

Abstract
Objective: To develop and test the prototype of a serious digital game for improving community-dwelling older adults' heart failure (HF) knowledge and self-management behaviors. The serious game innovatively incorporates evidence-based HF guidelines with contemporary game technology.
Materials and Methods: The study included three phases: development of the game prototype, its usability assessment, and evaluation of the game's functionality. Usability testing included researchers' usability assessment, followed by research personnel's observations of participants playing the game, and participants' completion of a usability survey. Next, in a pretest–post-test design, validated instruments—the Atlanta Heart Failure Knowledge Test and the Self Care for Heart Failure Index—were used to measure improvement in HF self-management knowledge and behaviors related to HF self-maintenance, self-management, and self-efficacy, respectively. A postgame survey assessed participants' perceptions of the game.
Results: During usability testing, with seven participants, 100%, 100%, and 86% found the game easy to play, enjoyable, and helpful for learning about HF, respectively. In the subsequent functionality testing, with 19 participants, 89% found the game interesting, enjoyable, and easy to play. Playing the game resulted in a significant improvement in HF self-management knowledge, a nonsignificant improvement in self-reported behaviors related to HF self-maintenance, and no difference in HF self-efficacy scores. Participants with lower education level and age preferred games to any other medium for receiving information.
Conclusion: It is feasible to develop a serious digital game that community-dwelling older adults with HF find both satisfying and acceptable and that can improve their self-management knowledge.
Keywords: : Games, Heart failure, Self-management
Introduction
The American Heart Association estimates that the number of U.S. residents with heart failure (HF) may increase by 46% in 2030 and that 2 million of those with HF will then be over age 80.1 HF is the most common diagnosis among hospitalized patients aged 65 years or older.2,3 To reduce hospitalizations and mortality, HF clinical guidelines therefore advocate effective HF self-management.4–6 However, recent large-scale studies of interventions designed to support patients' HF self-management have failed to demonstrate reduced mortality or hospital admissions.7–9 Older adults find it difficult to attain proficiency in HF self-management because it requires them to become adept in a wide range of skills on a daily basis within the context of their disease as well as comorbidities.10 There is an urgent need to find effective, portable, and scalable tools that can empower older adults with HF to improve their self-management.
One new exciting avenue to foster effective self-management skills in older individuals with HF is offered by digital health games. Such games can provide flexible, accessible, and appealing educational environments within which patients can learn about self-management of their disease by seeking information, practicing skills, and receiving social support.11–13 Systematic reviews have found videogames to be helpful for education and positive reinforcement, resulting in participants' increased knowledge14 and improved self-management.15
To our knowledge, although digital game playing has been associated with significant positive effects on physical health outcomes of older adults,16 no serious digital game has yet been developed to improve HF self-management-related knowledge and behaviors specifically with older adults as the target audience. In this article, we present a Heart Health game prototype—an application for mobile tablets—and we assess the game's usability and evaluate its functionality for improving HF self-management knowledge and behaviors among community-dwelling older adults with HF.
Materials and Methods
Approval for this feasibility study was obtained from the Institutional Review Boards of The University of Texas at Austin (#: 2014-07-0022) and St. David's Healthcare System. The study consisted of three phases: development of the game prototype, assessment of its usability, and evaluation of the game's functionality.
Participant inclusion criteria
Participants, 55 years or older, who were fluent in English, diagnosed with HF, and with minimal cognitive and physical impairment, were recruited from three outpatient HF clinics and a safety net health center in central Texas during the summer of 2015. Safety net health centers are federally qualified health centers that deliver healthcare to medically underserved and uninsured populations. The clinical staff at the clinics and health center obtained contact information of participants who were interested in the study and provided it to the research team. Potential participants were then screened for eligibility on the phone using home health screening questionnaires from the Medicare-mandated Outcome and Assessment Information Set (OASIS).17 Screening criteria included a score of <1 (alert and oriented or requiring prompting only under stressful or unfamiliar conditions) on the OASIS item for cognitive functioning and <2 (able to independently walk without a device or using a cane or walker) on the item for ambulation/locomotion. The inclusion criteria were similar for participants recruited to the usability assessment and functionality evaluation phases of the study as well.
Study phase 1: Development of the game prototype
In prior research, older adults were found to prefer digital games that were casual (i.e., digital games intended for mass audiences) or that were associated with traditional familiar games.18 In addition, to efficiently capture the preferences of a wide range of older adult patients within a short time, we conducted an open-ended survey about providers' awareness of patient preferences for electronic games with 34 nurses from a home health agency and the safety net health center during their monthly meetings. We selected a casino slot game for our game prototype because this genre ranked among the top three preferred game genres in the survey and is a casual game that resembles traditional casino slot machines.
