
Figure 3.
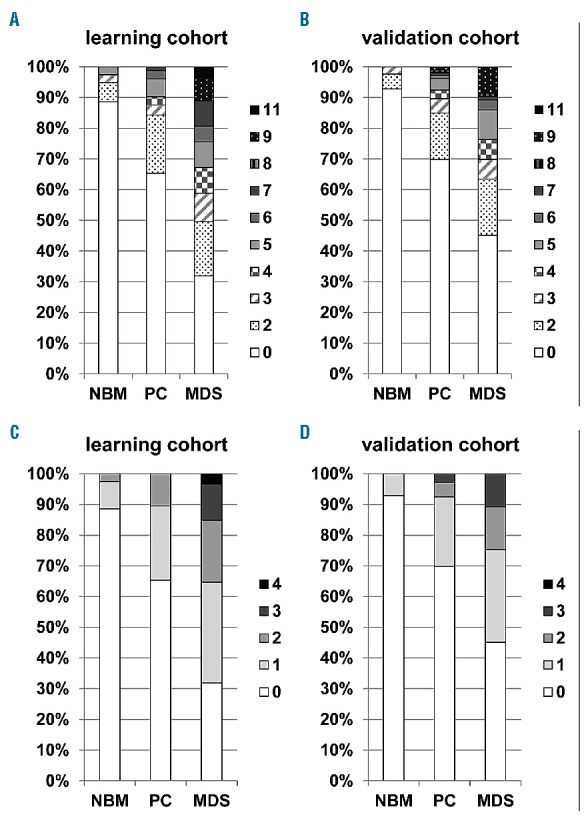
FC-erythroid dysplasia score in learning and validation cohorts. The weighted score consists of four parameters: increase in CD36 CV (4 points) and CD71 CV (3 points); decrease in CD71 MFI (2 points); and decrease or increase of CD117+ erythroid progenitors (2 points). A maximum score of 11 points can be reached. Data are grouped as normal bone marrow (NBM), pathological controls (PC) and MDS, relative distribution of the results for the score is displayed along the Y-axes. Panel A. represents the learning cohort consisting of 79 normal bone marrow samples (NBM), 153 pathological controls (PC) and 119 MDS cases. The FC-erythroid dysplasia score could only be calculated in the cases with data on all four defined parameters (351/670 cases). Panel B. represents the results in the validation cohort consisting of 42 NBM samples, 106 pathological controls and 93 MDS cases (241/320 cases). Clonal disorders as aplastic anemia and those within the category of essential thrombocythemia, polycythemia vera and primary myelofibrosis were excluded from both cohorts (two and nine cases for learning and validation cohorts, respectively). A cut-off of ≥5 points resulted in a specificity of 90% (95% CI: 84–94%) and a sensitivity of 33% (95% CI: 24–42) in the learning cohort; in the validation cohort, specificity was 92% (95% CI: 86–97%) and sensitivity 24% (95% CI: 15–34%). The numerical score, depicted in panels C and D, consists of four parameters: increase in CD36 CV and CD71 CV; decrease in CD71 MFI; and decrease or increase of CD117+ erythroid progenitors. A maximum score of 4 points can be reached. A cut-off of ≥2 points resulted in a specificity of 90% (95% CI: 84–94%) and a sensitivity of 35% (95% CI: 27–45) in the learning cohort; in the validation cohort, specificity and sensitivity were 92% (95% CI: 86–97%) and 25% (95% CI: 16–35%), respectively.