

Abstract
Background
It is generally understood that Fine Particulate Matter (PM2.5) can cause high blood pressure. However, it remains unclear whether there is a relationship between the elemental composition of PM2.5 and cardiovascular disease in emergency department patients.
Methods
Crossover design for time stratified cases and conditional logistic regression were used to analyze the correlation between emergency admissions for cerebral hemorrhage, cerebral infarction, TIA (Transient ischemic attack), coronary heart disease and PM2.5, concentrations of chemical element compositions, and Particulate Matter 10 (PM10) in Changsha city.
Results
When the temperature, atmosphere pressure, maximum wind speed, NO2 and SO2 were adjusted, the OR (Odd Ratio) of cerebral hemorrhage was 1.177 [95% confidence interval (CI): 1.006-1.376, p = 0.04] with every10 μg/m3 increase of PM2.5. PM10 was unrelated to cardiovascular emergencies (p > 0.05). In addition, with each additional IQR (Interquartile Range) increase of Ni, Zn and Pb concentrations in PM2.5, the values of OR were 1.826 (95% CI: 1.031-3.233), 1.568 (95% CI: 1.015-2.423) and 1.682 (95% CI: 1.010-2.800), respectively.
Conclusions
Concentration rises of nickel, zinc and lead elements for PM2.5 in Changsha city were related to the increase of emergency admissions with cerebral hemorrhage.
Keywords: Cerebral hemorrhage, Emergency admission, Fine particulate matter, Hypertension
INTRODUCTION
The latest survey data show that there are approximately 254 million patients with hypertension in China,1 and hypertensive patients have a high incidence of stroke.2,3 Studies have shown that fine particulate matter (PM2.5) is an important underlying component for people suffering from high blood pressure and could induce and aggravate cardiovascular and cerebrovascular diseases, and even affect average life expectancy.4-6 Clinical observation have found that short-term exposure to high concentrations of PM2.5 would elevate blood pressure, increase heart rate variability (HRV), induce arrhythmia, aggravate congestive heart failure and stimulate complications such as atherosclerosis, ischemic heart disease and stroke, leading to increased morbidity and mortality of cardiovascular diseases.7-10 PM2.5 is a complex compound, and the biological effects and toxicity of PM2.5 with different chemical compositions are significantly distinct.11 Current evidence has shown that elevated levels of PM2.5 are associated with an increase in emergency admissions for hypertension.12 However, the impact of the concentration changes for major elemental composition of PM2.5 on hypertension and the emergency admissions of the associated cardiovascular diseases require further investigation.
The purpose of this study was to investigate the correlation between PM2.5 and its chemical elemental composition, and emergency admissions for cardiovascular diseases in Changsha, which may provide further evidence for targeted interventions.
MATERIAL AND METHODS
Data on emergency admission
Data obtained upon emergency admission were from medical records of the Third Xiangya Hospital of Central South University, including daily data of the emergency admissions for hypertensive patients with cardiovascular diseases from June 1, 2009 to October 31, 2009. Specific characteristics of these emergency cases included sex, age, treatment department, hospital department, diagnosis and home address of the patients. Classification of diseases was performed according to the International Classification of Diseases, 10th edition coding (ICD-10), and cerebrovascular diseases (ICD-10: I60-70) were collected and classified. Cerebral hemorrhage and cerebral infarction cases were diagnosed by CT or MRI. The Third Xiangya Hospital of Central South University is located in the Yuelu District of Changsha city, which was the area’s largest 3A hospital. The information collected in this study was derived from the local residents as well as long-term foreign residents in this area, who comprised a certain representation for data analysis on emergency admission for cardiovascular diseases and PM2.5 exposure in the area. This study was approved by the hospital’s Ethics Committee.
Meteorological and air pollution data
Meteorological data were collected from routine monitoring by the Changsha Municipal Meteorological Bureau and Central South University. Daily average concentrations of sulfur dioxide (SO2), nitrogen dioxide (NO2) and PM10 in Changsha during the study period were obtained from the Public Weather Information Service website of Changsha City (http://www.csqx.com/). Meteorological data (average daily temperature, average daily relative humidity, daily average barometric pressure and daily maximum wind speed) were downloaded from the International Meteorological website (http://www.wunderground.com/, monitoring points: Huanghua Airport). The PM2.5 concentration monitoring and main chemical element composition analysis method were consistent with a previous study.13 The PM2.5 monitoring location was 3 kilometers (KM) from the hospital environment monitoring points. The sample acquisition time was from June 1, 2009 to October 31, 2009, and PM2.5 samples were collected by PQ200 Ambient Fine Particulate Sampler (BGI Incorporated, Waltham, MA, USA) during the study to establish mass and concentration database of the daily average of PM2.5. Analysis of PM2.5 elemental composition was performed by Energy Dispersive X-Ray Fluorescence (EDXRF) spectrometer ED 2000 (Oxford Instruments, UK). The contents of the chemical composition for the particulate matter in PM2.5 sample were analyzed, in which 18 kinds of chemical elements were measured, including Sodium (Na), magnesium (Mg), aluminium (Al), silicon (Si), phosphorus (P), sulfur (S), potassium (K), calcium (Ca), titanium (Ti), manganese (Mn), iron (Fe), nickel (Ni), copper (Cu), zinc (Zn), lead (Pb), vanadium (V), arsenic (As) and chromium (Cr). These 18 kinds of elements were further used to establish the mass and concentration database of the chemical elements.
