
Fig. 2.
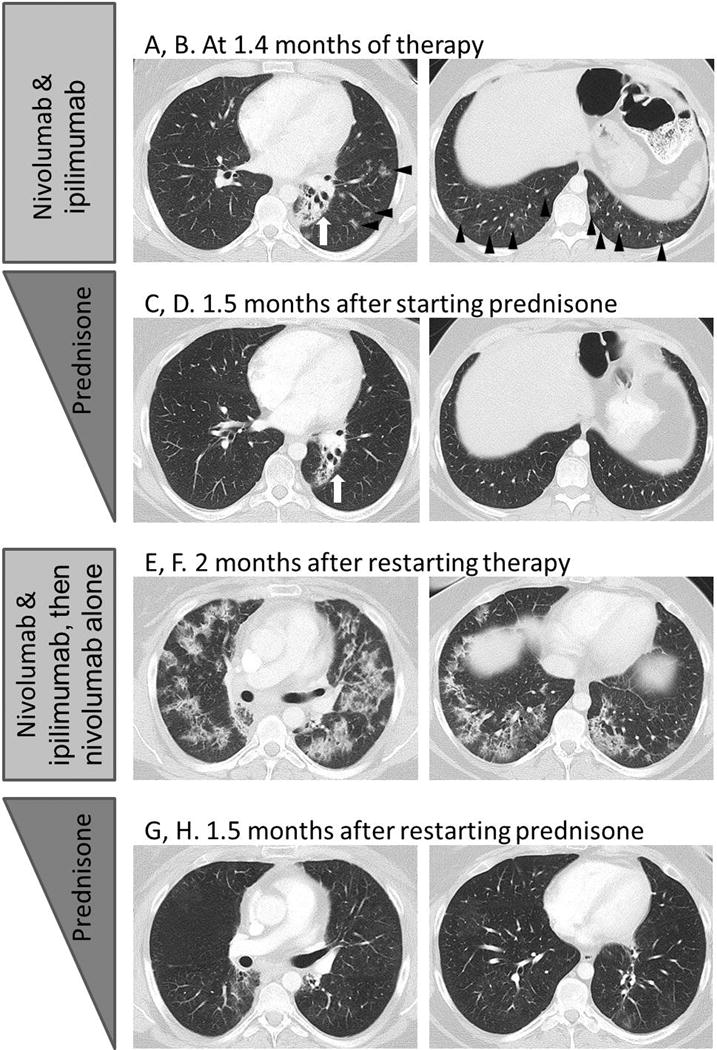
Pneumonitis with a COP pattern in a 33-year-old female with Hodgkin lymphoma treated with nivolumab and ipilimumab combination therapy (Patient 16), with a recurrence during retreatment and two episodes of pneumonitis flare after completion of corticosteroid taper.
A, B. CT scan of the chest at 1.4 months of therapy demonstrated ground-glass and reticular opacities and consolidations with multifocal distribution, indicative of a COP pattern of pneumonitis (arrowheads). Left perihilar opacity and traction bronchiectasis are due to prior radiation therapy (arrows).
C, D. The patient was treated with oral prednisone taper, and the findings have resolved on the follow-up scan performed 1.5 month later.
E, F. The patient restarted therapy and received 2 doses of nivolumab and ipilimumab and 2 doses of nivolmab monotherapy, then developed recurrent pneumonitis after 2 months since restarting therapy. The scan at the time of recurrent pneumonitis demonstrated similar findings with muitifocal ground-glass and reticular opacities and consolidations, again representing a COP pattern. The findings were more extensive than the first episode.
G, H. Nivolumab was held and the patient was treated again with prednisone taper for pneumonitis, with subsequent improvement.