

Abstract
Introduction:
In vitro fertilization is becoming more and more popular lately, as such light is to be shed on any possible related complication. One of these complications is the possible hormonal effect on the lipid profile of the patients.
Case presentation:
We present a case of a 39-year-old woman with no prior or family history of dyslipidemia, who presented with post in vitro fertilization severe hypertriglyceridemia and secondary acute pancreatitis and diabetic ketoacidosis. Discussion of the case is followed by a brief review of the literature related to in vitro fertilization–induced hypertriglyceridemia.
Conclusion:
This is, up to our knowledge, the sixth reported case of in vitro fertilization–induced hypertriglyceridemia with secondary acute pancreatitis. This is a serious and life-threatening complication. As such, it might be wise at least in high-risk patients (such as patients with diabetes mellitus, polycystic ovaries syndrome, obesity, and family and personal history of dyslipidemia) to screen for lipid abnormalities before initiating in vitro fertilization and monitor these levels afterward.
Keywords: In vitro fertilization, hypertriglyceridemia, mixed dyslipidemia, acute pancreatitis, diabetic ketoacidosis
Introduction
With in vitro fertilization (IVF) becoming more and more popular, an increased level of awareness as to the possible associated complications becomes necessary. One of these complications, which can be life threatening, is the hormonal effects on the lipid profile of the patient. We hereby present a case of IVF-induced severe hypertriglyceridemia with secondary severe hemorrhagic acute pancreatitis.
Case presentation
We present a case of a 39-year-old woman with a history significant for infertility, a type II diabetes mellitus, and a body mass index (BMI) of 27.5, who presented to our emergency department (ED) 10 days after an IVF procedure with severe epigastric pain and several episodes of nausea and vomiting that started one day prior to presentation. On initial evaluation in the ED, she was afebrile and hemodynamically stable. Her physical examination was significant only for epigastric and left upper quadrant pain. Her BMI was 27.5. Initial laboratory work-up could not be accurately interpreted due to severe lipemia (Figure 1); however, it revealed a serum level of lipase of 2470 U/L, amylase of 1000 U/L, blood glucose of 301 mg/dL, sodium of 117 meq/L, chloride of 92 meq/L, bicarbonate of 12 meq/L, aspartate transaminase of 60 U/L, alanine transaminase of 24 U/L, gamma-glutamyl transferase of 14 U/L, and alkaline phosphatase of 66 U/L. Arterial serum lactate was 0.78 meq/L, and urine ketone levels was valued as 4+ on urine dipstick. An ultrasound of the abdomen was performed and revealed fatty liver infiltration. A computed tomography scan of the abdomen and pelvis, done 48 h later, revealed acute hemorrhagic pancreatitis with peri-pancreatic fluid. The patient was admitted with a diagnosis of severe hypertriglyceridemia-induced acute pancreatitis, hypertriglyceridemia associated pseudo-hyponatremia, and possible diabetic ketoacidosis. The patient was admitted to the intensive care unit and started on aggressive intravenous (IV) hydration and intravenous insulin. The second day, her triglycerides dropped to 9234 mg/dL, her low-density lipoprotein (LDL) was 366 mg/dL, and her high-density lipoprotein (HDL) was 40 mg/dL. Her symptoms improved progressively every day and her pain became better. The third day, triglycerides dropped to 1455 mg/dL, and after confirmation of absence of pregnancy, she was started on fibrates and statins on day 3 of admission, after which her triglyceride level continued to drop (Table 1).
Figure 1.
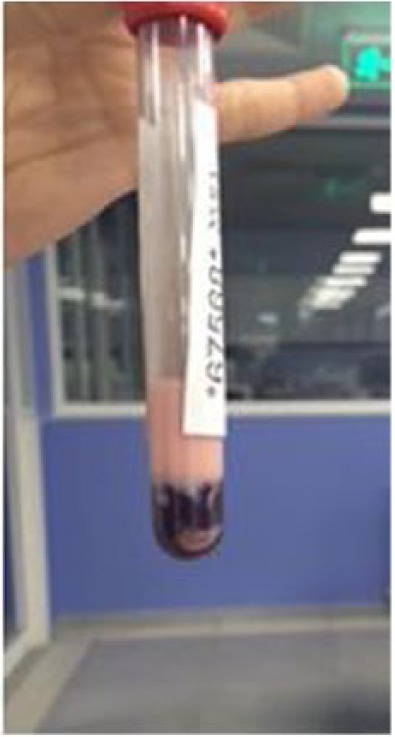
Patient’s lipemic blood on presentation.
Table 1.
Triglyceride levels during hospital stay.
| Day 1 | Day 2 | Day 3 | Day 4 | Day 5 | Day 8 | Day 10 | |
|---|---|---|---|---|---|---|---|
| Triglyceride (mg/dL) | 15,050 | 9234 | 3930 | 1455 | 887 | 252 | 325 |
The patient had a negative family history for dyslipidemia. No previous history of acute pancreatitis. She was maintained at home on oral metformin 850 mg daily for mild type II diabetes mellitus, estradiol 2 mg daily, progesterone 200 mg twice daily, aspirin 100 mg daily, and subcutaneous hydroxyprogesterone 500 mg daily and enoxaparin 40 mg daily as part of a regimen for IVF.
Discussion
This is a case of IVF-induced severe hypertriglyceridemia and mixed dyslipidemia complicated by acute pancreatitis and diabetic ketoacidosis.