Cross study for cases
This study referred to the report of Guo et al.12 in the literature. Case crossover design was used to compare the cardiovascular disease risk in the case period to that in the control period, and to examine the differences in air pollutant exposure that can be used to explain the differences in the daily number of cases. The controls and cases were matched by the day of the week, which could control any weekly patterns in emergency admission and air pollution levels.
Hysteresis effect
Due to the time lag effect of an atmospheric pollutant concentration increase on emergencies with hypertension and its related cardiovascular diseases, emergency situations of hypertension and other cardiovascular diseases on day 0, 2 and 4 after PM2.5 and PM10 concentration alterations were observed in the study. The PM concentration on the day of the incident was considered as the pollutant concentration of lag 0d, while the PM concentration on day 2 or day 4 before the incident was considered as the pollutant concentration of lag 2d or lag 4d. Generally, the optimal lag was determined according to the maximum effect value (OR).
Statistical analysis
Spearman’s correlation analysis and conditional logistic regression model were used in this study, with the daily emergency visits of hypertension and its related cardiovascular diseases taken as a weight, and the Cox regression of SPSS 17.0 (SPSS Inc, Chicago, Illinois, USA) software used to fit. Furthermore, the exposure odds ratio (OR) of the total PM2.5 concentration and its elemental composition concentration in the illness period and control period of emergency cases with hypertension and its related cardiovascular diseases each day were analyzed. The possible impact of the daily meteorological factors (temperature, pressure and maximum wind speed) for the selected PM2.5 on cardiovascular diseases was taken into account as covariates. The air temperature, barometric pressure and maximum wind speed as well as PM2.5 were introduced into regression to perform a single pollutant model study, while correcting NO2 and SO2 to study multiple pollution models.
RESULTS
Trends for time changes of atmospheric pollutants, meteorological factors and cardiovascular emergencies
The daily average concentration of PM2.5 from June 1, 2009-October 31, 2009 was 87.79 μg/m3 for PM2.5, and 93.96 μg/m3, 31.22 μg/m3 and 35.42 μg/m3 for PM10, SO2 and NO2, respectively. The time sequence diagram of the daily average PM2.5, PM10, SO2 and NO2 were plotted. As shown in Figure 1A, PM2.5 concentrations increased gradually and reached their peak in the area in early October. As shown in Figure 1B to 1D, the lowest values of PM10, SO2 and NO2 concentrations appeared in July or August during the summer. All four kinds of major pollutants in the atmosphere had significantly increased in October.
Figure 1.
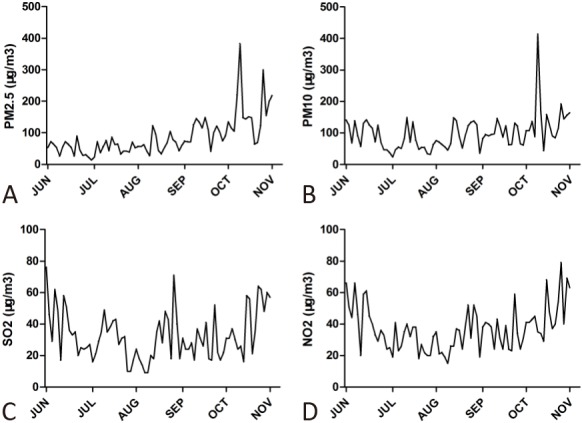
Concentration change of daily air pollutant from June 1 through October 31, 2009. (A) Daily Fine Particulate Matter (PM2.5) concentration change. (B) Daily Particulate Matter 10 (PM10) concentration change. (C) Daily sulfur dioxide (SO2) concentration change. (D) Daily nitrogen dioxide (NO2) concentration change.
