
Figure 1.
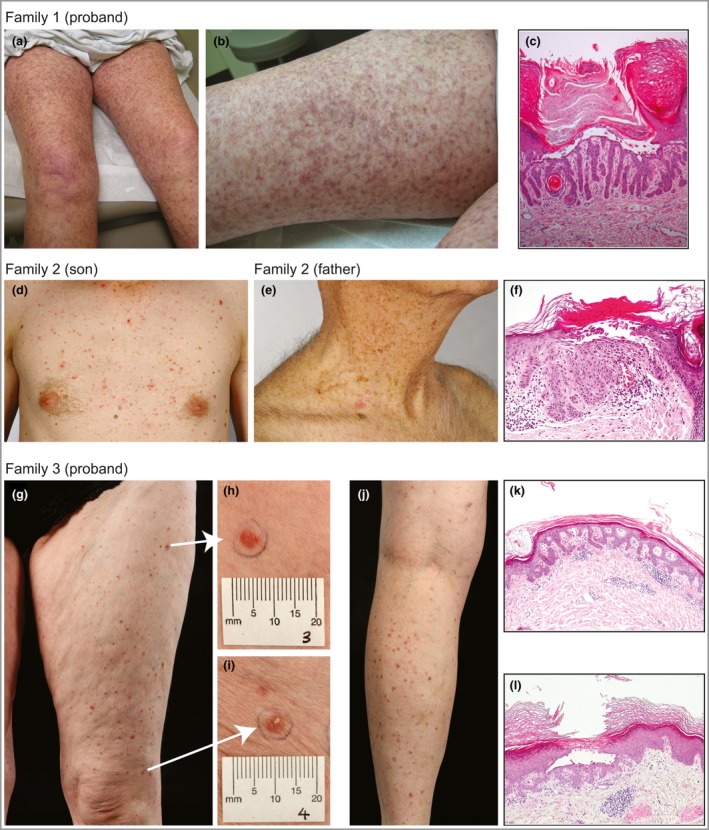
Clinical findings. (a, b) Reticulate hyperpigmented scaling plaques on the proximal legs of the proband of family 1. (c) Light microscopy of three punch biopsies from the proband of family 1 revealed similar findings of filiform digitate downgrowth of the epidermal rete ridges, presence of small horn cysts, epidermal acanthosis, hypergranulosis, and hyperkeratosis with parakeratosis and suprabasilar acantholysis. (d) Small red‐brown macules and crusted papules widely distributed over the trunk, neck, back, abdomen and limbs of the proband of family 2. The large body folds, hands and feet, and face were spared. (e) The father of the proband of family 2 had similar clinical features, limited to the neck region without involvement of the large flexures. (f) Light microscopy shows some apical acantholysis and parakeratosis with a moderate dermal inflammatory infiltrate. (g–j) The proband of family 3 with multiple small (approximately 5‐mm‐diameter) red‐brown scaly papules, present predominantly on the legs but also on the forearms with some postinflammatory change from previous lesions. (k) Light microscopy from the proband of family 3, a medium‐power view showing elongation of the rete ridge and modest inflammatory infiltrate. (l) A medium‐power view of a second biopsy from the right anterior thigh. There is an intraepidermal vesicle, as a result of acantholysis of the keratinocytes, some of which show dyskeratosis. Note the elongation of the rete ridges immediately below the vesicle.