
Figure 4. Lymph node core biopsy suspicious of involvement by AITL.
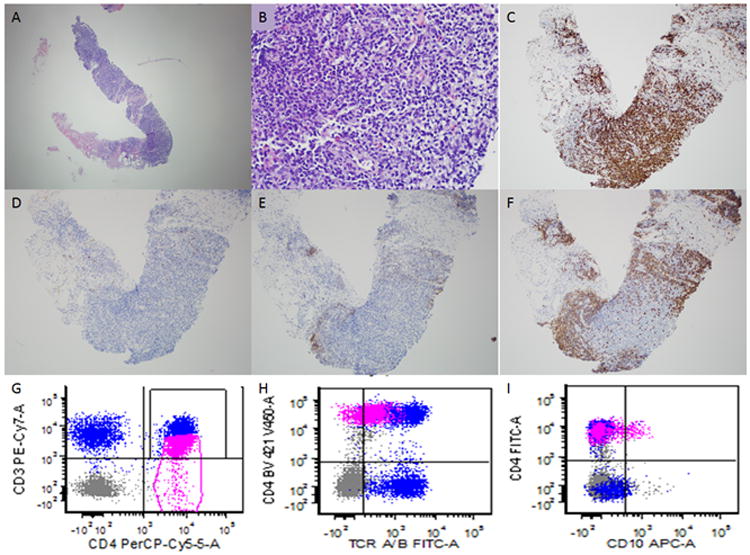
This patient had a previous history of AITL and had undergone chemotherapy. He presented with abdominal lymphadenopathy. A needle core biopsy was performed and minute fragments of tissue were present for evaluation (A). On higher power evaluation occasional atypical appearing lymphoid cells with clear cytoplasm are seen (B) which are present in association with occasional eosinophils. The majority of lymphoid cells are of T-cell lineage as demonstrated by CD3 (C). Rare CD10 positive cells are present (D). A CD21 immunohistochemical (E) stain is mostly negative and only highlights scattered follicular dendritic cells. The anti-CD20 antibody (F) highlights residual B-cell follicles. Although the findings were strongly suspicious for involvement by AITL, it was difficult to establish a definitive diagnosis due to the small nature of the biopsy. Flow cytometric immunophenotyping showed an aberrant T-cell population (shown in pink) with dim CD3 (G) and T-cell receptor alpha/beta expression (H) compared with background non-neoplastic T-cells. A subset of these cells showed aberrant CD10 expression. The flow cytometry results were helpful in establishing a definitive diagnosis. (A-B, hematoxylin and eosin; C-F, immunohistochemistry with hematoxylin counterstain)