The total number of study subjects with hypertension and other cardiovascular diseases in this study was 1027, with 86 cases of simple hypertension, 99 cases of cerebral hemorrhage, 353 cases of cerebral infarction, 242 cases of transient ischemic attack (TIA), and 246 cases of coronary heart diseases. As shown in Figure 1 and Figure 2, there was no obvious time lag between daily air pollutant and daily emergency department visits relating to cardiovascular diseases.
Figure 2.

Change of daily emergency admission with cardiovascular disease during June 1 and October 31, 2009. (A) Hypertension cases. (B) Cerebral hemorrhage cases. (C) Cerebral infarction. (D) Transient ischemic attack (TIA) cases. (E) Coronary heart disease cases. (F) Cardiovascular disease cases.
Analysis of the main chemical element composition in PM2.5 and the change trend
The average mass and concentration levels of Na and the other 17 kinds of chemical elements in PM2.5 were shown in Table 1. During the course of our study, the descending order of the average concentration of elements in PM2.5 in Changsha was S, Si, K, Al, Ca, Fe, Zn, Mg, Na, Mn, Pb, Ni, Ti, Cu, V, Cr, P, and As, of which the concentrations of S, Si and K reached more than 1000 ng/m3, namely 3753.23 ng/m3, 1702.69 ng/m3 and 1546.74 ng/m3.
Table 1. Average mass concentration levels of PM2.5 chemical elements in Changsha city (ng/m3).
| Indicators | Average value | Standard deviation | Minimum | Maximum | Percentiles (P) | ||
| 25 | 50 | 75 | |||||
| Na | 107.78 | 44.26 | 58.07 | 332.41 | 81.29 | 96.43 | 119.65 |
| Mg | 168.25 | 109.51 | 70.57 | 839.72 | 120.00 | 138.65 | 175.82 |
| Al | 833.55 | 380.31 | 425.83 | 2763.00 | 642.29 | 739.38 | 882.94 |
| Si | 1940.61 | 1158.14 | 759.44 | 9528.38 | 1430.57 | 1702.69 | 2095.75 |
| P | 12.19 | 5.78 | 1.80 | 45.55 | 9.08 | 11.20 | 13.27 |
| S | 3780.55 | 1525.23 | 966.14 | 9425.91 | 2763.43 | 3753.23 | 4415.92 |
| K | 1997.57 | 1695.27 | 296.39 | 11273.27 | 900.14 | 1546.74 | 2610.00 |
| Ca | 568.06 | 221.62 | 385.44 | 1638.62 | 438.02 | 483.09 | 612.40 |
| Ti | 34.53 | 18.73 | 13.05 | 145.10 | 23.49 | 30.84 | 38.83 |
| Fe | 462.51 | 222.12 | 181.63 | 1723.37 | 340.41 | 412.09 | 506.90 |
| Mn | 65.79 | 65.23 | 7.58 | 318.61 | 24.78 | 35.03 | 94.90 |
| Ni | 40.72 | 18.62 | 9.04 | 100.95 | 30.50 | 39.80 | 47.73 |
| Cu | 29.68 | 14.25 | 6.38 | 73.63 | 20.92 | 28.21 | 37.94 |
| Zn | 324.33 | 178.03 | 86.27 | 915.87 | 223.00 | 270.47 | 368.41 |
| Pb | 56.67 | 24.70 | 15.84 | 140.77 | 41.10 | 51.18 | 66.23 |
| V | 27.66 | 13.77 | 4.29 | 73.87 | 16.51 | 26.05 | 34.85 |
| Cr | 20.69 | 7.05 | 7.58 | 45.02 | 15.86 | 20.41 | 25.49 |
| As | 11.91 | 6.41 | 1.62 | 30.95 | 7.40 | 10.79 | 14.34 |
Al, aluminium; As, arsenic; Ca, calcium; Cr, chromium; Cu, copper; Fe, iron; K, potassium; Mg, magnesium; Mn, manganese; Na, Sodium; Ni, nickel; P, phosphorus; Pb, lead; S, sulfur; Si, silicon; Ti, titanium; V, vanadium; Zn, zinc.
Correlation analysis between atmospheric pollutants and meteorological factors
Considering the impact of air temperature, relative humidity, atmospheric pressure and the maximum wind speed, Spearman’s correlation between the atmospheric pollutants (PM2.5, PM10, SO2, NO2) and the temperature, relative humidity, barometric pressure and maximum wind speed were analyzed. Our study found that PM2.5 was positively correlated with PM10, SO2, NO2, negatively correlated with temperature and maximum wind speed, and positively correlated with atmospheric pressure. PM10 was positively correlated with SO2 and NO2, and had positive correlation with barometric pressure. SO2 had a positive correlation with NO2, and was negatively correlated with the relative humidity. NO2 was negatively correlated with air temperature and relative humidity, but positively correlated with barometric pressure (Table 2).
