

Abstract
Aim of the Study:
To study the effect of scrambler therapy on patients with chronic cancer pain.
Materials and Methods:
This is a prospective, observational study conducted on patients with chronic pain due to malignancy which is not responding to oral analgesics. A total of twenty patients were included in the study (ten males, ten females) with a visual analog scale score of >4 on oral analgesics. Patients aged 18–70 years with a life expectancy of >3 months having bony, neuropathic, or mixed type of pain were included in the study. A total of 12 sessions of scrambler therapy were planned, ten sessions on consecutive days and one session each on two follow-up visits after 1 week each. Each session lasted for 40 min. Pain relief and quality of life according to the World Health Organization Quality of Life were recorded as primary outcome variables.
Results:
All patients had good pain relief and improvement in all four domains of quality of life. Pain scores decreased significantly (P < 0.01) after each session and at each follow-up. Patients showed significant improvement in physical, psychological, social, and environmental health (P < 0.01) after the therapy.
Conclusion:
Scrambler therapy offers a promising role in the pain physician's armamentarium as an adjunct to pharmacological therapy for the treatment of chronic drug-resistant cancer pain; it may bring down analgesic drug requirements significantly and improve quality of life in cancer patients. Larger prospective, randomized multicenter studies are needed to validate the findings of the small pilot studies published in literature so far.
Keywords: Chronic pain, scrambler therapy, visual analog scale scores, World Health Organization Quality of Life
INTRODUCTION
The World Health Organization (WHO) estimates that approximately 9 million new cancer cases are diagnosed every year,[1] and there are nearly 15 million cancer patients worldwide.[2] In India, 2–2.5 million new cancer cases are diagnosed every year.[3] Cancer treatment is a niche which has improved a lot over the last decade. Aggressive clinical research, drug trials, development of better modalities of treatment through advanced biomedical engineering have increased survival and quality of life in cancer patients. With increased survival, good symptom control and supportive care are gaining importance to improve quality of life. Pain management is an integral part of symptom control. Cancer-related pain is multifactorial, it may be due to the disease per se, including pain secondary to involvement of bone, nerves, viscera, or soft tissue by the tumor, or it can be due to treatment of cancer leading to painful conditions such as chemotherapy-induced peripheral neuropathy (CIPN) and radiation-induced mucositis. Cancer or its treatment may lead to somatic, visceral, or neuropathic pain.[4]
Cancer pain is usually managed by pharmacological therapy under five essential concepts given by the WHO, i.e. treatment (1) by the ladder, (2) round the clock, (3) by mouth, (4) individual or patient specific, and (5) with attention to detail.[4] Nonsteroidal anti-inflammatory drugs, opioids, and adjuvants such as gabapentinoids form the basis of pharmacological therapy, but their use and dosage are limited by their adverse effects.[5,6]
Recognizing the limitations and hazards of use of multiple drugs for pain relief, increasing emphasis is being placed on the nonpharmacologic options for the management of chronic cancer pain. Neuromodulatory techniques such as transcutaneous electrical nerve stimulation (TENS) and scrambler therapy have gained popularity in recent times. Scientific data supporting these methods are limited.[7,8]
A wide variety of patients with chronic cancer pain are managed by the pharmacological therapy in our pain clinic outpatient department. Inadequate pain relief or intolerable adverse effects are seen in some patients despite using multimodal pharmacological approach to control pain and drug-related side effects such as nausea, vomiting, and constipation.
Scrambler therapy with MC5-A Calmare® is a device designed for use as an adjunct in the management of chronic pain. Preliminary studies with this device have shown variable success rates for management of chronic pain.[9,10]
We conducted this study in patients with chronic cancer pain not adequately controlled with pharmacological therapy.