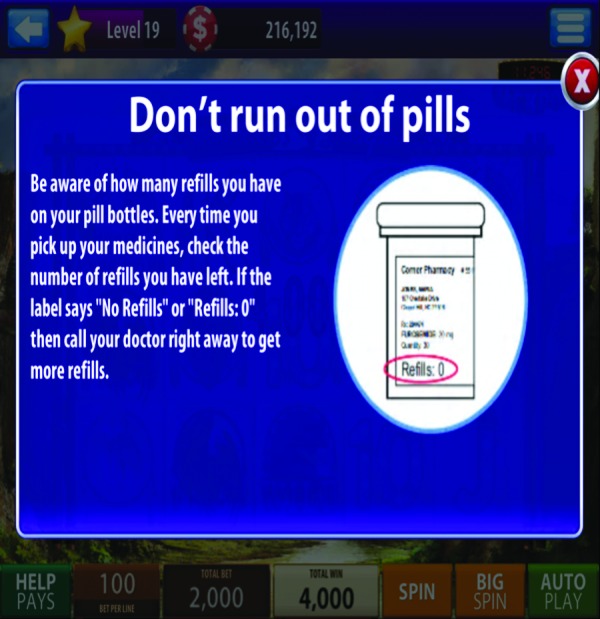
An interdisciplinary team of academic specialists in nursing, computer game programming, usability science, and health communication from The University of Texas at Austin School of Nursing, Game and Multimedia Applications Program, School of Information, and Moody College of Communication then collaborated with a central Texas-based game company (Bee Cave Games, Inc.) to develop the prototype of a serious digital game for HF self-management. The game company's existing casino slot game was repurposed as an HF game version for the iOS platform (Table 1 and Fig. 1). HF self-management education content from the Heart Failure Society of America's5 evidence-based guidelines and the Living with Heart Failure booklet,19 which is tailored to low literacy levels, was incorporated throughout the game, using game-based learning and Gagne's established instruction strategies20 (Table 2 and Fig. 2). The game presented content on HF self-management skills in the following order: (1) introduction to HF, (2) medications, (3) diet modification (e.g., low-sodium diet) and fluid restriction (e.g., 1500 mL/day), (4) physical activity modification (e.g., walk for 30 minutes/day), and (5) daily symptom checks (e.g., swelling, increase in weight, shortness of breath) and related responses.
Table 1.
Characteristics of a Videogame for Health (Heart Health)
| Health topic(s) | HF self-management |
| Targeted age group(s) | 50+ years |
| Other targeted group characteristics | Living in the community/not hospitalized |
| Short description of game idea | Play a casino slot game to learn about HF self-management |
| Target player(s) | Individual |
| Guiding knowledge or behavior change theory(ies), models, or conceptual framework(s) | Gagne's learning principles |
| Intended health behavior changes | HF self-management, self-maintenance, and self-confidence to manage HF-related diet, physical activity, medication, symptom monitoring, and crisis recognition |
| Knowledge element(s) to be learned | HF self-management in the domains of diet, physical activity, medication, symptom monitoring, and crisis recognition |
| Behavior change procedure(s) (taken from Michie inventory) or therapeutic procedure(s) employed | Improved knowledge reinforced through a feedback and reward mechanism will motivate behavior change |
| Clinical or parental support needed? | None |
| Data shared with parent or clinician | No |
| Type of game | Casual, educational |
| Story (if any) | None |
| Synopsis (including story arc) | None |
| How the story relates to targeted behavior change | NA |
| Game components | |
| Player's game goal/objective(s) | To earn points to continue playing the casino slot game |
| Rules | Play the slot game and read the educational messages, which were interspersed between betting on the slots, answer challenges, and reminder questions, to earn extra points to continue playing the casino slot game |
| Game mechanic(s) | Select amount of points to bet to play the casino slots. Earn additional point based on answers to challenge questions and reminders |
| Procedures to generalize or transfer what is learned in the game to outside the game | Use of evidence-based educational material that was tailored to low health literacy level, and use of images to illustrate the learning points. For example: Image on how to read sodium content in a grocery nutrition label was included in the educational messages |
| Virtual environment | |
| Setting (describe) | Four different rooms to play casino slot games with different graphical backgrounds in each room |
| Avatar | None |
| Game platform(s) needed to play the game | Tablet |
| Sensors used | None |
| Estimated play time | 45 minutes |
HF, heart failure.
FIG. 1.

Heart health game.
Table 2.
Gagne's Nine Events of Instruction
| 1. Gain attention |
| 2. Inform learners of objectives |
| 3. Stimulate recall of prior learning |
| 4. Present the content |
| 5. Provide learning guidance |
| 6. Elicit performance (practice) |
| 7. Provide feedback |
| 8. Assess performance |
| 9. Enhance retention and transfer to the job |
FIG. 2.
Game content.
In addition, to promote HF self-management-related knowledge and behaviors, the game incorporated basic game design elements such as game rules, leveling up, and a feedback and reward/incentive system based on participants' responses to quiz questions on the HF self-management content (Fig. 3). As an incentive designed to motivate players to repeatedly engage with the content, the casino slot game provided opportunities for HF patients to earn additional betting chips if they made correct responses to the content-related questions. Incorrect responses were followed by the presentation of relevant content on the specific HF self-management skill and repetition of the content-related questions. In addition, appropriate HF self-management-related behaviors were encouraged with daily reminder tips and questions on adherence of the HF self-management skills of sodium restriction (diet), medication adherence, physical activity, and symptom checks (Fig. 4).
