
Fig. 1.
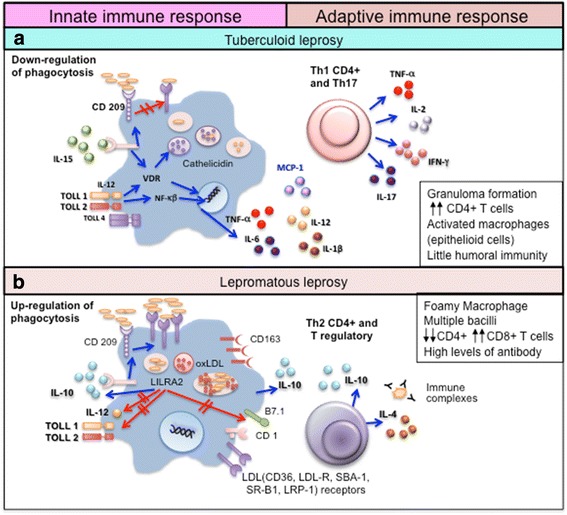
Immune response in the polar clinical forms of leprosy. a In tuberculoid leprosy (TT) patients, the innate immune response is activated by M. leprae through toll-like receptors (TLR2/1). IL-15 stimulates the vitamin D-dependent antimicrobial program in macrophages and inhibits phagocytosis of mycobacteria. These events promote a Th1 T-cell cytokine response (IFN-γ, IL-2, TNF, and IL-15) that contains the infection in well-formed granulomas, and a Th17 response (IL-17A, IL-17F, IL-21 and IL-22) that leads to tissue inflammation and destruction, neutrophil recruitment, macrophage activation, and enhancement of Th1 effector cells. b In lepromatous leprosy (LL) patients, IL-4, IL-10, leukocyte immunoglobulin-like receptor subfamily A member 2 (LILRA2), and oxidized phospholipids inhibit TLR2/1-induced cytokine responses but preserve IL-10 release. In addition, immune complexes trigger IL-10 production and increase phagocytosis of M. leprae, ApoB, haptoglobin-hemoglobin complex and oxidized phospholipids by macrophages through the receptors CD209 and CD163, without activating the vitamin D-dependent antimicrobial pathway. The foamy appearance of macrophages is due to the accumulation of lipid droplets (LD) inside these cells. There is an upregulation of perilipin and the adipose differentiation-related protein in the endoplasmic reticulum–Golgi complex with the formation of vesicles containing lipids, phospholipids, cholesterol ester, and cholesterol. Further, there is an increase in both the synthesis of LDL receptors (such as CD36, LDL-R, SBA-1, SR-B1, and LRP-1) and uptake of endogenous cholesterol that accumulates intracellularly. This induces a Th2 and Treg immune profile, with the production of IL-4 and IL-10, antibody production, absence of granulomas, and failure to restrict M. leprae growth [26, 31, 32, 41–46]