The device
Scrambler therapy provides noninvasive cutaneous electrostimulation, aiming to substitute “nonpain” sensation for “pain.” The device produces 16 different electrical currents that simulate normal nerve action potentials. These currents are organized into algorithms that take into account factors such as previous outputs, frequency, duration, and amplitude of modulation.[11] Surface electrodes which transmit impulses are placed on the area surrounding pain. If the electrodes are placed properly, patient should experience immediate pain reduction after each session of therapy as pain signals are replaced by nonpain signals. The electrical charge used in scrambler therapy has been approved safe by the Food and Drug Administration. The current delivered ranges from 3.50 to 5.50 mA and voltage delivered ranges from 06.5 to12.5 V, with settings of 10–70 on the dial corresponding to lowest and highest delivered current and voltage. The maximum current density is 0.0002009 W/cm2. The phase duration is 6.8–10.9 ms and the pulse rate is 43–52 Hz. The average charge per phase is 38.8 μC, which is same as the conventional TENS device. The maximum frequency of scrambler device is 52 Hz; thus, the mean energy delivered per second is less than most standard TENS.[11,12] Various mechanisms of action suggested for scrambler therapy are substituting pain signals with nonpain signals so that patient reports new sensations such as itching or flow of impulses or pressure sensation over the previously painful area. In addition, there is no C-fiber stimulation; thus, no painful sensations are generated. Separate receptors are thought to transmit nonpain information, thus brining almost immediate pain relief. Furthermore, long-lasting pain relief with scrambler therapy suggests either resetting of calcium channels channel receptors at the neuromuscular junction or remodulation of central and peripheral nervous system. Finally, nonpain information is thought to spread along the lines of nerve transmission, thus bringing pain relief throughout the dermatome and not just in the area under the electrodes.[11]
Electrodes are not placed at the site of actual pain but instead placed at a nearby location of preserved sensation. Intensity of stimulation is adjusted according to patient comfort, and if the placement is correct, pain is usually replaced by a pleasant, vibratory, and/or humming sensation.[13] The device runs for about 30–45 min in each session. Patient experiences pain relief from the first sitting itself, and the duration of posttreatment analgesia keeps increasing with each successive sitting. The duration of posttreatment relief classically lengthens with continued treatments until, ideally, the benefit is maintained throughout the entire day.
Usually, scrambler therapy is given for a total of ten treatment sessions. Pain relief is expected to persist for weeks to months after treatment. If patients relapse, booster sessions are administered.[13]
MATERIALS AND METHODS
Objectives
The objective is to study the impact of scrambler therapy on chronic cancer pain and quality of life (WHO quality of life domains).
Methodology
In the given observational study, patients were recruited from the outpatient pain clinic, and scrambler therapy was instituted in the Department of Onco-Anaesthesia and Palliative Care, Indian Rotary Cancer Hospital, All India Institute of Medical Sciences, after approval by the Ethics Committee of our hospital.
Selection criteria
A total of twenty patients were included in the study. Informed consent was taken before enrolling the patients; inclusion and exclusion criteria were as follows.
Inclusion criteria
Cancer patients having bony, neuropathic, or mixed type of pain with an average visual analog scale (VAS) >4
18–70 years of age
Ability to complete study questionnaire(s) by themselves or with assistance
Patient having life expectancy >3 months
Patients of childbearing potential agreeing to use acceptable contraceptive methods (e.g., double barrier) during the treatment.
Exclusion criteria
Not willing to participate in study
History of an allergic reaction or previous intolerance to TENS
Use of other interventional modalities for pain control (e.g., TENS, nerve blocks) concurrently or in the past 30 days
Psychiatric disorders affecting the ability to participate in study (e.g., mania, psychosis, schizophrenia)
Presence of dermatologic conditions that preclude application of skin electrodes
Uncontrolled seizures
Patient on antiepileptic medications
Any form of medical “metal” device (e.g., pacemakers, defibrillators, vascular clips, stents, cardiac valve or joint replacements)
Pregnant and nursing women.
Procedure
Patients were scheduled to undergo a total of 12 sittings of scrambler therapy, ten cycles on consecutive days and one each at the two follow-up visits after 1 week each.