FIG. 3.
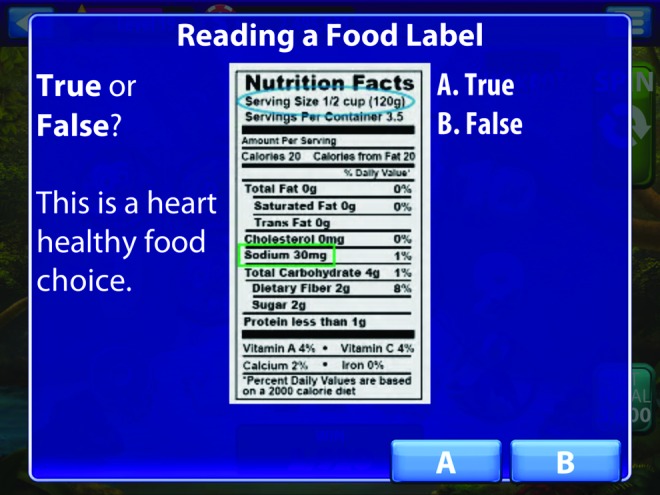
Miniquiz.
FIG. 4.
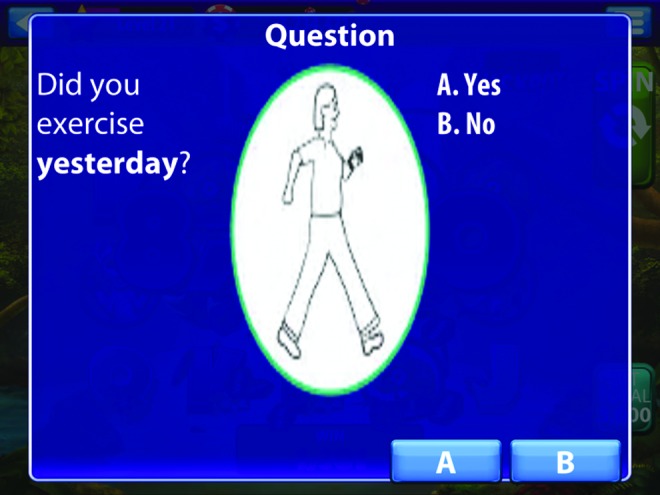
Reminders.
Study phase 2: Assessment of the game's usability
The game prototype was developed iteratively in several rounds, with its usability assessed first by researchers and then through observations of participating users by a trained graduate research assistant (GRA). During the initial rounds of development, four research team members from nursing and computer game programming assessed the game's usability by playing the game themselves; they then modified the game to improve its usability and make it senior friendly. Font size was increased, and the visual contrast was heightened. The placement of quizzes and reminders within the game was also adjusted to improve the game's flow. During this first part of phase 2, the game's playtime was estimated to be about 45 minutes to an hour, after which the content and the quiz questions were cyclically repeated.
Two rounds of usability assessment were then conducted with older adult HF participants, during which the GRA observed the participants while they played the game in their homes for about 30 minutes. The GRA noted his observations on a Microsoft Excel checklist, which consisted of tasks related to playing the game and system-related event descriptions from the instrument of Serious Game Usability Evaluator.21 We then modified the technical glitches that were identified in the checklist.
The participants also completed a usability survey based on the 4-item interest/enjoyment subscale of the Intrinsic Motivation Inventory (alpha = 0.8),22 a multidimensional instrument intended to assess participants' subjective experience related to a target activity. The interest/enjoyment subscale assesses one's interest and inherent pleasure in performing a specific activity.
Study phase 3: Evaluation of the game's functionality
A pre-/post-test study design was then used to evaluate the impact of the digital game on participants' HF self-management-related knowledge and behaviors. Participants played the digital game on an iPad, which they were allowed to keep for 4 weeks. In this phase, after the GRA provided initial training to the participants during the first visit, the participants played the game on their own without any research personnel's supervision.
Participants' knowledge of HF self-management was evaluated using the validated 30-item Atlanta Heart Failure Knowledge Test (AHFKT)23 (α = .84), which measures change in knowledge among HF patients in response to an intervention. Items in the instrument measure knowledge about HF disease process, diet, and nutrition (including sodium and fluid restriction), medications, symptoms, and behaviors (e.g., daily weighing and physical activity). Each correct answer is scored as 1 point, with no additional weighting of items; correct responses are then summed. Incorrect or skipped questions are awarded 0 points. Total scores range from 0 to 30.