Table 2. Spearman’s correlation analysis between atmospheric pollutants and meteorological factors.
| Items | PM2.5 | PM10 | SO2 | NO2 | Air temperature | Relative humidity | Atmospheric pressure | Maximum wind velocity |
| PM2.5 | 1.000 | 0.546# | 0.281* | 0.463# | -0.471# | 0.011 | 0.645# | -0.262* |
| PM10 | 1.000 | 0.591# | 0.728# | -0.111 | -0.210 | 0.398# | -0.115 | |
| SO2 | 1.000 | 0.775# | 0.114 | -0.456# | 0.160 | -0.095 | ||
| NO2 | 1.000 | -0.063 | -0.361# | 0.355# | -0.233* | |||
| Air temperature | 1.000 | -0.597# | -0.683# | -0.027 | ||||
| Relative humidity | 1.000 | 0.070 | 0.135 | |||||
| Atmospheric pressure | 1.000 | -0.148 | ||||||
| Maximum wind velocity | 1.000 |
* p < 0.05; # p < 0.01.
Correlation analysis between PM2.5, PM10 and emergencies with cardiovascular diseases
After the impact of everyday air temperature, air pressure and maximum wind speed were adjusted for the selected PM2.5, the OR value for the impact of lag 0d PM2.5 pollution on emergency admissions with hypertension, cerebral hemorrhage and TIAs reached the maximum. And the OR value for the impact of lag 2d PM2.5 pollution on emergency admissions with cerebral infarction, coronary heart disease and the overall cardiovascular diseases was the largest, but the differences were not statistically significant (p > 0.05). The concentration of PM2.5 and chemical elements on the day of the emergency, which is lag 0d, were chosen in subsequent study to analyze its effects on emergencies with cardiovascular diseases, and lag 0d was chosen in PM10 analysis as well.
Taking into account that PM2.5 and PM10 were positively correlated with SO2 and NO2, SO2 and NO2 were further corrected to perform multi-pollutant model analysis. As shown in Figure 3, after NO2, SO2 and meteorological factors were corrected simultaneously, the OR value of the emergency admissions with cerebral hemorrhage was 1.177 [95% confidence interval (CI): 1.006-1.376] when the PM2.5 increased by 10 μg/m2, and the correlation was statistically significant (p = 0.04). While the OR values of the emergency admissions with simple hypertension, cerebral infarction, TIA, coronary heart disease and total emergency hospital admissions were 1.080 (95% CI: 0.960-1.215), 1.040 (95% CI: 0.953-1.135), 1.028 (95% CI: 0.901-1.172), 1.021 (95% CI: 0.901-1.156) and 1.014 (95% CI: 0.896-1.148), respectively, these association had no statistical significance (p > 0.05). Figure 4 showed that the difference of the OR value between PM10 and emergency admissions with cardiovascular diseases was not statistically significant.
Figure 3.
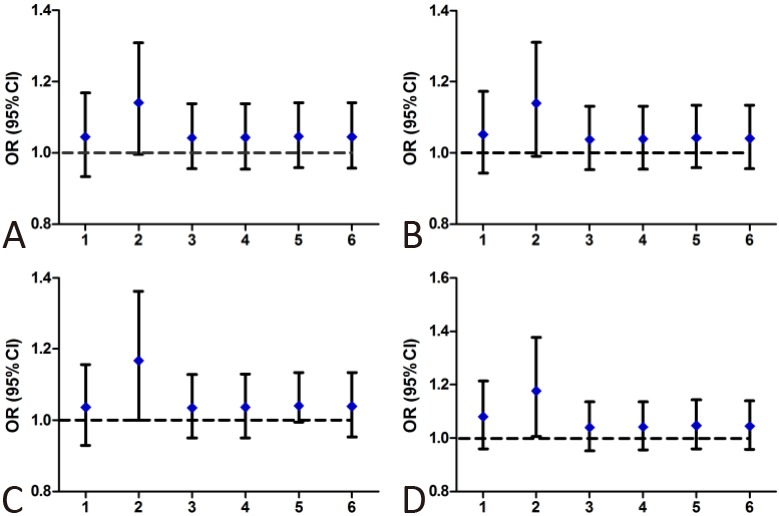
Correlation of PM2.5 concentrations and cardiovascular disease risk. (A) PM2.5. (B) PM2.5 corrected SO2. (C) PM2.5 corrected NO2. (D) PM2.5 corrected SO2 and NO2. 1, hypertension. 2, cerebral hemorrhage. 3, cerebral infarction. 4, TIA. 5, coronary heart diseases. 6, cardiovascular diseases.
Figure 4.
