
Fig. 1. A 60-year-old man with a right frontal glioblastoma, undergoing his second operation 16 months after the first operation.
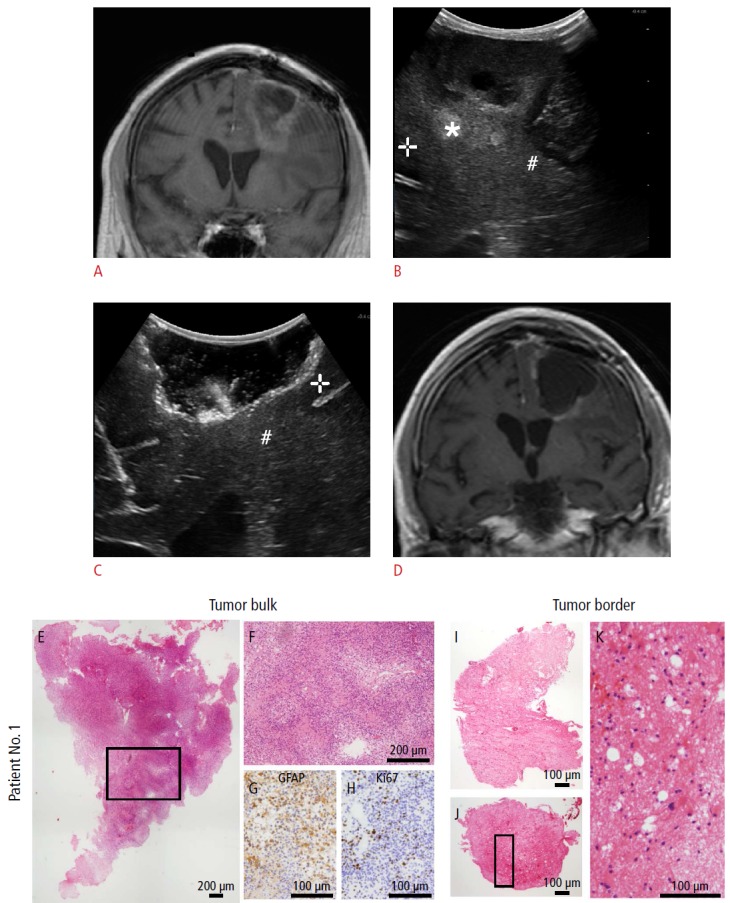
A. Coronal magnetic resonance imaging (MRI) (T1, contrast-enhanced) defines the extent of tumor recurrence. B. Intraoperative ultrasonography (IOUS) before tumor resection (coronal image) reveals hypoechoic (+) as well as intermediate hypoechoic (#) and hyperechoic tissue (*). C. Coronal IOUS shows the extent of resection; at the border, a hypoechoic gyrus can be identified (+). The region where sample 2 was taken (indistinguishable to the surgeon’s eye between border or normal tissue) is marked (#). D. The postoperative coronal MRI (T1, contrast-enhanced) taken at the day after resection shows only linear contrast media enhancement. E-K. Histopathological examination demonstrated that the hyperechoic lesion contained cell-rich solid tumor (tumor bulk) (E-H), whereas in the intermediate tissue, infiltrating tumor cells and necrosis were found (tumor border) (I-K).