The 22-item validated Self-Care of Heart Failure Index (SCHFI)24 (α = .76) was used to evaluate dimensions of HF self-management behaviors on three separate scales: self-maintenance, self-management, and self-efficacy. Scores on each scale range from 0 to 100, with higher scores reflecting better self-care.25 Scores of 70 or greater on each SCHFI scale indicate adequate self-care.25
Participants' pretest responses on both the AHFKT and SCHFI instruments were collected before they received the iPad and again at the end of the 4 weeks. In addition, the participants completed an initial demographic survey and a postgame survey on their perceptions about playing the game. Game data on number of times the game was played, number of spin times for the slots, and total game-playing time for each participant were also collected.
Data analysis
Participants completed all the surveys on Qualtrics software, version 08/2015,26 an online survey administration tool. Statistical software SPSS v21 was used to evaluate the data. Descriptive statistics were used for participants' demographics and game-playing data, as well as their responses on the usability and postgame surveys. Participants' responses on the two instruments for HF self-management knowledge and behaviors were evaluated using paired t-tests. Finally, correlations were identified for participants' demographics, game-playing data, and responses on the HF self-management knowledge and behavior instruments and the postgame survey.
Results
Of 57 potential participants who were approached for the study, 27 (47%) consented to participate. Seven participated in the usability assessment (U1 to U7), and 20 participated in the functionality evaluation (F1 to F20). One of those 20 (F17) was unable to complete the post-test evaluation, owing to hospitalization.
Phase 2: Game usability assessment
Participants in the usability assessment were seven community-residing older adults with HF. The majority were female, Caucasian, and 60–69 years old (Table 3). Only two had a college degree. The GRA observation notes on these participants as they played the game identified technical glitches related to unexplained cessation of background music, lack of increase in the game's level number, lack of consistency in the location of spin buttons across game rooms, small text size, redundant buttons, unclear labeling of the buttons, and duration between spins. All these glitches in the casino slot game were then modified.
Table 3.
Demographic Characteristics
| Game study phase | ||||
|---|---|---|---|---|
| Characteristic | Usability testing (n = 7) | Participant IDs | Functionality testing (n = 19) | Participant IDs |
| Age (years) | ||||
| 50–59 | 1 | U1 | 5 | F7, F9, F13, F18, F20 |
| 60–69 | 5 | U2, U3, U5, U6, U7 | 3 | F8, F11, F14 |
| 70–79 | 0 | — | 5 | F1, F5, F10, F12, F15 |
| 80–89 | 1 | U4 | 4 | F3, F4, F16, F19 |
| >90 | 0 | — | 2 | F2, F7 |
| Gender (n) | ||||
| Males | 3 | U1, U5, U6 | 17 | F2 to F9, F11 to F16, F18 to F20 |
| Females | 4 | U2 to U4, U7 | 2 | F1, F10 |
| Race/ethnicity (n) | ||||
| White | 4 | U1, U3, U4, U7 | 16 | F1 to F7, F10, F12 to F16, F18 to F20 |
| Nonwhite | 3 | U2, U5, U6 | 3 | F8, F9, F11 |
| Education Level | ||||
| Kindergarten to eighth grade | 0 | — | 3 | F1, F10, F11 |
| Some high school, no diploma | 2 | U5, U6 | 1 | F8 |
| High school graduate, diploma, or equivalent [e.g., General Educational Development (GED)] | 1 | U1 | 4 | F7, F9, F13, F15 |
| Some college credit, no degree | 2 | U2, U4 | 4 | F4, F5, F14, F20 |
| Trade/technical/vocational training | 0 | — | 1 | F18 |
| Associate degree | 0 | — | 1 | F12 |
| Bachelor degree | 2 | U3, U7 | 2 | F2, F6 |
| Graduate degree | 0 | — | 3 | F3, F19, F16 |
| Duration of HF diagnosis (years) | ||||
| <2 | — | — | 1 | F10 |
| 2 to 5 | — | — | 7 | F2, F3, F8, F11, F12 F16, F18 |
| 6 to 10 | — | — | 0 | — |
| >10 | — | — | 11 | F1, F4 to F7, F9, F13, F14, F15, F19, F20 |
| HF hospitalizations in the past 12 months (n) | ||||
| 0 | — | — | 6 | F3, F7, F12, F14, F16, F20 |
| 1 to 2 | — | — | 7 | F1, F2, F4, F5, F10, F15, F19 |
| >3 | — | — | 5 | |
| Missing | — | — | 1 | F9 |
| Played computer games before (n) | ||||
| Yes | — | — | 11 | F2, F3, F5, F7, F10, F12, F13, F14, F18, F19, F20 |
| No | — | — | 8 | F1, F4, F6, F8, F9, F11, F15, F16 |
Almost all the participants in the usability assessment found the game interesting, enjoyable, and easy to play (Table 4). Positive and critical comments on the game by the participants during this phase are provided in Table 5. Positive comments mainly addressed the game's usefulness in providing tips, reminders, and information for those with less education or with a recent HF diagnosis. Many critical comments were related to participants' lack of preference for games or digital media and to the slot game's repetitiveness.