On the first visit, pain was assessed by VAS and the area of pain was marked. Electrodes were placed on and around the area of maximal pain. If there was a painful open cancer wound, the electrodes were placed around the open wound after aseptic cleaning of the wound. Once the electrodes were positioned appropriately, the device was turned on and the current intensity was increased to the maximal tolerated strength; with an option of turning down/switching off the current intensity, if pain occurred due to the electric current during the procedure. Up to five channels or sets of electrodes were used during treatment as shown in Figure 1. Each patient received daily sessions for ten consecutive days for 40 min on each day. Patients had the option to stop the treatment in between if they felt no pain relief. A comfortable position of the patient was ensured as time taken for each sitting was 40 min. Placement of electrodes was individualized according to the site of pain and dermatome involved, and during study, the position of electrodes was changed according to the change in site of pain. As shown in Figure 2a–d, the area of electrode placement changed in the same patient during therapy as the painful area decreased with each sitting of scrambler therapy. Pain scores were assessed daily, before and after the procedure, and in the two follow-up visits. The quality of life was assessed using WHOQOL BREF Questionnaire[14] at the time of enrolment, after the tenth session, and at follow-up visits. Follow-up was maintained with regular telephonic conversations and on hospital visits.
Figure 1.

CALMARE MC 5A with five channels of electrodes.
Figure 2.

Placement of electrodes in a patient. Involvement of C3 dermatome in a patient as well placement of electrodes and change in position of electrodes with the changing area of pain during therapy. (a) Before treatment. (b) Primarily area of pain. (c) During treatment of ST. (d) After treatment of ST. (e) Area of pain. ST (scrambler therapy).
RESULTS
A total of twenty patients (ten males and ten females) were included in the study. All patients successfully completed the therapy and no adverse effects were observed.
Values obtained by the study of each qualitative variable were expressed as absolute and relative frequencies, whereas continuous variables were expressed as mean, median, or mode. To find the association between categorical variables, Chi-square test or Fisher exact (pre- and post-therapy) test or Wilcoxon test was used according to the distribution of data, and in case of more than two groups, repeated measure ANOVA was used as required. P < 0.05 was considered as statistically significant.
Scrambler therapy provided pain relief and had a positive effect on quality of life of all the patients. VAS scores for pain were decreased significantly after each session [Table 1]. Improvements in physical, psychological, and social health were seen in all the patients [Table 2 and Figure 3].
Table 1.
Mean visual analog scale score distribution
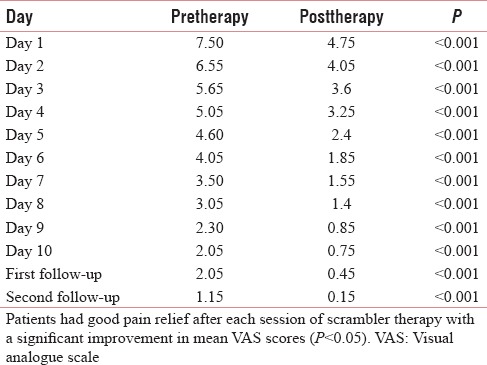
Table 2.
Mean domain scores for quality of life domains at 1st day, 10th day, first follow-up, and second follow-up
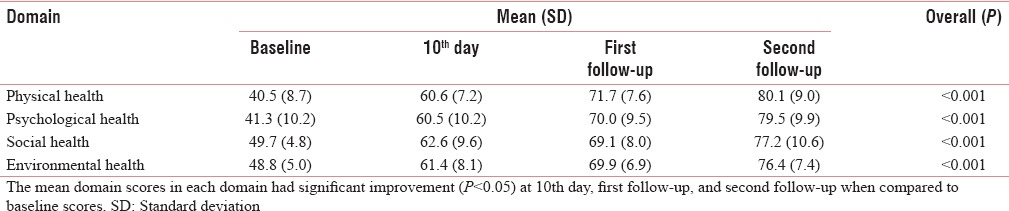
Figure 3.
