
Figure 1. Images and schematic drawings of each anastomosis during APLT in the rat and postoperative appearance of the graft and native liver.
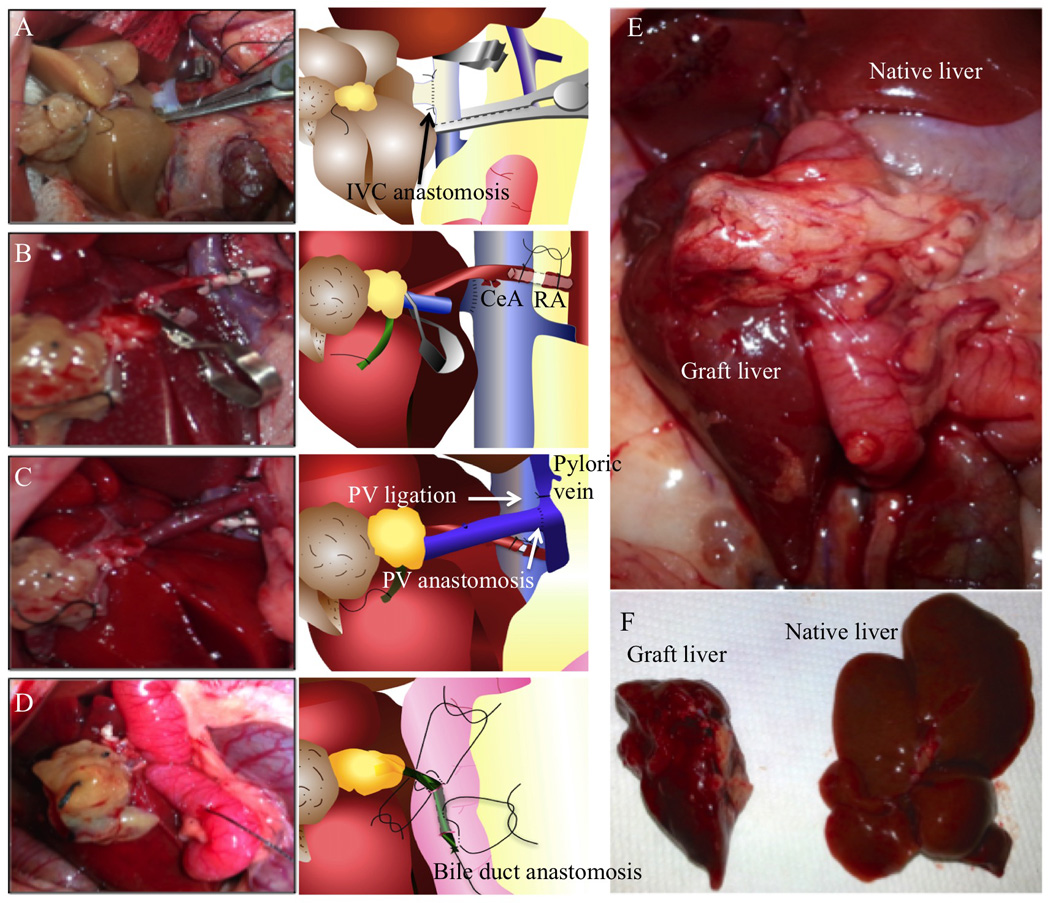
(A) IVC anastomosis. After clamping the proximal and distal ends of the IHIVC, the anterior wall of the IHIVC was cut to make a 7 mm vertical incision, as close to the ligated right renal vein as possible, for the IVC anastomosis. A stay suture was placed with 10-0 nylon at the distal end before beginning the continuous suture. Prior to completion of the anastomosis, saline was injected slowly using a L-shaped injector into the IHIVC anastomosis to remove any air trapped inside. (B) Arterial anastomosis. The thread tied to the right RA was held and pulled to the left side of the recipient. The proximal side of the right RA was clamped and the anterior wall of the artery cut with scissors and the blood inside the artery washed out. Then, the arterial stent tied on the graft celiac artery was inserted into the recipient’s right RA. The arterial stent was ligated in place with 7-0 silk to complete the arterial anastomosis. (C) PV anastomosis. The inside of the graft PV was washed and 2 stay sutures placed from outside to inside on each edge of the graft SMV using 10-0 nylon. The superior mesenteric artery (SMA) was clamped during PV anastomosis to minimize intestinal congestion. The splenic vein, the PV and SMV were clamped, to provide space for the anastomosis. The PV was cut about 4 mm on the opposite side of the splenic vein for anastomosis. An end-to-side anastomosis was performed between the graft SMV and the recipient’s PV. (D) Bile duct reconstruction. A small stitch was placed on the duodenal wall and on the right side wall of the graft bile duct close to the hilum using 10-0 nylon. Then, another small stitch was placed from the duodenum to the left side of the bile duct, 2 mm proximal to the previous suture. A 24-gauge needle was inserted into the duodenum 1 cm distal from the sutures and exited from the duodenal lumen between the sutures to introduce the bile duct into the duodenum. The anterior wall of the bile duct was then cut to create an opening for bile drainage. The bile duct was pulled with the bile duct opening inside the duodenum to avoid bile leakage and the 10-0 sutures tied to connect the duodenum and the bile duct. One Lembert suture was placed on the duodenum to close the insertion hole from the 24-gauge needle. (E) Appearance of the graft and native livers in situ 4 weeks after surgery. The liver graft has regenerated well and is similar macroscopically to the native liver. (F) Appearance of the liver graft (left) and native liver (right) following excision 4 weeks after surgery.