
Figure.
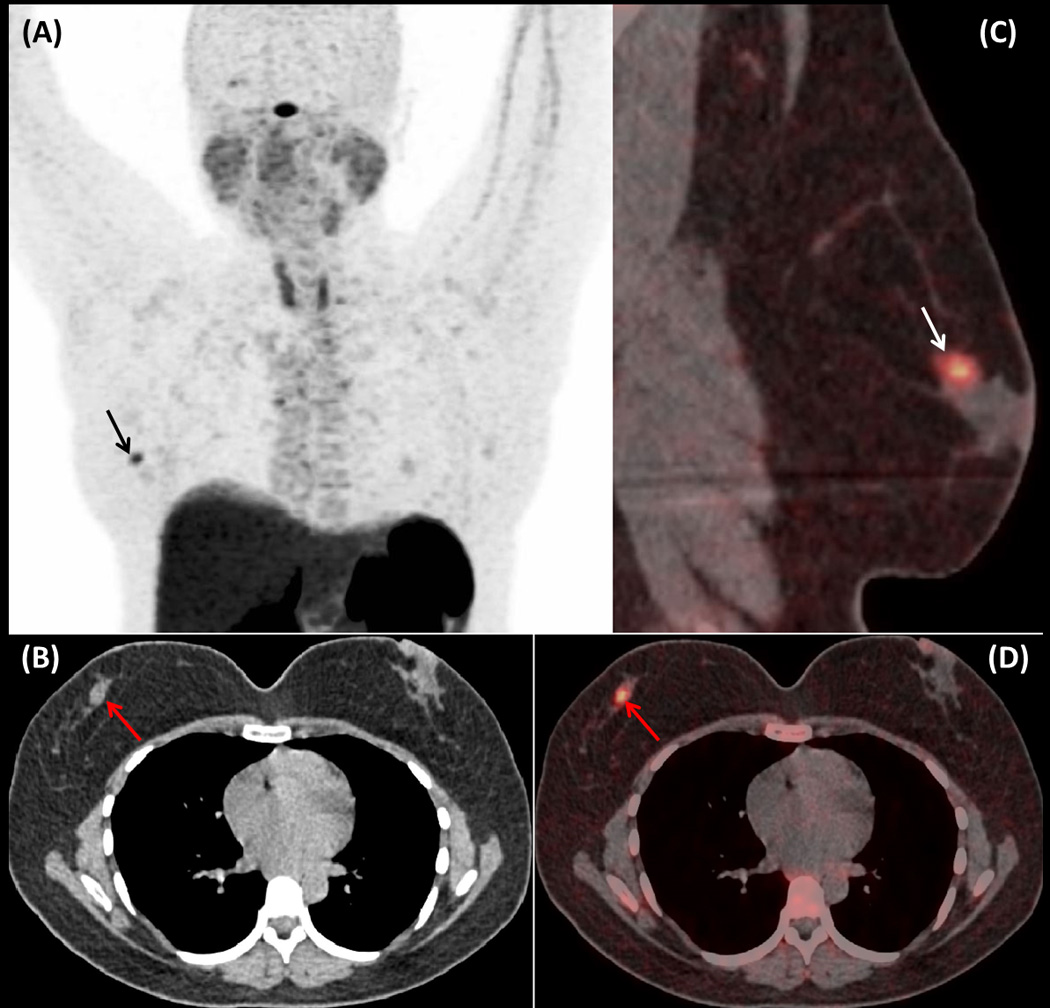
A 37 year-old woman with history of well-differentiated carcinoid tumor of the rectum that was successfully resected with no evidence of recurrence on consecutive imaging studies, was referred to our institute for further follow-up. The patient was evaluated with whole-body PET/CT scan using 68Ga-DOTATATE for the detection of metastatic neuroendocrine tumor (NET) lesions, which showed a focus of mildly increased activity (SUVmax: 5,2) (Fig 1A: maximum intensity projection (MIP) image; arrow) in the right breast corresponding to a soft tissue density residing adjacent to the areola, on its supra-lateral aspect (Fig1B: axial CT image of the chest; arrow) (Fig. 1C &D: sagittal and axial fused 68Ga-DOTATATE PET/CT images; arrows). Due to patient’s elevated levels of chromogranin-A (499ng/ml), and episodes of flushing and shortness of breath, suspicion of metastatic NET lesion was raised and excisional biopsy of the breast lesion was performed revealing a fibroadenoma.
Fibroadenoma is the most commonly encountered benign tumor of the breast displaying admixture of stromal and epithelial proliferation [1]. Typically fibroadenoma presents as a painless, firm, well-defined, solitary tumor. However, multiple fibroadenomas may be present in up to 15% of patients in the same or in both breasts (10% of patients). On ultrasound fibroadenomas usually appear with, uniformly distributed internal echoes, enabling differentiation from cysts [2]. On contrast-enhanced computed tomography (CT) fibroadenomas present as non specific well-circumscribed, homogeneously enhancing masses without associated nipple retraction or skin thickening and may demonstrate “popcorn like” calcifications [3]. On contrast enhanced MR imaging, these tumors are typically hypointense on T1-weighted and hyperintense on T2-weighted images, with considerable variation of signal intensity based on the amount of fibrous tissue they contain [4]. Usually, breast fibroadenomas present no or low-level activity on 18F-FDG PET indicating very low cell proliferation. However, increased 18F-FDG uptake can be observed in the presence of fibrocystic changes, atypical ductal hyperplasia, or ductal ectasia [5, 6].
The conjunction of newer generation somatostatin (SST) analogues with the chelator DOTA-, enabled labelling with the PET-emitter gallium-68 (68Ga), allowing somatostatin receptors (SSTRs) imaging with positron emission tomography (PET). The produced compounds present higher affinity to SSTRs compared to diethylenetriaminepentaacetic acid (DTPA)–octreotide used in conventional SSTR-imaging with single photon emission computed tomography (SPECT) [7]. Moreover, the vastly superior resolution provided by PET/CT scanners, the capability of imaging within 60 minutes post radiotracer administration, and the lower radiation dose compared to conventional SSTR-imaging with 111In, have made SSTR imaging using 68Ga-DOTA-conjugated-peptides the new standard of reference for the detection and characterization of NETs and other SSTR-positive lesions [7–9]. The presented case of a biopsy proven breast fibroadenoma with increased 68Ga-DOTATATE activity suggests cell surface over-expression of SSTRs and particularly SSTR-2 for which 68Ga-DOTATATE has a predominant affinity. This finding is consistent with existing data in the literature [10] and highlights the need for correlation with patient’s history and additional imaging modalities for 68Ga-DOTATATE positive breast lesions, which could erroneously be considered as metastatic lesions especially in the setting of patients with history of neuroendocrine malignancy.