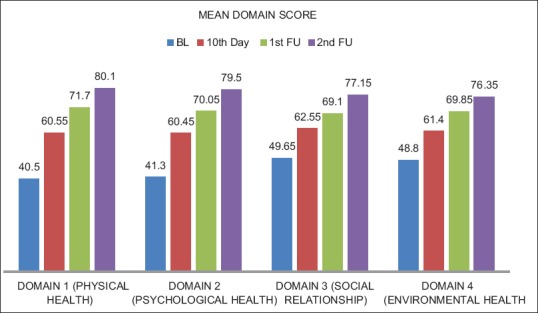
Impact of scrambler therapy on World Health Organization domains of quality of life. As seen in the figure, improvement in all four domains of life according to World Health Organization Quality of Life was seen with scrambler therapy after the ten sessions and on each follow-up (BL - baseline, FU - follow-up).
DISCUSSION
Scrambler therapy was introduced as a method of chronic pain relief in 2003, in the first trial involving this technique by Giuseppe Marineo, the developer of scrambler therapy; 11 terminal cancer patients suffering from drug-resistant chronic visceral pain were included in the study. All patients responded positively to the treatment with significant reductions in pain score and increase in pain threshold over the ten sessions. Nine of 11 patients could stop their analgesics totally by the fifth session. No undesirable side effects were seen.[15]
In the second trial with scrambler therapy, 226 patients with neuropathic pain were treated. Eighty percent of patients reported 50% pain reduction, 10% reported pain reduction up to 25%–49%, and 10% had no appreciable response.[16]
Since then, scrambler therapy has been used with encouraging results to provide pain relief in chronic painful conditions such as CIPN,[8,12,17] low back pain,[18] postherpetic neuralgia,[19] and chronic pain, following rotator cuff repair.[20]
In the field of cancer pain management, scrambler therapy has been used successfully to relieve chronic cancer-related pain[9,21] and pain due to bony and visceral metastasis.[10]
The results of our study were in accordance with the previous studies as all patients had good pain relief with no side effects. We observed significant reduction in pain scores after every sitting (P < 0.001) for all the ten sittings. Mean VAS scores decreased from pretreatment value of 7.5–0.45 after tenth sitting (P < 0.05). Similar results were seen in 25 cancer patients with bony and visceral metastasis having chronic intractable pain. After 10 days of scrambler therapy, pain scores significantly reduced from 8.4 ± 1.4 to 2.9 ± 1.5 (P = 0.008), and pain scale just after each daily treatment was always significantly lower than numeric rating scale just prior the session of scrambler therapy.[10]
As in previous studies,[8,9,10,22] we observed no adverse effects in patients on use of scrambler therapy.
Quality of life has been suggested an important outcome measure in studies related to pain management.[14] This is in line with the concept of total pain which deals with social, psychological, and spiritual aspects of pain in addition to physical pain and their effect on quality of life.[23] We studied changes in quality of life of the patients with scrambler therapy for their pain management, an aspect which has not been studied frequently in literature.[10,24] This is one of the main strengths of our study. Improvements in all domains (physical, psychological, social, and environmental health) were seen after scrambler therapy, which further reinforces the use of this modality as a nonpharmacological adjunct to chronic cancer pain treatment.
This is one of the first attempts in the context of Indian patient population to see the benefit of scrambler therapy in cancer pain; this is another strength of our study.
Our study had drawbacks such as limited sample size of twenty patients, no control or placebo group for comparison, no patient or observer blinding. Since this was pilot observational study, we would like to improve upon these drawbacks with larger study having a bigger sample size, blinding at observer recording the pain scores. Placebo or control groups in studies involving application of a device or a technique may be difficult and a sham-controlled methodology has to be applied.[25] Till date, only one trial with single blinding and sham control has been conducted on thirty patients with low back pain randomized to scrambler therapy or a sham placebo group.[22] The methodology of this trial may be used in randomized placebo-controlled trials in future. Sham-controlled studies for pain relief in clinical practice may face ethical problems.[25,26] Such trials would only be valid in the research setting, but their extrapolation to clinical settings will be questionable.[26]
CONCLUSION
Scrambler therapy offers a promising role in the pain physician's armamentarium as an adjunct to pharmacological therapy for treatment of chronic drug-resistant cancer pain; it may bring down analgesic drug requirements significantly and improve quality of life in cancer patients. Larger prospective, randomized multicenter studies are needed to validate the findings of the small pilot studies published in literature so far so that this promising technique gains wider acceptance.
