

Summary
A preventable subgroup of burn injuries is scalds sustained from motor vehicle radiators. This study was to determine changes in trends in epidemiology of such injuries and to discuss whether current and other prevention efforts proposed previously require reinforcement. We conducted a retrospective study (February 2007-August 2015) of all motor vehicle-related burn referrals to our regional burns service. 68 cases of motor vehicle radiator burns were identified. Male to female ratio was 65:3. Mean age was 35.1 (range = 9-71). Most cases occurred in the summer months (22/68 = 32.4%). 65 cases (95.6%) involved car radiators. 66% of injuries resulted from actively removing the pressure cap of an overheated radiator in the motor vehicle. Mean total burn surface area (%TBSA) was 2.1% (range = 0.5- 11%). The depths of burn injuries were mostly superficial partial thickness. Face, chest and upper limbs were the most common sites of injury. Mean healing time was 14.2 days (range = 4-60). Following the introduction of safety measures by vehicle manufacturers, motor vehicle radiator burns in this era are mostly minor injuries and can be potentially managed conservatively as an outpatient. This contrasts with findings from previous studies over a decade ago of larger, more significant injuries requiring admission and surgery. Whilst manufacturers have installed safety measures into the design of radiator caps, our findings suggest that re-educating the public to allow a period of cooling prior to opening caps should be reinforced.
Keywords: motor vehicle; car; radiator,; scald; burns
Abstract
Les ébouillantements par liquide de refroidissement de voitures (LRV) sont évitables. Cette étude a pour but d’évaluer les changements épidémiologiques de ce type d’accidents et de discuter si les stratégies préventives passées et actuelles nécessitent une mise à jour. Nous avons étudié rétrospectivement tous les patients hospitalisés dans notre CTB entre février 2007 et août 2015 à la suite de brûlures en relation avec un véhicule à moteur. Parmi ceux-ci, 68 (65 hommes, 3 femmes) âgés en moyenne de 35,1 ans (9-71) s’étaient brûlés avec du LRV. La plupart des cas (22 soit 32,4%) étaient observés en été. La grande majorité (66 cas soit 95,6%) mettaient en cause le radiateur avec 2 fois sur 3 l’ouverture de celui-ci en raison d’une surchauffe. La surface brûlée était de 2,1% (0,5-11%) et les brûlures, le plus souvent superficielles (délai de guérison moyen de 14,2 jours (4-60), touchaient principalement la partie haute du corps (visage, thorax, membres supérieurs). Les systèmes de sécurité mis en place par les constructeurs ont permis d’observer des brûlures mineures guérissant spontanément après une prise en charge en externe, contrastant avec les observations précédentes de brûlures plus étendues et plus profondes, nécessitant une hospitalisation et des greffes. Cependant, une prévention passive insistant sur la nécessité de laisser refroidir le moteur avant d’essayer d’ouvrir le radiateur semble nécessaire.
Introduction
A preventable subgroup of motor vehicle injuries is burns from motor-vehicle radiators. Such burns can have a significant impact on return to work and patient psychological wellbeing.1 These injuries are commonly scald burns, often occurring following attempts to remove the lid of a hot radiator with high pressure or explosion of the radiator. This results in a spray of superheated fluid and steam as the content of a closed system adjusts to the surrounding environment once the closed system is breached. Current prevention strategies include instructions in car manuals, caution labels on the radiator caps, valve mechanisms to allow internal pressure to reduce before caps can be opened, and care manufacturers carefully positioning the caps so that the chances of scald injuries are minimised if the caps are opened or broken accidentally. Despite these efforts, burn injury resulting from motor vehicle radiators is a continuing problem.2 Given that this type of injury has not been reviewed for over a decade, we present a retrospective analysis of scald burns involving motor vehicle radiators treated by our burns service, a tertiary burns centre situated in the east of England that caters to a population of 9.9 million inhabitants.
The purpose of this study was to determine more recent statistics on the epidemiology of motor vehicle radiator-related scald injuries and to discuss whether current and further prevention measures require reinforcement.
Methods
We reviewed all admissions to the burns service between February 2007 and August 2015. The study data was collected via the admissions database. This enabled us to identify all patients that presented with burn injuries involving motor vehicle radiators, using the keywords ‘scald’, ‘radiator’, ‘motor-vehicle’ and ‘car’. Admission notes in patients’ medical records were reviewed to determine patient demographics and demographics of motor vehicle radiator burn injuries. These included type of motor vehicle, total burn surface area, distribution, documented burn depth and time taken to heal. At our institution, patients with scald burns are reviewed within 48 hours of injury. The wounds are cleaned and blisters de-roofed. Burn size and depth are assessed clinically by the senior burns fellow and consultant. Photographs and wound swabs are taken as standard of care. A non-adherent dressing is then applied, whilst paraffin is used on the face. Patients are reviewed again in the following 72 hours, and then weekly. Healing time was measured as the time taken for 100% re-epithelisation if managed conservatively and graft acceptance if managed surgically. We additionally reviewed the number of cases between 2007-2010 and 2011-2015 to help identify the current trend in frequency of injury, statistically analysed using a t-test. Burn injuries that were not caused by motor vehicle radiators were excluded from the study. This project was approved by our institution’s review board.
