
Figure 6.
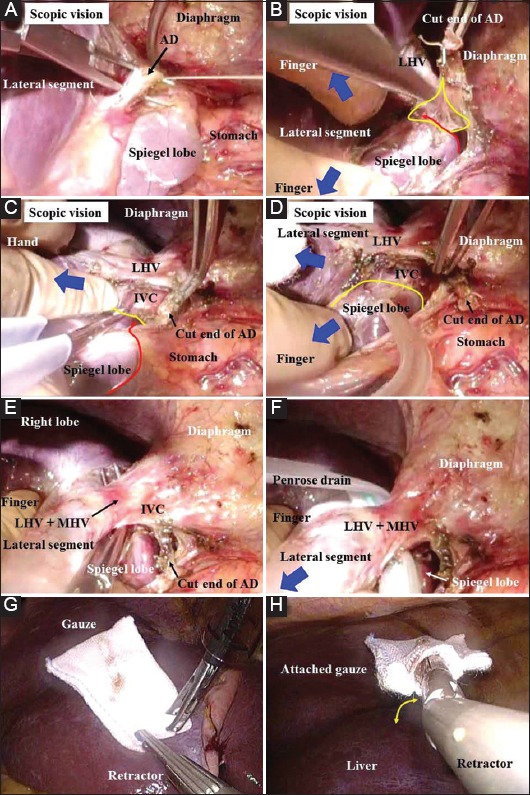
(A) Arantius’ duct is ligated and then cut. (B-D) Delicate and detail-oriented retraction/countertraction is performed with the finger, and general and rough retraction/countertraction is performed with the hand (blue arrows). The connective tissues should be completely dissected (yellow area). The membrane around Spiegel’s lobe is cut (red line), and the upper side of this lobe is completely bared (yellow line). The pinch-burn-cut technique works well. (E) The inferior vena cava wall is bared sufficiently at the upper side of Spiegel’s lobe. The extrahepatic margin of the common channel of the left and middle hepatic veins is also skeletonized. (F) This common channel is hanged with a Penrose drain. (G) For a hybrid technique/pure laparoscopic surgery, specialized gauze is prepared for retraction/countertraction of the liver. (H) An articulated fan-shaped retractor attached to specialized gauze is employed for a hybrid technique/pure laparoscopic surgery. This device is bendable (yellow arrow) AD, Arantius’ duct; IVC, inferior vena cava; LHV, left hepatic vein; MHV, middle hepatic vein