
Figure 2.
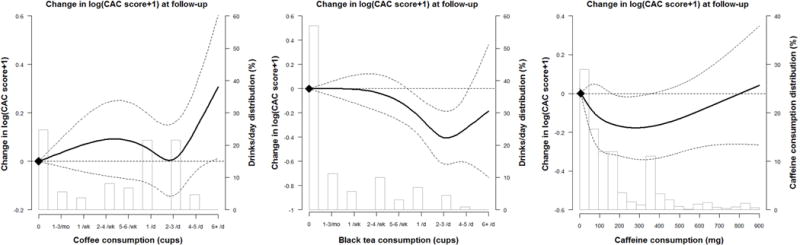
Change log (coronary artery calcium scores+1) during follow up among all participants by coffee, tea and caffeine consumption at baseline.
The curves represent the adjusted change of CAC scores and coffee/tea consumption. The dose response association of coffee/tea consumption was estimated by using a linear and a cubic spline term for coffee/tea consumption in the mixed effect regression. The reference values (diamond dots) were set at 0 drink per day. For caffeine intake, knots were set at the 5th, 35th, 65th and 95th percentiles of their sample distributions (corresponding to 0.5, 59, 161, 626 mg). The reference values (diamond dots) were set at 10th percentile (5 mg). The model adjusted for age, sex, race/ethnicity, education, smoking (never, former, current), physical activity, total fat, alcohol consumption, fruits quartiles, vegetables quartiles, red meat quartiles, systolic and diastolic blood pressures, use of antihypertensive medications, lipid-lowering medication, anti-diabetic medication, BMI, family history of CHD, diabetes, HDL-cholesterol, total cholesterol, and triglyceride.