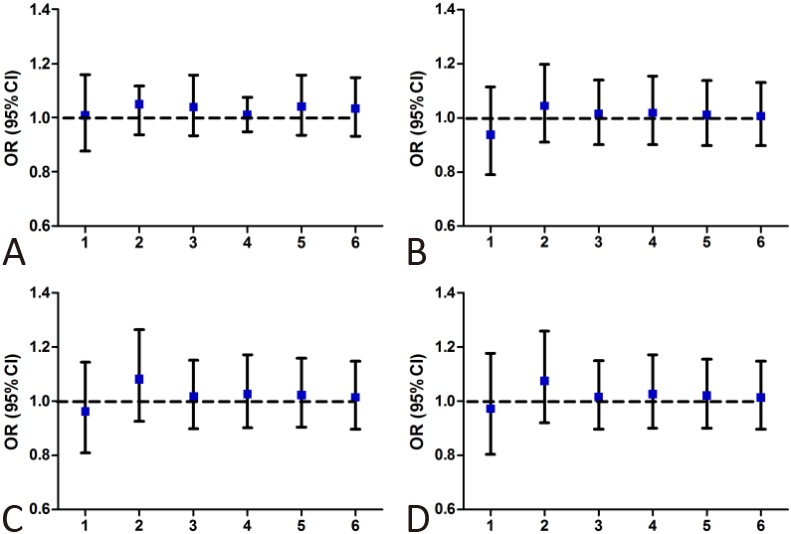
Correlation of PM10 concentrations and cardiovascular disease risk. (A) PM10. (B) PM10 corrected SO2. (C) PM10 corrected NO2. (D) PM10 corrected SO2 and NO2. 1, hypertension. 2, cerebral hemorrhage. 3, cerebral infarction. 4, TIA. 5, coronary heart diseases. 6, cardiovascular diseases.
Correlation analysis between concentrations of chemical elements in PM2.5 and emergency admission with cardiovascular diseases
The correlation analysis between concentrations of elemental composition in PM2.5 and the emergency admission with cardiovascular disease was shown in Table 3. Therein, the concentration of Ni, Zn and Pb elements were related to hypertensive cerebral hemorrhage in emergency admissions. For each additional increase IQR (17.23 ng/m3) of Ni element concentration, the OR value was 1.826 (95% CI: 1.031-3.233, p = 0.04). For each additional increase IQR (145.41 ng/m3) of Zn element, the OR value was 1.568 (95% CI: 1.015-2.423, p = 0.04), and for each additional increase IQR (25.13 ng/m3) of Pb element, the OR value was 1.682 (95% CI: 1.010-2.800, p = 0.05). The concentration of other elements had no statistically significant association with emergencies involving hypertension cardiovascular diseases (p > 0.05).
Table 3. PM 2.5 element concentrations and emergency treatment OR values of hypertension associated with cardiovascular disease (for each additional one IQR).
| Hypertension | Cerebral hemorrhage | Cerebral infarction | TIA | Coronary heart disease | Total cardiovascular diseases | |
| Na | 0.704 (0.259-1.916) | 1.157 (0.407-3.294) | 0.918 (0.439-1.921) | 0.959 (0.450-2.042) | 1.022 (0.489-2.139) | 0.944 (0.454-1.963) |
| Mg | 1.131 (0.641-1.995) | 0.984 (0.697-1.390) | 1.049 (0.784-1.402) | 1.042 (0.780-1.392) | 1.040 (0.779-1.390) | 1.044 (0.782-1.393) |
| Al | 1.241 (0.702-2.196) | 1.163 (0.759-1.783) | 1.066 (0.742-1.532) | 1.066 (0.740-1.534) | 1.065 (0.742-1.529) | 1.066 (0.743-1.529) |
| Si | 1.103 (0.610-1.991) | 0.985 (0.692-1.402) | 0.975 (0.708-1.344) | 0.964 (0.700-1.326) | 0.966 (0.703-1.328) | 0.968 (0.704-1.332) |
| P | 1.027 (0.596-1.769) | 1.048 (0.630-1.744) | 1.076 (0.699-1.656) | 1.098 (0.706-1.707) | 1.079 (0.700-1.661) | 1.059 (0.690-1.625) |
| S | 1.420 (0.468-4.307) | 2.022 (0.865-4.724) | 1.291 (0.683-2.439) | 1.365 (0.723-2.580) | 1.272 (0.679-2.385) | 1.367 (0.724-2.579) |
| K | 0.836 (0.472-1.480) | 1.318 (0.686-2.532) | 0.860 (0.564-1.308) | 0.889 (0.593-1.334) | 0.934 (0.626-1.392) | 0.920 (0.617-1.317) |
| Ca | 0.892 (0.570-1.395) | 1.437 (0.734-2.813) | 0.899 (0.603-1.342) | 0.929 (0.623-1.386) | 0.960 (0.649-1.420) | 0.941 (0.636-1.392) |
| TI | 0.879 (0.452-1.707) | 1.079 (0.626-1.859) | 0.936 (0.596-1.471) | 0.933 (0.595-1.463) | 0.924 (0.519-1.443) | 0.942 (0.602-1.473) |
| V | 1.922 (0.822-4.493) | 1.622 (0.858-3.066) | 1.759 (0.958-3.228) | 1.644 (0.897-3.015) | 1.665 (0.904-3.067) | 1.736 (0.951-3.167) |
