
Figure 2.
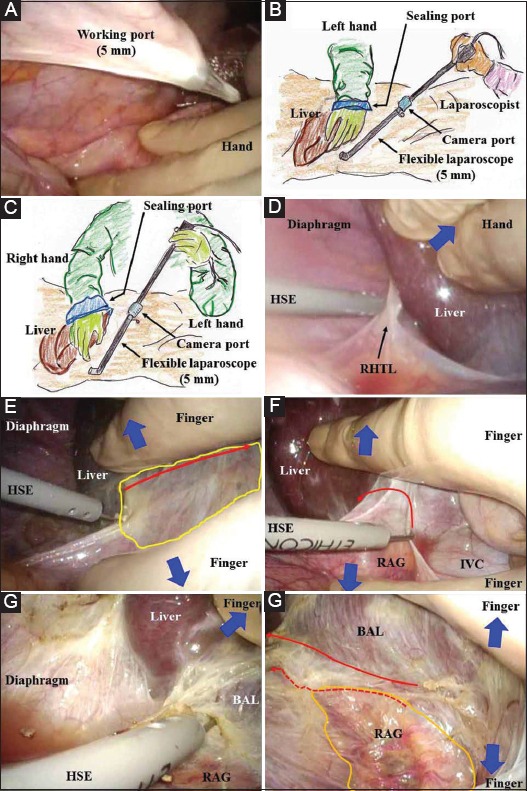
(A) The intra-abdominal organs should be guarded by the surgeon’s hand during port placement. (B) The left hand is inserted into the abdomen via a sealing port in situations where both a surgical and laparoscopic assistant are present. (C) If the assistant surgeon is well educated and greatly experienced, his or her right hand is inserted via a sealing port to retract the liver, and a flexible laparoscope is then manipulated only by the left hand. A more coordinated surgical field with a magnified view will thus be obtained. (D) The right hepatic triangular ligament is cut by a hook-shaped electrode under liver retraction (blue arrow). To expose the bare area of the liver in the right subphrenic area, a working port is placed as far toward the lateral-dorsal side as possible. (E) Delicate and detail-oriented retraction/countertraction is performed with the finger, and general and rough retraction/countertraction is performed with the hand (blue arrows). The pressure of pneumoperitoneum helps to create a dissectible/cuttable layer by marked infiltration of carbon dioxide gas (yellow area). The retroperitoneum is intentionally cut near the liver (red arrow). (F) The retroperitoneum around the right adrenal gland and inferior vena cava is cut near the liver (red arrow) under the countertraction (blue arrows) and tension created by a hook-shaped electrode. (G) The bare area of the liver is exposed. (H) The retroperitoneum is cut near the liver (solid arrow), not near the right adrenal gland (dotted arrow). The right adrenal gland should be carefully saved with a membrane capsule (orange area) BAL, bare area of the liver; HSE, hook-shaped electrode; IVC, inferior vena cava; RAG, right adrenal gland; RHTL, right hepatic triangular ligament