Table 4.
Usability Results from the Usability and Functionality Testing Phases of the Study
| Usability parameters | Usability testing phase (n = 7) | Participant ID | Functionality testing phase (n = 19) | Participant ID |
|---|---|---|---|---|
| Interesting, n (%) | 6 (86) | U2 to U7 | 17 (89) | F1, F3 to F16, F18, F19 |
| Easy, n (%) | 7 (100) | U1 to U7 | 18 (94) | F1, F3 to F16, F18 to F20 |
| Enjoyable, n (%) | 7 (100) | U1 to U7 | 15 (79) | F1, F3 to F11, F13, F14, F15, F18, F19 |
| Satisfaction with sound, n (%) | 5 (71) | U2, U3, U4, U6, U7 | 15 (79) | F1, F3 to F11, F14 to F16, F18, F19 |
| Satisfaction with graphics, n (%) | 7 (100) | U1 to U7 | 18 (94) | F1, F3 to F16, F18, F19 |
| Satisfaction with game play (e.g., miniquiz; earning points; moving up levels), n (%) | 6 (86) | U2 to U7 | 15 (79) | F1, F3 to F11, F13 to F15, F18, F19 |
| Satisfaction with content/information, n (%) | 6 (86) | U2 to U7 | 15 (79) | F1, F3 to F11, F13 to F15, F18, F19 |
Table 5.
Participants' Comments on Playing the Digital Game for HF Management
| Positive themes (participant ID) | Critical themes (participant ID) |
|---|---|
| Gameplay “Interesting way to learn about HF” (U3, U4) “Easy to play” (F9) |
Lack of interest or trust in games or digital media “I do not play games and have little interest in playing them” (F12) |
| “Very satisfying, relaxes your mind, I rather play game than read” (F11) “Relaxing had fun, entertaining” (F8) |
“do not like computers” (F2, F4) “Prefer paper or brochure” (U2, U3, F16, F15) |
| “Earning more points helped” (F8, F11) | “HF serious subject…not a game” (U1) |
| “Graphics … presented in a fun way” (F6) | “Would want info from qualified medical persons” (U7, F6) |
| Reminders | Repetitiveness |
| “Reminders are helpful as you get older and forgetful” (U6) “Enjoyed it, been helpful in reminding me.” (F1) “Game was helpful especially through reminders on salt.” (U6) |
“not a big “slots player …repetitiveness, got tedious after a short while” (F5) “I didn't feel the repetition helped all that much. I'd rather read” (F14, F17) “It worked fine and was educational; however, the spinning and stopping buttons was monotonous” (U7) |
| Educational | Content |
| “The tips were good to know” (U3) “Informative” (U1, U3, U5, F4) “Enjoyed game … great for refresher info … can see how it would be a huge benefit for ‘older/younger’ folks.” (F6) |
“Need more information on the topics mentioned” (U1, U2, U3, U6, U7, F15) “Need more quiz questions” (U3, U5, F6) |
| “This was a very good refresher for me. That is, getting the info via a game.” (F19) | |
| “Education is always helpful” (U7) | |
| “Feel like I needed the information” (F10, F17, F18) | |
| “The tips reinforced what I already do.” (U1) | |
| “Useful for patients with less education” (U6) | |
| “Game good for novice HF person, who has no information on HF. Good pointers in there for such people” (F2, F6) | |
| “I think it was a good idea overall. I did learn a couple of points I had not realized before, especially about SALT.” (F15) | |
| Gameplay | |
| “Need to earn real money” (F11) |
Phase 3: Game functionality evaluation
Participants in the game's functionality testing were 19 community-residing older adults with HF. The majority were male, Caucasian, older than 70 years, and diagnosed with having HF for more than 10 years (Table 3). Fourteen of these participants did not have a college degree; eight were educated at the high school level or less. Thirteen had been hospitalized at least once for HF-related reasons in the past 12 months. Eleven had played computer games before.
During the functionality evaluation, 8 of the 19 participants played the game 5 times or more, 11 played the game for 2 hours or more, and 15 were able to play the game without assistance from family members or friends (Table 6). Seventeen of the 19 participants indicated that they would recommend the game to others with HF (Table 6). In addition, participants with lower education levels (p = 0.01) and age (p = 0.01) significantly preferred the digital game to any other medium for receiving information on HF self-management. Finally, among all 19 participants, playing the game improved HF self-management knowledge significantly from pretest to post-test (p = 0.007) (Table 7). The highest improvement in correct answers, with increases in scores of 8 to 10 points, occurred on questions related to medication and diet management. Playing the game also resulted in a nonsignificant improvement in HF self-maintenance on the SCHFI from pretest to post-test (p = 0.11), but did not result in any difference in HF self-efficacy scores. We were unable to evaluate scores on the self-management subscale, which requires participants to be symptomatic of HF exacerbation during the past 3 months; in this study, only 6 of the 19 participants (F1, F2, F4, F5, F8, F18) reported HF-related symptoms for that time. In the postgame survey, 15 participants reported that playing the digital game motivated them to engage in HF self-management behaviors (Table 5). Other demographic or game-playing data showed no correlation with changes in knowledge or self-management scores on the instruments.
