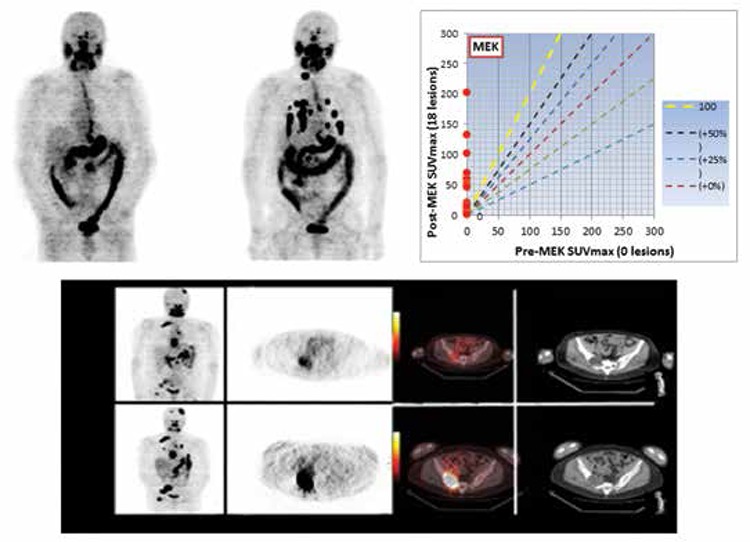
Figure 4. A thyroid cancer patient with widely metastatic neck nodes, pulmonary nodules, mediastinum, and osseous sites. The upper row is the baseline study before seluemetanib treatment (left), and the post four week MEK treatment image showing a number of pulmonary lesions now taking up the radioactive iodine. The graph (top, right) compares the standardized uptake values (SUV) before (abscissa) and after (ordinate) treating in quantitative terms. No lesions were detectable in terms of 124I prior to treatment and subsequently, the uptake that developed was seen. There is a different patient showing baseline (upper row) and the re-induction effects of treatment on radioiodine uptake (bottom row). There are new lesions in the lungs and the osseous lesions have greater uptake (left panel coronal image baseline, above and post-treatment below); cross-sectional imaging 124I imaged on positron emission tomography, baseline (above) and post-treatment (below). There is marked increase in the intensity of uptake in the R. pelvis, and the relationship to computed tomography findings is dramatically displayed in the fusion positron emission tomography/computed tomography, which shows a space occupying lesion in the R. ileum, now with therapeutic levels of uptake. As part of the selumetinib pilot trial, we have been able to document dose-response relationships between 124I lesional dosimetry and subsequent structural disease response as determined by Response Evaluation Criteria in Solid Tumors criteria in eight differentiated thyroid cancer patients (1).