
Figure 3.
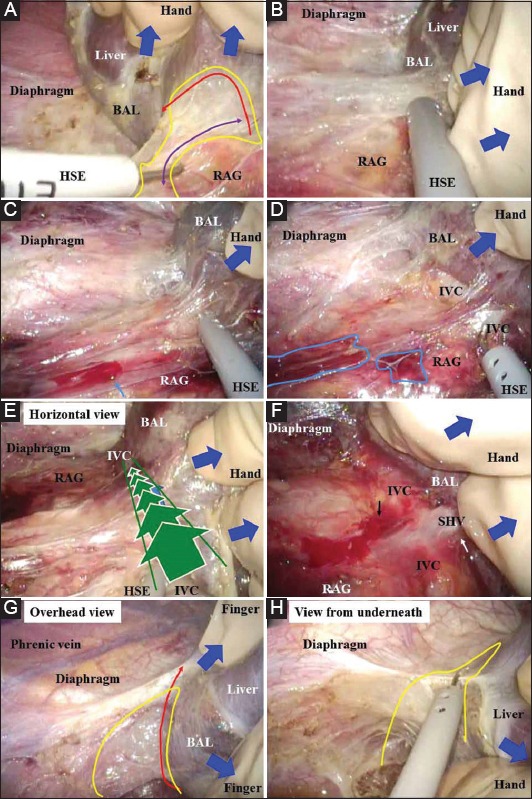
(A,B) A dissectible/cuttable layer should be created (yellow area). An adequately wide layer is confirmed with a reciprocating hook (purple arrow) and is cut near the liver (red arrow). (C,D) Even slightly careless retraction/countertraction of the liver may easily result in hemorrhage and/or oozing around the right adrenal gland (aqua arrow and areas). (E) Delicate and detail-oriented retraction/countertraction is performed with the finger, and general and rough retraction/countertraction is performed with the hand (blue arrows). The horizontal view via the laparoscope provides an excellent view along the inferior vena cava (green arrows). The surgical field essentially spreads to the foreground via the laparoscope (green lines). (F) The lateral wall of the inferior vena cava is bared, and then short hepatic veins and the hepatocaval ligament can be skeletonized. Even slightly careless retraction/countertraction will easily result in hemorrhage and/or oozing around the inferior vena cava (black arrow). (G) From an overview provided by laparoscopic vision, the liver is removed from the diaphragm without any injury to the liver or phrenic veins (blue arrows). The bare area of the liver is adequately exposed. The dissectible/cuttable layer is very wide (yellow area) and is intentionally cut as close to the liver as possible (red arrow). (H) The view from underneath also provides an excellent field for cutting a dissectible/cuttable layer (yellow area) BAL, bare area of the liver; HSE, hook-shaped electrode; IVC, inferior vena cava; RAG, right adrenal gland; SHV, short hepatic vein