
Fig. 3.
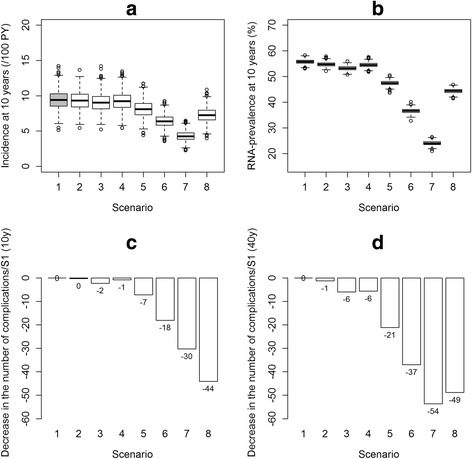
Results according to various HCV cascade of care scenarios; 1,000 simulations. a. Boxplots of the incidence at 10 years; b. Boxplots of the prevalence at 10 years; c. Proportion of cirrhosis complications avoided after 10 years (mean percentage of new cirrhosis complications avoided, compared with the reference scenario (S1)); d. Proportion of cirrhosis complications avoided after 40 years (mean percentage of new cirrhosis complications avoided, compared with the reference scenario (S1)). S1 (reference): The current HCV cascade of care using the new DAAs. S2: S1 with an improvement in the mean time to detection of chronic HCV from 2y to 0.5y. S3: S1 with an improvement in linkage to care, with a decrease in mean time to linkage to care from 1.7y to 0.5y and a loss to follow-up rate from 10.2%/y to 5%/y. S4: S1 with an improvement in adherence to treatment, i.e. we improved the SVR rate of 81% to the level demonstrated in clinical trials, i.e. 90%. S5: S1 with an improvement in treatment initiation rate from 5%/y to 10%/y when linked to care. S6: Improvement in the treatment initiation rate from 5%/y to 20%/y when linked to care. S7: Combined scenarios S2, S3, S4 and S6 to determine the impact of improvements in the entire cascade of care; no fibrosis criteria for treatment initiation. S8: S1 with an initiation of HCV treatment at fibrosis levels F2-F3-F4 only