [Google Scholar]
- 43.Fadel F, El Karoui K, Knebelmann B. Anti-CTLA4 antibody-induced lupus nephritis. N Engl J Med. 2009;361(2):211–212. doi: 10.1056/NEJMc0904283. [DOI] [PubMed] [Google Scholar]
- 44.Iwama S, De Remigis A, Callahan MK, Slovin SF, Wolchok JD, Caturegli P. Pituitary expression of CTLA-4 mediates hypophysitis secondary to administration of CTLA-4 blocking antibody. Sci Transl Med. 2014;6(230):230ra245. doi: 10.1126/scitranslmed.3008002. [DOI] [PubMed] [Google Scholar]
- 45.Klair JS, Girotra M, Hutchins LF, Caradine KD, Aduli F, Garcia-Saenz-de-Sicilia M. Ipilimumab-Induced Gastrointestinal Toxicities: A Management Algorithm. Dig Dis Sci. 2016 Feb 5; doi: 10.1007/s10620-016-4042-4. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 46.Turesson C, Matteson EL. Malignancy as a comorbidity in rheumatic diseases. Rheumatology (Oxford) 2013;52(1):5–14. doi: 10.1093/rheumatology/kes189. [DOI] [PubMed] [Google Scholar]
- 47.Stone JH, Holbrook JT, Marriott MA, et al. Solid malignancies among patients in the Wegener’s Granulomatosis Etanercept Trial. Arthritis Rheum. 2006;54(5):1608–1618. doi: 10.1002/art.21869. [DOI] [PubMed] [Google Scholar]
- 48.Johnston RL, Lutzky J, Chodhry A, Barkin JS. Cytotoxic T-lymphocyte-associated antigen 4 antibody-induced colitis and its management with infliximab. Dig Dis Sci. 2009;54(11):2538–2540. doi: 10.1007/s10620-008-0641-z. [DOI] [PubMed] [Google Scholar]
- 49.Gogas H, Ioannovich J, Dafni U, et al. Prognostic significance of autoimmunity during treatment of melanoma with interferon. N Engl J Med. 2006;354(7):709–718. doi: 10.1056/NEJMoa053007. [DOI] [PubMed] [Google Scholar]
- 50.Gielisse EA, de Boer NK. Ipilimumab in a patient with known Crohn’s disease: to give or not to give? J Crohns Colitis. 2014;8(12):1742. doi: 10.1016/j.crohns.2014.08.002. [DOI] [PubMed] [Google Scholar]
- 51.Bostwick AD, Salama AK, Hanks BA. Rapid complete response of metastatic melanoma in a patient undergoing ipilimumab immunotherapy in the setting of active ulcerative colitis. J Immunother Cancer. 2015;3:19. doi: 10.1186/s40425-015-0064-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Johnson DB, Sullivan RJ, Ott PA, et al. Ipilimumab Therapy in Patients With Advanced Melanoma and Preexisting Autoimmune Disorders. JAMA Oncol. 2015:1–7. doi: 10.1001/jamaoncol.2015.4368. [DOI] [PubMed] [Google Scholar]
- 53.Joseph CG, Darrah E, Shah AA, et al. Association of the autoimmune disease scleroderma with an immunologic response to cancer. Science. 2014;343(6167):152–157. doi: 10.1126/science.1246886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Shah AA, Rosen A, Hummers L, Wigley F, Casciola-Rosen L. Close temporal relationship between onset of cancer and scleroderma in patients with RNA polymerase I/III antibodies. Arthritis Rheum. 2010;62(9):2787–2795. doi: 10.1002/art.27549. [DOI] [PMC free article] [PubMed] [Google Scholar]