
Figure 4.
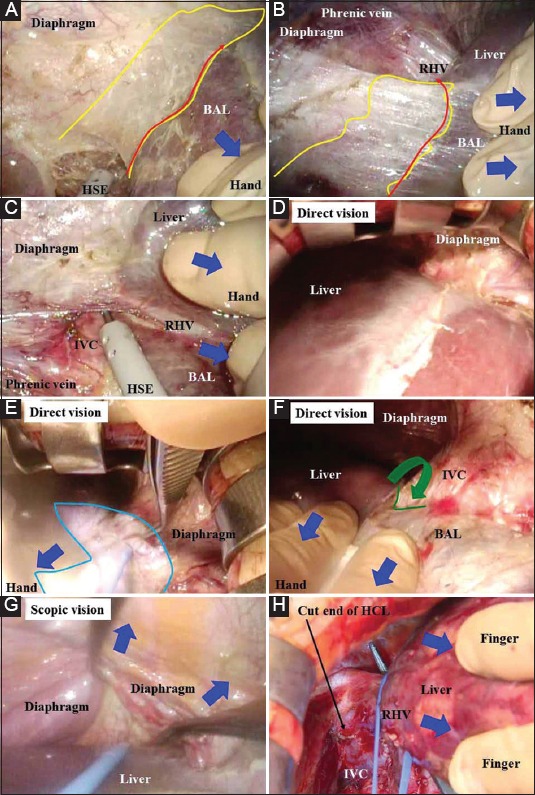
(A,B) Simultaneous retraction/countertraction with a hand or finger (blue arrows) and marked infiltration of carbon dioxide gas that created pneumoperitoneal pressure worked well to create a dissectible/cuttable layer (yellow areas). Because this layer was so wide, it was intentionally traced as close to the liver as possible during dissection (red arrows). (C) According to the process of exposure of the bare area of the liver, the walls of the inferior vena cava and right hepatic vein are carefully detected. (D) Direct vision also provides a good surgical field for right hepatic vein detection if a 2-cm extensional incision is made below the xiphoid process. (E) Direct vision requires focal lighting (aqua area). (F) The division between the right hepatic vein and middle hepatic vein is detected (green line) and dissected (green arrow). (G) The cut ends around the right hepatic vein from the central and right sides are connected via scopic vision because direct vision provides only a limited view under the right subphrenic space. (H) The hepatocaval ligament is cut, and the inferior vena cava wall and extrahepatic margin of the right hepatic vein are bared. The right hepatic vein is then skeletonized BAL, bare area of the liver; HSE, hook-shaped electrode; IVC, inferior vena cava; RHV, right hepatic vein