Table 6.
Participant Perceptions on Game for HF Self-Management Knowledge and Behaviors
| Post-test survey items | Agreement | Participant ID |
|---|---|---|
| Played the game without assistance, n (%) | 15 (79) | F2, F3, F5 to F9, F11, F12, F14 to F16, F18 to F20 |
| Prefer the digital game to other media for receiving HF information, n (%) | 11 (58) | F1, F3, F5, F8 to F11, F13, F14, F18, F19 |
| (a) Correlation with age | r = 0.61 (p = 0.006) | |
| (b) Correlation with education level | r = 0.57 (p = 0.011) | |
| Promoted learning of, n (%) | ||
| (a) HF condition | 17 (89) | F1, F3 to F16, F18, F19 |
| (b) HF medications | 15 (79) | F3 to F5, F7 to F15, F18 to F20 |
| (c) Diet | 17 (89) | F3 to F16, F18 to F20 |
| (d) Physical activity | 17 (89) | F3 to F16, F18 to F20 |
| (e) Symptom monitoring | 18 (95) | F1, F3 to F16, F18 to F20 |
| (f) When to follow-up with healthcare providers | 17 (89) | F1, F3 to F16, F18, F19 |
| Game Motivated me to, n (%): | ||
| (a) Salt restriction | 16 (84) | F3 to F7, F9 to F16, F18 to F20 |
| (b) Physical activity | 15 (79) | F3 to F8, F10 to F16, F18, F19 |
| (c) Medication management | 16 (84) | F3 to F8, F10 to F16, F18, F20 |
| (d) Daily symptom monitoring checks | 16 (84) | F3 to F8, F10 to F16, F18 to F20 |
| (e) When to follow-up with healthcare providers | 16 (84) | F3 to F15, F18 to F20 |
| Will recommend the game to others with HF, n (%) | 17 (89) | F1, F3 to F16, F18, F19 |
| Average # of times game was played | 9.7 (range: 3–66) | — |
| Average of total game-playing time (in minutes) | 237 (range: 12–1298) | — |
Table 7.
Functionality Results: HF Self-Management Knowledge and Behavior Scores
| Scores | Pretest mean (SD) | Post-test mean (SD) | p |
|---|---|---|---|
| Knowledge (n = 19) | 22.26 | 25.00 | 0.007 |
| Self-maintenance (n = 19) | 31.1 | 33.1 | 0.11 |
| Self-management (n = 6) | 16.8 | 14.3 | 0.07 |
| Self-confidence (n = 19) | 18.31 | 18.36 | 0.95 |
Discussion
This feasibility study demonstrates that serious digital games can be satisfying and acceptable to community-dwelling older adults with HF. To our knowledge, this is the first serious game developed specifically for HF self-management with older adults as the target audience. Collaboration between industry and academia enabled us to repurpose an existing commercial game as a serious health game for self-management that was both esthetically pleasing and visually sophisticated despite the constraints of limited time and resources.
Two other studies have evaluated serious games for cardiac conditions among adults.27,28 One of those studies evaluated a game for hypertension management, finding no significant difference in blood pressure reduction between control and intervention groups.27 However, blood pressure reduction within the intervention group was found to be statistically and clinically significant over time. In the other study, a serious game—The Heart Game—was developed to assist heart patients in telerehabilitation, incorporating gamification principles such as competition, the use of leaderboards, and the inclusion of a close relative.28 Participants in that study reported that the game motivated them to engage in their daily cardiac rehabilitation activities. Both of these studies, along with ours, suggest that serious digital games offer a promising approach to health management for patients with cardiac diseases. However, future studies must demonstrate the efficacy of serious digital games for improved health outcomes such as quality of life and healthcare utilization among patients with cardiac disorders.
Although this study and its results are exploratory, they do suggest several lessons. The HF self-management content was tailored to a low literacy level so that the game would be accessible and understandable for all participants. Improvement of HF knowledge was noteworthy since more than half of the participants had suffered from chronic HF for more than 10 years. However, more highly educated participants expressed disappointment with the game's amount of information and repetitiveness. Future games could explore mechanisms to deliver health-related content tailored to the health literacy of players to sustain their engagement.
In the postintervention survey, participants reported that the game motivated them to modify HF-related self-management behaviors. However, the rewards and incentives were internal to the game and did not correspond to real-life behaviors. Game feedback and rewards that correspond to real-life behaviors might be a stronger strategy for behavior modification. Incorporation of constructs from behavioral science theories (e.g., the transtheoretical stages of change model29,12 or self-determination theory30), along with objective monitoring of behaviors (e.g., physical activity) and health parameters (e.g., heart rate and blood pressure), could help bridge the gap between the game environment and the real world. These would provide both intrinsic and extrinsic motivation. In addition, game mechanisms could incorporate collaboration and peer social support among participants to sustain their engagement.30
Of course, some older adults may not prefer games or digital media as a health management tool. Indeed, 7 of 26 participants did not prefer games or digital media, including one participant (F2) who experienced exacerbation of arthritis in his fingers and faced difficulty operating the tablet computer's touch screen. Although it is important to respect older adults' game-playing preferences and abilities, effective training and improved usability of digital games might help increase their acceptability,31 as we observed among the remaining older adult participants who played the digital game.