As shown in Table 1, patients had good pain relief after each session of scrambler therapy, with a significant improvement in mean VAS scores after each session (P < 0.05).
The mean domain scores in each domain had significant improvement over baseline (P < 0.05) at 10th day and 1st and 2nd follow-up when compared to baseline scores [Table 2].
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent forms. In the form the patient(s) has/have given his/her/their consent for his/her/their images and other clinical information to be reported in the journal. The patients understand that their names and initials will not be published and due efforts will be made to conceal their identity, but anonymity cannot be guaranteed.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.World Health Organization. Cancer Pain Relief: With A Guide To Opioid Availability. World Health Organization. 1996 [Google Scholar]
- 2.Stewart B, Christopher P. Wild. “World Cancer Report 2014.”. World (2016) [Google Scholar]
- 3.Krishnan NM, Varghese C, Swaminathan R. “Cancer: current scenario, intervention strategies and projections for 2015.”. NCHM Background papers-Burden of Disease in India. 2005:219–25. [Google Scholar]
- 4.Chang HM. Pain and its management in patients with cancer. Cancer Invest. 2004;22:799–809. doi: 10.1081/cnv-200032845. [DOI] [PubMed] [Google Scholar]
- 5.Breivik H, Cherny N, Collett B, de Conno F, Filbet M, Foubert AJ, et al. Cancer-related pain: A pan. European survey of prevalence, treatment, and patient attitudes. Ann Oncol. 2009;20:1420–33. doi: 10.1093/annonc/mdp001. [DOI] [PubMed] [Google Scholar]
- 6.Finnerup NB, Sindrup SH, Jensen TS. The evidence for pharmacological treatment of neuropathic pain. Pain. 2010;150:573–81. doi: 10.1016/j.pain.2010.06.019. [DOI] [PubMed] [Google Scholar]
- 7.Cruccu G, Aziz TZ, Garcia-Larrea L, Hansson P, Jensen TS, Lefaucheur JP, et al. EFNS guidelines on neurostimulation therapy for neuropathic pain. Eur J Neurol. 2007;14:952–70. doi: 10.1111/j.1468-1331.2007.01916.x. [DOI] [PubMed] [Google Scholar]
- 8.Coyne PJ, Wan W, Dodson P, Swainey C, Smith TJ. A trial of Scrambler therapy in the treatment of cancer pain syndromes and chronic chemotherapy-induced peripheral neuropathy. J Pain Palliat Care Pharmacother. 2013;27:359–64. doi: 10.3109/15360288.2013.847519. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Ricci M, Pirotti S, Scarpi E, Burgio M, Maltoni M, Sansoni E, et al. Managing chronic pain: Results from an open-label study using MC5-A Calmare® device. Support Care Cancer. 2012;20:405–12. doi: 10.1007/s00520-011-1128-6. [DOI] [PubMed] [Google Scholar]
- 10.Notaro P, Dell'Agnola CA, Dell'Agnola AJ, Amatu A, Bencardino KB, Siena S. Pilot evaluation of scrambler therapy for pain induced by bone and visceral metastases and refractory to standard therapies. Support Care Cancer. 2016;24:1649–54. doi: 10.1007/s00520-015-2952-x. [DOI] [PubMed] [Google Scholar]
- 11.Marineo G, Iorno V, Gandini C, Moschini V, Smith TJ. Scrambler therapy may relieve chronic neuropathic pain more effectively than guideline-based drug management: Results of a pilot, randomized, controlled trial. J Pain Symptom Manage. 2012;43:87–95. doi: 10.1016/j.jpainsymman.2011.03.015. [DOI] [PubMed] [Google Scholar]