| Cr | 0.448 (0.130-1.545) | 1.269 (0.542-2.971) | 1.241 (0.640-2.408) | 1.159 (0.598-2.248) | 1.157 (0.608-2.201) | 1.165 (0.608-2.233) |
| Mn | 1.042 (0.557-1.948) | 0.987 (0.919-1.061) | 0.878 (0.546-1.413) | 0.869 (0.537-1.406) | 0.981 (0.614-1.568) | 0.933 (0.587-1.482) |
| Fe | 1.084 (0.518-2.269) | 1.054 (0.653-1.700) | 1.034 (0.679-1.575) | 1.030 (0.677-1.566) | 1.038 (0.682-1.578) | 1.029 (0.678-1.563) |
| Ni | 1.016 (0.551-1.876) | 1.826 (1.031-3.233)* | 1.169 (0.723-1.890) | 1.277 (0.777-2.097) | 1.184 (0.725-1.933) | 1.204 (0.747-1.941) |
| Cu | 0.999 (0.449-2.225) | 1.201 (0.623-2.317) | 1.008 (0.569-1.786) | 1.087 (0.617-1.916) | 1.032 (0.586-1.819) | 1.064 (0.609-1.861) |
| Zn | 0.810 (0.474-1.384) | 1.568 (1.015-2.423)* | 1.059 (0.720-1.559) | 1.054 (0.714-1.556) | 1.084 (0.733-1.603) | 1.063 (0.724-1.561) |
| As | 0.998 (0.605-1.646) | 1.155 (0.748-1.785) | 1.019 (0.684-1.518) | 1.116 (0.729-1.707) | 1.066 (0.717-1.583) | 1.046 (0.705-1.552) |
| Pb | 0.838 (0.473-1.485) | 1.682 (1.010-2.800)* | 0.988 (0.657-1.485) | 0.974 (0.646-1.468) | 1.008 (0.675-1.505) | 0.988 (0.660-1.478) |
* p < 0.05.
DISCUSSION
To date, this is the first correlation study between chemical element compositions in PM2.5 and hospital emergency admission associated with cardiovascular diseases in hypertensive population in Changsha, China. Time-stratified case-crossover design and conditional logistic regression models were used to analyze the correlation between emergency admission of cerebral hemorrhage, cerebral infarction, TIA, and coronary heart disease in hypertensive patients, and the concentrations of PM2.5 and its chemical elemental composition.
Arising from the daily average concentration change analysis of 18 kinds of chemical elements in PM2.5, we found that the increased concentration of three elements in PM2.5, including Ni, Zn and Pb, would increase the number of emergency admissions with hypertensive cerebral hemorrhage. Zanobetti et al.14 analyzed emergency admission data of the elders in 26 communities of the United States from 2000-2003, and found that Ni, As, Cr, Br and organic carbon (OC) component in PM2.5 were closely related to hospitalization caused by coronary heart disease, myocardial infarction, heart failure, diabetes and respiratory diseases. The elemental analysis in this study showed that Na, K and other elements were derived from waste biomass fuel combustion and the secondary particles, that Ni element was from characteristic elements of diesel combustion, and that Zn and Pb were mainly from automobile tires, brake pads wear and vehicle fuel emissions. These elements were consistent with the main source (soil dust, traffic emissions, coal combustion, waste incineration, secondary particulate matter and diesel exhaust) of air pollution in Changsha shown in a previous study.13 Therefore, this study suggested that controlling the air pollution caused by transport emissions and biomass burning may reduce the occurrence of emergencies with hypertensive cerebral hemorrhage.