Limitations
The study was limited by its small sample size, lack of a control group, and short follow-up time of 4 weeks. The short follow-up prevented assessment of any sustained or long-term retention of HF self-management knowledge. Participants' stage of HF disease was not assessed as participants were not aware of their HF stage, and this is a limitation of this study. A higher proportion of our study participants were males, were educated at the high school or lower level, and had experienced more hospitalizations than those indicated in prior epidemiological profiles of HF patients.1,32,33 The study might have suffered from selection bias because participation was voluntary and because participants who had experienced a high number of hospitalizations might have been especially motivated to participate. Low female enrollment could have been due to women's roles as caregivers even in the presence of a chronic disease, which could be a barrier to participation.34 Reliance on participants' self-reports regarding their HF self-management behaviors was also a limitation of this study.
Conclusion
The development of a serious game prototype that is acceptable to community-dwelling older adults with HF and that can improve their knowledge of HF self-management is clearly feasible. Future studies should explore the impact of game-based learning strategies and game-motivated behavior modification on improving older adults' HF outcomes, including self-management behaviors, rehospitalizations, and quality of life.
Acknowledgments
Research reported here was supported by the National Institute of Nursing Research of the National Institutes of Health under Award Number P30NR015335 (PI Kim). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. The authors gratefully acknowledge the support received from The University of Texas Austin's new faculty start-up funds. Editorial support with manuscript development was provided by the Cain Center for Nursing Research and the Center for Transdisciplinary Collaborative Research in Self-management Science (P30, NR015335) at The University of Texas at Austin School of Nursing. The authors gratefully acknowledge the support received from the staff at St. David's Heart Failure Clinic, Austin Heart Hospital, Texas Heart and Vascular Center, and The Family Wellness Center. The authors gratefully acknowledge the support received from the staff at Bee Cave Games, Inc., Austin, TX.
Author Disclosure Statement
No competing financial interests exist.
References
- 1.Mozaffarian D, Benjamin EJ, Go AS, et al. . Heart disease and stroke statistics—2016 update: A report from the American Heart Association. Circulation 2016; 133:e38–e60 [DOI] [PubMed] [Google Scholar]
- 2.Fitch K, Pelizzari PM, Pyenson B. Inpatient utilization and costs for Medicare fee-for-service beneficiaries with heart failure. Am Health Drug Benefits 2016; 9:96–104 [PMC free article] [PubMed] [Google Scholar]
- 3.Ross JS, Chen J, Lin Z. Recent national trends in readmission rates after heart failure hospitalization. Circ Heart Fail 2010; 3:97–103 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Lainscak M, Blue L, Clark AL, et al. . Self-care management of heart failure: Practical recommendations from the Patient Care Committee of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2011; 13:115–126 [DOI] [PubMed] [Google Scholar]
- 5.Heart Failure Society of America, Lindenfeld J, Albert NM, et al. . HFSA 2010 Comprehensive heart failure practice guideline. J Card Fail 2010; 16:e1–e194 [DOI] [PubMed] [Google Scholar]
- 6.Yancy CW, Jessup M, Bozkurt B, et al. . 2013 ACCF/AHA guideline for the management of heart failure: A report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013; 62:e147–e239 [DOI] [PubMed] [Google Scholar]
- 7.Cockayne S, Pattenden J, Worthy G, et al. . Nurse facilitated self-management support for people with heart failure and their family carers (SEMAPHFOR): A randomised controlled trial. Int J Nurs Stud 2014; 51:1207–1213 [DOI] [PubMed] [Google Scholar]
- 8.Jaarsma T, van der Wal MH, Lesman-Leegte I, et al. . Effect of moderate or intensive disease management program on outcome in patients with heart failure: Coordinating study evaluating outcomes of advising and counseling in heart failure (COACH). Arch Intern Med 2008; 168:316–324 [DOI] [PubMed] [Google Scholar]
- 9.Powell LH, Calvin JE, Jr., Richardson D, et al. . Self-management counseling in patients with heart failure: The heart failure adherence and retention randomized behavioral trial. JAMA 2010; 304:1331–1338 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Riegel B, Lee CS, Dickson VV. Self care in patients with chronic heart failure. Nat Rev Cardiol 2011; 8:644–654 [DOI] [PubMed] [Google Scholar]
