
Figure 1. Receiver operating characteristic (ROC) curve showing the 10 and 11.5 cutpoints in the HIV+ group.
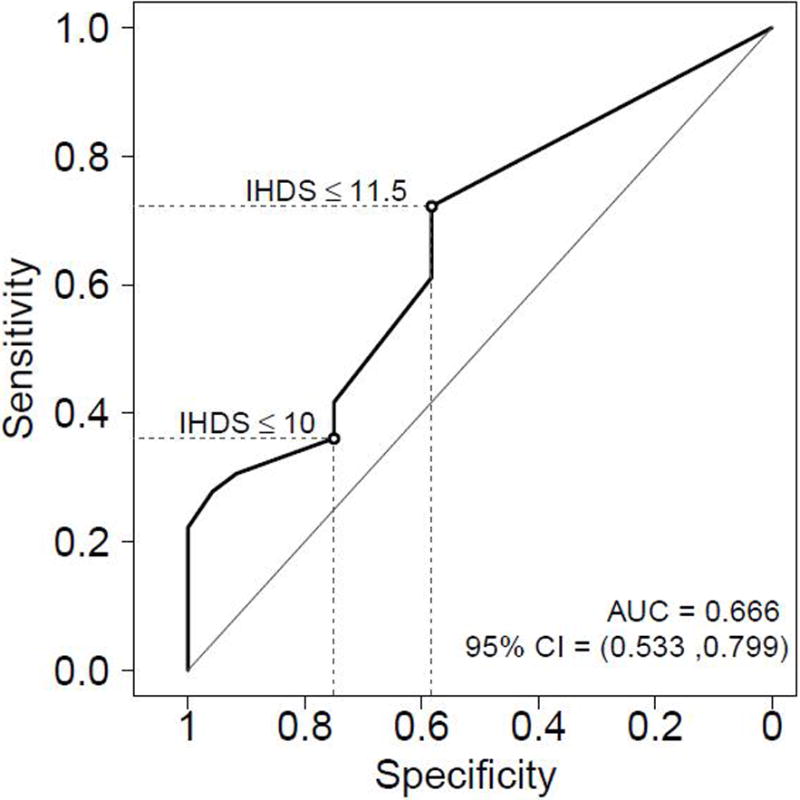
In the HIV+ group (n=60), Sensitivity and specificity of the standard raw cutpoint (≤10) were 36% and 75%. Using the cutpoint of ≤11.5 improved the sensitivity to 72% but decreased the specificity to 58%. The positive predictive value (PPV) increased slightly from 68% (≤10) to 72% (≤11.5) and the negative predictive value (NPV) increased from 44% (≤10) to 58% (≤11.5). The overall accuracy for the standard cutpoint (≤10) was 52% while the 11.5 cutpoint provided an overall accuracy of 67%. Youden’s index (J) increased from 0.11 (≤10) to 0.30 (≤11.5); Youden’s index is the vertical distance between the ROC curve and the first bisector (or chance line).
Considering only the participants HIV+ with HAD (n=5) and using 11.5 cut-off, the sensitivity of IHDS was 40% (2 out of 5 got values below 11.5); while three (60%) got a perfect score of 12, but it is a very small number of subjects limiting the ability to test the accuracy.