- 12.Smith TJ, Coyne PJ, Parker GL, Dodson P, Ramakrishnan V. Pilot trial of a patient-specific cutaneous electrostimulation device (MC5-A Calmare®) for chemotherapy-induced peripheral neuropathy. J Pain Symptom Manage. 2010;40:883–91. doi: 10.1016/j.jpainsymman.2010.03.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Majithia N, Smith TJ, Coyne PJ, Abdi S, Pachman DR, Lachance D, et al. Scrambler Therapy for the management of chronic pain. Support Care Cancer. 2016;24:2807–14. doi: 10.1007/s00520-016-3177-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.WHOQOL-BREF: Introduction, Administration, Scoring, and Generic Version of the Assessment. Geneva: WHO; 1996. World Health Organization, Programme on Mental Health. [Google Scholar]
- 15.Marineo G. Untreatable pain resulting from abdominal cancer: New hope from biophysics? JOP. 2003;4:1–10. [PubMed] [Google Scholar]
- 16.Sabato AF, Marineo G, Gatti A. Scrambler therapy. Minerva Anestesiol. 2005;71:479–82. [PubMed] [Google Scholar]
- 17.Pachman DR, Watson JC, Loprinzi CL. Therapeutic strategies for cancer treatment related peripheral neuropathies. Curr Treat Options Oncol. 2014;15:567–80. doi: 10.1007/s11864-014-0303-7. [DOI] [PubMed] [Google Scholar]
- 18.Ghatak RK, Nandi SN, Bhakta A, Mandal GC, Bandyopadhyay M, Kumar S. Prospective study of application of biological communication (cybernatics) in management of chronic low back pain – A preliminary report. Nepal Med Coll J. 2011;13:257–60. [PubMed] [Google Scholar]
- 19.Smith TJ, Marineo G. Treatment of postherpetic pain with scrambler therapy, a patient-specific neurocutaneous electrical stimulation device. American Journal of Hospice and Palliative Medicine. 2013 doi: 10.1177/1049909113494002. 1049909113494002. [DOI] [PubMed] [Google Scholar]
- 20.Lee DK, Kim EK. Effect of pain scrambler therapy on shoulder joint pain and range of motion in patients who had undergone arthroscopic rotator cuff repair for the first time. J Phys Ther Sci. 2016;28:2175–7. doi: 10.1589/jpts.28.2175. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Lee SC, Park KS, Moon JY, Kim EJ, Kim YC, Seo H, et al. An exploratory study on the effectiveness of “Calmare therapy” in patients with cancer-related neuropathic pain: A pilot study. Eur J Oncol Nurs. 2016;21:1–7. doi: 10.1016/j.ejon.2015.12.001. [DOI] [PubMed] [Google Scholar]
- 22.Starkweather AR, Coyne P, Lyon DE, Elswick RK, Jr, An K, Sturgill J. Decreased low back pain intensity and differential gene expression following Calmare®: Results from a double-blinded randomized sham-controlled study. Res Nurs Health. 2015;38:29–38. doi: 10.1002/nur.21632. [DOI] [PubMed] [Google Scholar]
- 23.Anita A, Chan LS. Understanding of the concept of total pain: A prerequisite for pain control. J Hosp Palliat Nurs. 2008;10:26–32. [Google Scholar]
- 24.Pachman DR, Weisbrod BL, Seisler DK, Barton DL, Fee-Schroeder KC, Smith TJ, et al. Pilot evaluation of Scrambler therapy for the treatment of chemotherapy-induced peripheral neuropathy. Support Care Cancer. 2015;23:943–51. doi: 10.1007/s00520-014-2424-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Macklin R. The ethical problems with sham surgery in clinical research. N Engl J Med. 1999;341:992–6. doi: 10.1056/NEJM199909233411312. [DOI] [PubMed] [Google Scholar]
- 26.Miller FG, Kaptchuk TJ. Sham procedures and the ethics of clinical trials. J R Soc Med. 2004;97:576–8. doi: 10.1258/jrsm.97.12.576. [DOI] [PMC free article] [PubMed] [Google Scholar]