
Figure 1.
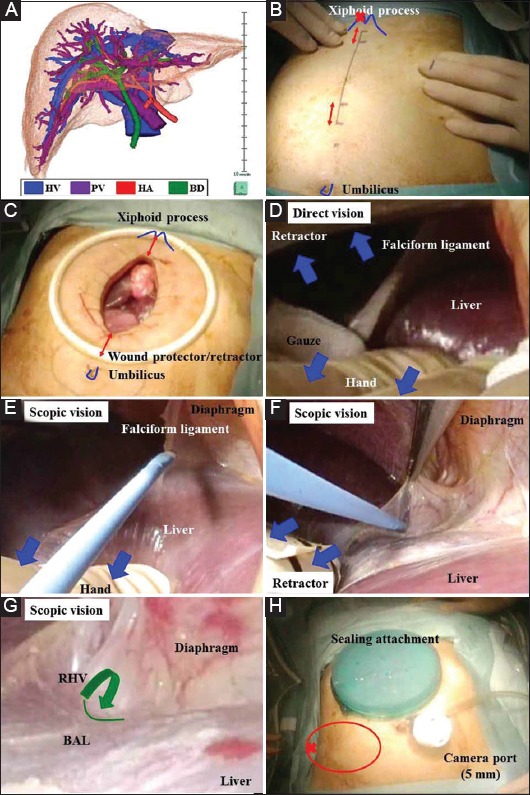
(A) A three-dimensional image that articulates the vessels (i.e., hepatic vein, portal vein, and hepatic artery) and biliary duct in an all-in-one package should be made preoperatively. (B) An 8-cm mark is made along the midline from a point 2 cm below the xiphoid process. Several 2-cm incisions from the upper and lower sides of the midline incision are added if needed (red arrows). To expose the bare area of the liver in the right subphrenic area in pure laparoscopic surgery or a hybrid technique, a working port should be placed as far toward the head side as possible (red cross). (C) The midline incision is protected and retracted by a wound attachment. (D) Direct vision alone may provide an inadequate surgical field. Adequate retraction of the liver is performed (blue arrows). (E) Scopic vision provides an excellent surgical field for cutting of the falciform ligament and (F) dissection around the right hepatic vein. (G) Scopic vision provides a magnified view. The division between the right and middle hepatic veins is detected (green line) and dissected through the anterior wall of the inferior vena cava (green arrow). (H) The wound is sealed with a gel-type attachment. The camera port is placed at the umbilicus, and a working port is placed at the right lateral wall (red circle). To expose the bare area of the liver at the right subphrenic area in either pure laparoscopic surgery or a hybrid technique, a working port should be placed as far toward the lateral-dorsal side as possible (red cross) BAL, bare area of the liver; BD, biliary duct; HA, hepatic artery; HV, hepatic vein; PV, portal vein; RHV, right hepatic vein