- 11.Beale IL, Kato PM, Marin-Bowling VM, et al. . Improvement in cancer-related knowledge following use of a psychoeducational video game for adolescents and young adults with cancer. J Adolesc Health 2007; 41:263–270 [DOI] [PubMed] [Google Scholar]
- 12.Thompson D, Baranowski T, Buday R, et al. . Serious video games for health: How behavioral science guided the development of a serious video game. Simul Gaming 2010; 41:587–606 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.McGonigal J. Reality Is Broken: Why Games Make Us Better and How They Can Change the World. New York: Penguin; 2011 [Google Scholar]
- 14.Theng YL, Lee JW, Patinadan PV, Foo SS. The use of videogames, gamification, and virtual environments in the self-management of diabetes: A systematic review of evidence. Games Health J 2015; 4:352–361 [DOI] [PubMed] [Google Scholar]
- 15.Charlier N, Zupancic N, Fieuws S, et al. . Serious games for improving knowledge and self-management in young people with chronic conditions: A systematic review and meta-analysis. J Am Med Inform Assoc 2016; 23:230–239 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Hall AK, Chavarria E, Maneeratana V, et al. . Health benefits of digital videogames for older adults: A systematic review of the literature. Games Health J 2012; 1:402–410 [DOI] [PubMed] [Google Scholar]
- 17.Madigan EA, Fortinsky RH. Interrater reliability of the outcomes and assessment information set: Results from the field. Gerontologist 2004; 44:689–692 [DOI] [PubMed] [Google Scholar]
- 18.Cota TT, Ishitani L. Motivation and benefits of digital games for the elderly: A systematic literature review. Rev Bras Comp Aplicada 2015; 7:2–16 [Google Scholar]
- 19.DeWalt DA, Malone RM, Bryant ME, et al. . A heart failure self-management program for patients of all literacy levels: A randomized, controlled trial [ISRCTN11535170]. BMC Health Serv Res 2006; 6:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Gagne RM. The Conditions of Learning and Theory of Instruction. 4th ed. New York: Holt, Rinehart & Winston; 1985 [Google Scholar]
- 21.Moreno-Ger P, Torrente J, Hsieh YG, Lester WT. Usability testing for serious games: Making informed design decisions with user data. Adv Hum-Comput Interact 2012; 2012:369637 [Google Scholar]
- 22.McAuley E, Duncan T, Tammen VV. Psychometric properties of the Intrinsic Motivation Inventory in a competitive sport setting: A confirmatory factor analysis. Res Q Exerc Sport 1989; 60:48–58 [DOI] [PubMed] [Google Scholar]
- 23.Reilly CM, Higgins M, Smith A, et al. . Development, psychometric testing, and revision of the Atlanta Heart Failure Knowledge Test. J Cardiovasc Nurs 2009; 24:500–509 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Vellone E, Riegel B, Cocchieri A, et al. . Psychometric testing of the Self-Care of Heart Failure Index Version 6.2. Res Nurs Health 2013; 36:500–511 [DOI] [PubMed] [Google Scholar]
- 25.Riegel B, Lee CS, Dickson VV, Carlson B. An update on the Self-Care of Heart Failure Index. J Cardiovasc Nurs 2009; 24:485–497 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Qualtrics software, Version 08/2015. Qualtrics, Provo, UT. www.qualtrics.com (accessed September20, 2016)
- 27.Hickman RL, Jr., Clochesy JM, Pinto MD, et al. . Impact of a serious game for health on chronic disease self-management: Preliminary efficacy among community dwelling adults with hypertension. J Health Hum Serv Adm 2015; 38:253–275 [PubMed] [Google Scholar]
- 28.Dithmer M, Rasmussen JO, Grönvall E, et al. . “The Heart Game”: Using gamification as part of a telerehabilitation program for heart patients. Games Health J 2016; 5:27–33 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Prochaska JO, Butterworth S, Redding CA, et al. . Initial efficacy of MI, TTM tailoring and HRI's with multiple behaviors for employee health promotion. Prev Med 2008; 46:226–231 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Deci EL, Ryan RM. The “what” and “why” of goal pursuits: Human needs and the self-determination of behavior. Psychol Inquiry 2000; 11:227–268 [Google Scholar]
- 31.Fisk AD, Rogers WA, Charness N, Czaja SJ, Sharit J. Designing for Older Adults: Principles and Creative Human Factors Approaches. 2nd ed. Boca Raton, FL: CRC Press; 2009 [Google Scholar]
- 32.Wong CY, Chaudhry SI, Desai MM, Krumholz HM. Trends in comorbidity, disability, and polypharmacy in heart failure. Am J Med. 2011; 124:136–143 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Gheorghiade M, Peterson ED. Improving postdischarge outcomes in patients hospitalized for acute heart failure syndromes. JAMA 2011; 305:2456–2457 [DOI] [PubMed] [Google Scholar]
- 34.Navaie-Waliser M, Feldman PH, Gould DA, et al. . When the caregiver needs care: The plight of vulnerable caregivers. Am J Pub Health 2002; 92:409–413 [DOI] [PMC free article] [PubMed] [Google Scholar]