
Figure 3: Cardiovascular Magnetic Resonance for Differentiation of Aetiology of Left Ventricular Hypertrophy.
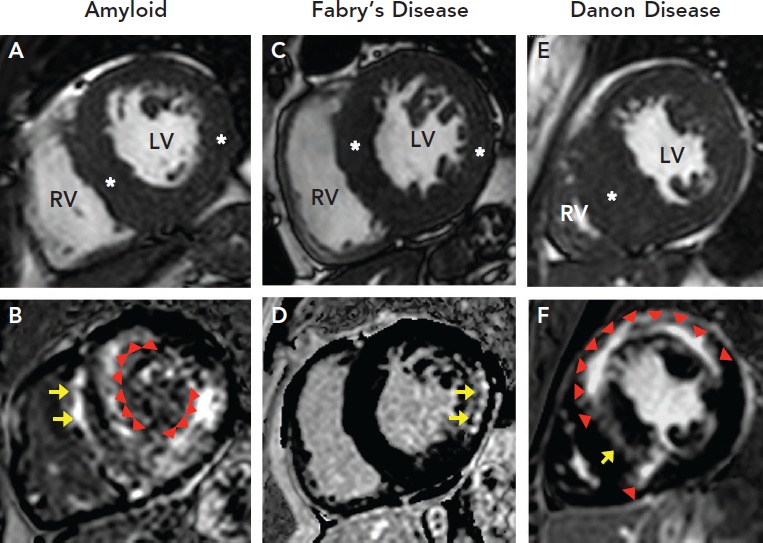
Three different patients referred for evaluation of HCM; CMR in each raised concern for alternative aetiology of LV hypertrophy. A: Pre-contrast short-axis CMR image in a 64-year-old man with increased LV wall thickness in both septum and lateral wall (maximum wall thickness of 18 mm in septum and 14 mm in lateral wall). B: Post-contrast images in the same patient demonstrates early contrast washout with epicardial LGE in septum (arrows) and global subendocardial LGE (arrowheads) leading to concern for amyloidosis. Patient underwent cardiac biopsy confirming a diagnosis of amyloidosis. C: Pre-contrast short-axis CMR image in a 44-year-old woman with increased LV wall thickness in both septum and lateral wall (maximum wall thickness of 16 mm in septum and 13 mm in the lateral wall). D: Post-contrast images in the same patient demonstrate LGE confined to the basal inferolateral wall leading to concern for Fabry’s disease. Patient underwent genetic testing, which revealed a pathogenic mutation in the galactosidase alpha gene confirming the diagnosis. E: Pre-contrast short-axis CMR image in a 21-year-old man demonstrated massive LV hypertrophy (wall thickness of 32 mm) confined to the ventricular septum (asterisk). F: Post-contrast images in the same patient demonstrated transmural LGE throughout the anterior and lateral walls with mid-myocardial LGE throughout the septum in a pattern atypical for HCM and thereby raising concern for Danon Disease. Genetic testing was thereby sent and revealed a pathogenic mutation in the lysosomal-associated membrane protein 2 gene confirming the diagnosis. CMR = cardiovascular magnetic resonance; HCM = hypertrophic cardiomyopathy; LGE = late-gadolinium enhancement; LV = left ventricle; RV = right ventricle.