A thorough review of the literature revealed several reported cases of pregnancy-associated hyperlipidemia-induced acute pancreatitis. However, to our knowledge, this is the sixth reported case of IVF-induced hypertriglyceridemia with secondary acute pancreatitis. The pathophysiology of IVF-induced hypertriglyceridemia has not yet been clearly delineated but is most likely related to estrogen therapy. Estrogens are known to increase triglycerides level by several mechanisms. Such mechanisms include an increase in the synthesis of triglycerides in the liver followed by its secretion into the circulation as very-low-density lipoprotein (VLDL),1 an increase in newly synthesized triglycerides in the liver, and the hypersecretion of triglycerides and apoprotein B.2,3 Another, still controversial, mechanism of IVF-induced hypertriglyceridemia is through estrogens’ effect on lipid metabolism, particularly through its inhibitory effect on lipoprotein lipase (LpL) promoter activity, resulting in LpL deficiency,4 an effect that was not found in another study.5 This effect on triglyceride levels seems to be more encountered in oral rather than transdermal estrogen forms.6
This case is interesting because it witnessed a paradoxical increase in the level of LDL, thus defying the effect of estrogen. Usually estrogen decreases LDL levels through both receptor-dependent and receptor-independent effects on the LDL receptors. Estrogen increases the expression of the LDL receptors and decreases the production of LDL.7 Estrogen also increases hepatic production of HDL and prolongs the half-life of circulating HDL by decreasing its clearance.7 In the study by Hammadeh et al.,8 a similar effect was achieved by demonstrating a decrease in LDL, an increase in HDL, and interestingly an increase in ketones. What complicates the interpretation of the increased levels of LDL in our patient is the fact that there were no previous records of her LDL level before the IVF. She might have had chronically high level of LDL, and thus there is no baseline level to compare to.
Furthermore, all the changes mentioned earlier rarely lead to the very high levels of triglycerides found in our patient. An exception to this rational is the presence of an underlying genetic familial disease, a remote possibility in our patient’s case particularly in the absence of a personal and family history of dyslipidemia.
Despite the fact that the lack of previous records of lipid levels makes it hard for a cause–effect relationship to be firmly concluded, it is highly unlikely for other etiologies to cause such high levels of triglycerides reaching 15,000 as in our patient. Uncontrolled diabetes as well as diabetic ketoacidosis can lead to hypertriglyceridemia but unlikely to such high levels.
The management of hypertriglyceridemia-induced pancreatitis in the acute phase is similar to other causes of acute pancreatitis with the addition of various other modalities that target specifically hypertriglyceridemia such as insulin, heparin, fibric acid derivatives, and in extreme cases plasmapheresis.9 The patient presented above responded to aggressive IV hydration in addition to fibrates and IV insulin that was helpful also in controlling her ketoacidosis.
In conclusion, our patient is one of the rare cases of reported IVF-induced severe hypertriglyceridemia with secondary acute pancreatitis. The occurrence of hypertriglyceridemia is a serious complication of IVF, particularly during pregnancy, which might lead to further increase in triglyceride level, and consequently an increased risk on both the mother and the fetus. As such, with the increasing popularity of IVF, and aiming at the prevention of such life-threatening complications, prescreening of patients with lipid levels before IVF should be highly considered, especially in those who might be at a higher risk (such as patients with diabetes mellitus, polycystic ovaries syndrome, obesity, and family and personal history of dyslipidemia).
Footnotes
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval: Our institution does not require ethical approval for reporting individual cases or case series.
Funding: The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent: Written informed consent was obtained from the patient for their anonymized information to be published in this article.
References
- 1. Melmed S, Polonsky KS, Larsen PR, et al. Williams textbook of endocrinology. 13th ed. Toronto, ON, Canada: Elsevier. [Google Scholar]
- 2. Dashti N, Kelley JL, Thayer RH, et al. Concurrent inductions of avian hepatic lipogenesis, plasma lipids, and plasma apolipoprotein B by estrogen. J Lipid Res 1983; 24: 368–380. [PubMed] [Google Scholar]
- 3. Walsh BW, Schiff I, Rosner B, et al. Effects of postmenopausal estrogen replacement on the concentrations and metabolism of plasma lipoproteins. N Engl J Med 1991; 325: 1196–1204. [DOI] [PubMed] [Google Scholar]
- 4. Homma H, Kurachi H, Nishio Y, et al. Estrogen suppresses transcription of lipoprotein lipase gene. Existence of a unique estrogen response element on the lipoprotein lipase promoter. J Biol Chem 2000; 275: 11404–11411. [DOI] [PubMed] [Google Scholar]
- 5. Applebaum DM, Goldberg AP, Pykalisto OJ, et al. Effect of estrogen on post-heparin lipolytic activity. Selective decline in hepatic triglyceride lipase. J Clin Invest 1977; 59: 601–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Vrablika M, Fait T, Kovar J, et al. Oral but not transdermal estrogen replacement therapy changes the composition of plasma lipoproteins. Metabolism 2008; 57(8): 1088–1092. [DOI] [PubMed] [Google Scholar]
- 7. Barton M. Cholesterol and atherosclerosis: modulation by oestrogen. Curr Opin Lipidol 2013; 24: 214–220. [DOI] [PubMed] [Google Scholar]
- 8. Hammadeh ME, Munz W, Meisinger M, et al. Effects of ovarian stimulation on serum concentrations of lipids and ketone bodies in patients undergoing IVF/ICSI treatment. Zentralbl Gynakol 2004; 126(2): 67–72 (in German). [DOI] [PubMed] [Google Scholar]
- 9. Coskun A, Erkan N, Yakan S, et al. Treatment of hypertriglyceridemia-induced acute pancreatitis with insulin. Prz Gastroenterol 2015; 10(1): 18–22. [DOI] [PMC free article] [PubMed] [Google Scholar]