
Figure 1. Preventing astrocyte scar formation does not lead to spontaneous regrowth of CST, AST, or 5HT axons after SCI.
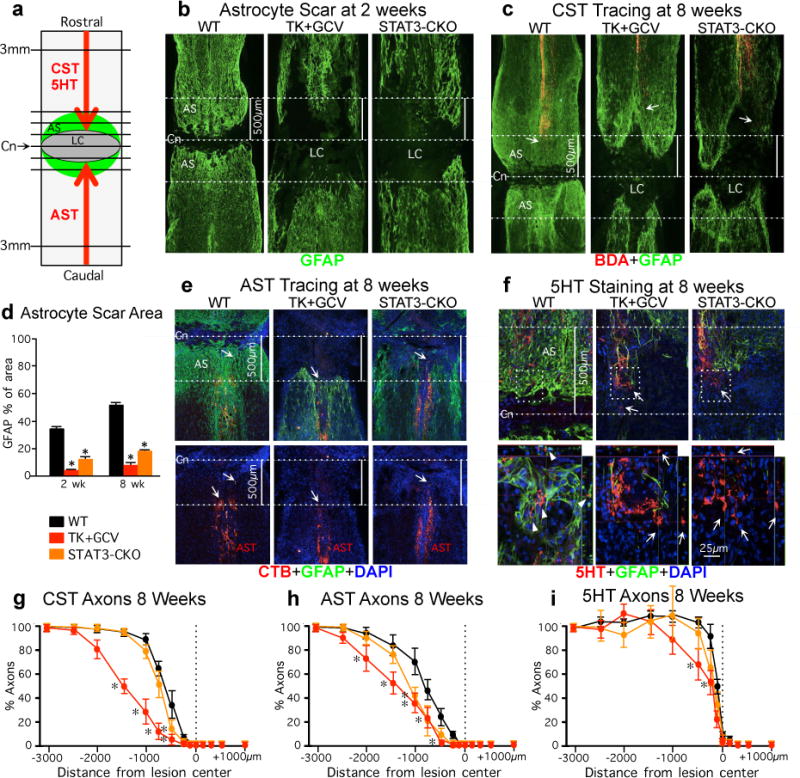
(a) Experiment summary schematic. Horizontal view of lesion core (LC) and astrocyte scar (AS) after SCI. Intercepts of CST, AST or 5HT axons with lines drawn at various distances from lesion center (Cn) were counted and expressed as a percent of axons 3mm proximal. (b,c,e,f) Dotted lines demarcate Cn and 500μm on either side. (b,d) Area occupied by GFAP-positive scar-forming astrocytes within 500μm on either side of Cn at 2 or 8 weeks after SCI. n = 6; (c, e) Arrows depict most caudal CST axons (BDA-tracing) or most rostral AST axons (CTB-tracing). (f) Arrows in top images depict most caudally penetrating 5HT axons, boxed areas are shown below. In WT mice, 5HT axons are surrounded by AS (arrowheads). In TK+GCV and STAT3-CKO mice, many 5HT axons are not in contact with AS (arrows), but have not regrown. (g–i) Numbers of CST (g), AST (h) and 5HT (i) axons at various distances from the SCI lesion center (Cn) as a percent of the number of axons present 3mm proximal. n = 6 CST; n = 5 AST and 5HT; * p<0.05 versus WT (ANOVA with Newman-Keuls).