We also confirmed that the PM2.5 concentration increase was closely related to the emergencies of cerebral hemorrhage in hypertensive patients. After simultaneously correcting meteorological factors, including NO2 and SO2, as the daily average PM2.5 increased by 10 ug/m3, the OR value of cerebral hemorrhage was 1.177 (95% CI: 1.006-1.376). However, no association between the PM10 concentrations and emergency admissions with hypertension cardiovascular diseases was seen in this study. We speculated that the incidence of hypertension-related cerebral hemorrhage was mainly influenced by the concentration of PM2.5 in Changsha, but not by PM10. Guo12 found that with every 10 ug/m3 increase in PM2.5 and PM10, the hypertensive emergency admission risk in Beijing was 1.084 (95% confidence interval (CI: 1.028, 1.139) and 1.060% (95% CI: 1.020, 1.101). Nascimento15 found that with 10 ug/m3 for each additional PM10, the hospitalization rate of hypertension increased by 13%. The pathogenesis and environmental data of the 63,724 death cases were analyzed in Japan, and it was found that death caused by brain hemorrhage was clearly correlated with the concentration of particulate matter (PM7) within 2 hours before death. When the average concentration of PM7 per hour reached above 200 ug/m3 in this period, the OR value of the death caused by cerebral hemorrhage was 2.40 (95% CI: 1.480-3.890).9 Nonetheless, the relationship between PM10 and hemorrhagic death in different areas remains controversial, while the researchers found that the correlation was negative in Chicago, but positive in Minneapolis.9
In order to investigate whether there was a time lag effect on the impact of PM2.5 on emergencies with hypertensive cardiovascular diseases, the lag situation on day 0, 2, or 4 was analyzed. The results showed that when NO2, SO2 and meteorological factors were corrected, as PM2.5 increased by 10 μg/m3, the OR value of emergency admissions with hypertensive cerebral hemorrhage was 1.177 (95% CI: 1.006-1.376), and the correlation was statistically significant (p = 0.042). However, no association was found in the data of lag 2d or 4d, which was similar to Guo et al.’s findings.16 The results of an association between PM2.5 and death caused by cerebral hemorrhage suggested that the blood pressure increase caused by long-term and short-term PM2.5 exposure was associated with the activation of the body’s inflammatory response,17,18 and Brook et al.19 found that PM2.5 had a delayed effect on the vascular injury. Even if a direct attack of PM2.5 disappeared, the blood pressure would fall, but the damage to the vessels could last for 24 hours.
The temperature is generally negatively correlated with PM2.5, which was confirmed by our data (Table 2). In the single pollutant models and multiple pollution models analysis, we took the air temperature as covariate to minimize the bias of temperature. Interestingly, we found the highest PM2.5 concentration in October as Figure 1A showed. The environmental pollution problems in China have some special characteristics based on the complicated emission sources. Changsha is famous for fireworks manufacturing in China, and there were several large fireworks shows in October. In our monitoring data, the maximum concentration of PM2.5 can even reach 382.14 μg/m3 in October. Therefore, a large number of emissions lead to a higher concentration of PM2.5 in October, and this phenomenon is repeated every year, which could well support our findings.
There were some limitations in this study. For example, the cases came from a single center, although they were all residents near the hospital. Since we cannot get the patient’s socio-economic data, the study did not take the socio-economic factors into account, which may affect the patients’ choice for hospital. As a pilot study, certain patients’ characteristics (e.g. body mass index, smoking, comorbidity) were not analyzed in this study. Secondly, in our study, PM2.5 was monitored for only five months, which is a comparatively short period. This is mainly because China mainland has just begun to monitor PM2.5 concentration from 2013, yet the database is still not open to public and the elements of PM2.5 have not been monitored regularly. Furthermore, the environmental concentrations and individual exposure concentrations had some differences. Because elemental concentrations of particulate matter were often lower, and obviously affected by various meteorological factors, no more elements and results associated with the disease were found. Hence, longer and prospective clinical studies are needed to further confirm this association.
CONCLUSIONS
In the present study, we found that concentration rises of nickel, zinc and lead elements for PM2.5 were related to the increase of emergency admissions with cerebral hemorrhage. This result aids to further understand the hazards mechanism of air pollution on the cerebrovascular diseases, and might provide a reference for the local environmental governance.
Acknowledgments
This study was supported by the National Natural Science Foundation of China (81673520, 81202166), the National Science and Technology Benefiting Funds (2012GS430101), and the Scientific and Technological Project of Hunan (2011SK3240).
COMPETING INTERESTS
None of the authors have any competing interests.
REFERENCES
- 1.Gao Y, Chen G, Tian H, et al. China National Diabetes and Metabolic Disorders Study Group. Prevalence of hypertension in china:a cross-sectional study. PLoS One. 2013;8:e65938. doi: 10.1371/journal.pone.0065938. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Xu G, Ma M, Liu X, Hankey GJ. Is there a stroke belt in China and why? Stroke. 2013;44:1775–1783. doi: 10.1161/STROKEAHA.113.001238. [DOI] [PubMed] [Google Scholar]
- 3.Wang WJ, Lu JJ, Wang YJ, et al. China National Stroke Registry (CNSR) Clinical characteristics, management, and functional outcomes in Chinese patients within the first year after intracerebral hemorrhage: analysis from China National Stroke registry. CNS Neurosci Ther. 2012;18:773–780. doi: 10.1111/j.1755-5949.2012.00367.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Brook RD, Rajagopalan S, Pope CA, 3rd, et al. Particulate matter air pollution and cardiovascular disease: an update to the scientific statement from the American Heart Association. Circulation. 2010;121:2331–2378. doi: 10.1161/CIR.0b013e3181dbece1. [DOI] [PubMed] [Google Scholar]
- 5.Brook RD, Weder AB, Rajagopalan S. “Environmental hypertensionology” the effects of environmental factors on blood pressure in clinical practice and research. J Clin Hypertens (Greenwich) 2011;13:836–842. doi: 10.1111/j.1751-7176.2011.00543.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Pope CA, 3rd, Ezzati M, Dockery DW. Fine-particulate air pollution and life expectancy in the United States. N Engl J Med. 2009;360:376–386. doi: 10.1056/NEJMsa0805646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Wellenius GA, Boyle LD, Wilker EH, et al. Ambient fine particulate matter alters cerebral hemodynamics in the elderly. Stroke. 2013;44:1532–1536. doi: 10.1161/STROKEAHA.111.000395. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Auchincloss AH, Diez Roux AV, Dvonch JT, et al. Associations between recent exposure to ambient fine particulate matter and blood pressure in the Multiethnic Study of Atherosclerosis (MESA). Environ Health Perspect. 2008;116:486–491. doi: 10.1289/ehp.10899. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Yamazaki S, Nitta H, Ono M, et al. Intracerebral haemorrhage associated with hourly concentration of ambient particulate matter: case-crossover analysis. Occup Environ Med. 2007;64:17–24. doi: 10.1136/oem.2005.021097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jia X, Song X, Shima M, et al. Effects of fine particulate on heart rate variability in Beijing: a panel study of healthy elderly subjects. Int Arch Occup Environ Health. 2012;85:97–107. doi: 10.1007/s00420-011-0646-3. [DOI] [PubMed] [Google Scholar]
- 11.Chen LC, Lippmann M. Effects of metals within ambient air particulate matter (PM) on human health. Inhal Toxicol. 2009;21:1–31. doi: 10.1080/08958370802105405. [DOI] [PubMed] [Google Scholar]
- 12.Guo Y, Tong S, Zhang Y, et al. The relationship between particulate air pollution and emergency hospital visits for hypertension in Beijing, China. Sci Total Environ. 2010;408:4446–4450. doi: 10.1016/j.scitotenv.2010.06.042. [DOI] [PubMed] [Google Scholar]
- 13.Li JD, Deng QH, Lu C, Huang PL. Chemical compositions and source apportionment of atmospheric PM10 in suburban area of Changsha, China. J Cent South Univ Technol. 2010;17:509–515. [Google Scholar]
- 14.Zanobetti A, Franklin M, Koutrakis P, Schwartz J. Fine particulate air pollution and its components in association with cause-specific emergency admissions. Environ Health. 2009;8:58. doi: 10.1186/1476-069X-8-58. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Nascimento LF, Francisco JB. Particulate matter and hospital admission due to arterial hypertension in a medium-sized Brazilian city. Cad SaudePublica. 2013;29:1565–1571. doi: 10.1590/0102-311x00127612. [DOI] [PubMed] [Google Scholar]
- 16.Guo Y, Tong S, Li S, et al. Gaseous air pollution and emergency hospital visits for hypertension in Beijing, China: a time-stratified case-crossover study. Environ Health. 2010;9:57. doi: 10.1186/1476-069X-9-57. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Fuks K, Moebus S, Hertel S, et al. Heinz Nixdorf Recall Study Investigative Group. Long-term urban particulate air pollution, traffic noise, and arterial blood pressure. Environ Health Perspect. 2011;119:1706–1711. doi: 10.1289/ehp.1103564. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Coogan PF, White LF, Jerrett M, et al. Air pollution and incidence of hypertension and diabetes in African American women living in Los Angeles. Circulation. 2012;125:767–772. doi: 10.1161/CIRCULATIONAHA.111.052753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Brook RD, Urch B, Dvonch JT, et al. Insights into the mechanisms and mediators of the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension. 2009;54:659–667. doi: 10.1161/HYPERTENSIONAHA.109.130237. [DOI] [PMC free article] [PubMed] [Google Scholar]