Results
Over an 8-year period (Feb 2007-August 2015), 68 cases of motor vehicle radiator burns were identified. Non-motor vehicle burns were excluded because these generally result from different mechanisms such as home radiator heating systems that cause contact burns. The mean age was 35.1 years (range 9-71 years). Male to female ratio was 65:3. When comparing the number of cases between 2007-2010 and 2011-2015, the incidence was 32/68 (47.0%) and 36/68 (53.0%) respectively (Fig. 1).
Fig. 1. Trends in motor vehicle radiator burns between 2007-2010 and 2011-2015 (p value = 1.0).
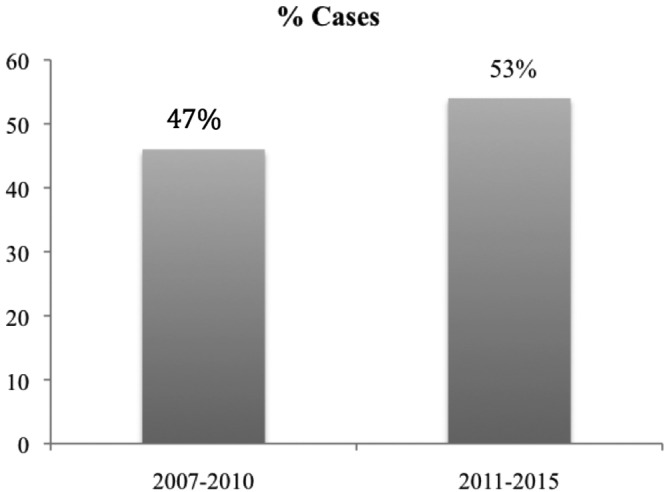
When analysing the trends between these groups, there was no statistical difference in the mean number of cases per year (p value = 1.0). Regarding time of injury, 18/68 (26.5%) cases occurred in the spring, 22/68 (32.4%) in the summer, 14/68 (20.6%) in the autumn, and 14/68 (20.6%) in the remaining winter months.
The highest proportion of cases involved car radiators, 65/68 (95.6%). Other less common vehicles were motorbikes (1/68) and large vehicles (2/68), accounting for the remaining 4.4%. Forty-five (66.2%) injuries resulted from actively removing the pressure cap of the radiator in the motor vehicle. In 6 of these cases (13.3%), opening the cap lead to an explosion from the radiator and steam. Twenty-three (33.8%) injuries occurred when the individual was in close proximity to the radiator as it exploded, commonly when the car bonnet was lifted with the radiator cap closed.
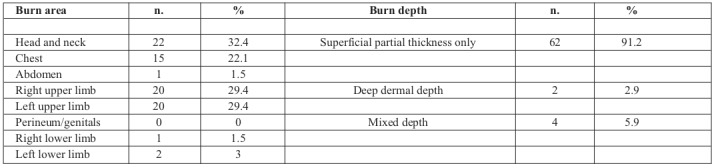
Mean total burn surface area (%TBSA) was 2.1% (range = 0.5-11%). Depth of burn injury was documented as partial thickness (PT: 62/68 = 91.2 %), mixed partial thickness/deep dermal (PT/DD: 4/68 = 5.9%) and mixed deep dermal/full thickness (DD/FT: 2/68 = 2.9%). There were no cases of purely full thickness (FT) injuries. Seven of the 68 cases (10.3%) were associated with erythema. Three patients had been wearing long sleeves and gloves. In addition, one of these patients had been wearing a facemask. These cases occurred in the autumn and winter. This attire could be attributable to the colder seasons of the year rather than the intended use as protective gear. Thirtyone had not been wearing any protective gear, and in 34/68 this was unspecified. There were 4 cases with a %TBSA >5% and these were patients who clearly had no protective gear on.
Table I reports the typical distribution pattern of burn injuries resulting from motor vehicle radiators. Our results show that the head/neck, chest and upper limbs are the most common sites of injury. This is illustrated by an example case in Fig. 2. Healing time depended on the size of the burn, and ranged from 4 days to 60 days (mean = 14.2 days). Two cases required surgical management as a result of mixed depth burns with prolonged healing. There were no reported cases of severe eye injury resulting in visual loss. There were no cases of steam inhalation injury. Sixty-six (97.1%) cases were managed as outpatients. Two cases (2.9%) were admitted, with an average length of stay of one day for overnight observation and pain management.
Table I. The distribution pattern of burns resulting from motor vehicle radiator injuries in this study.
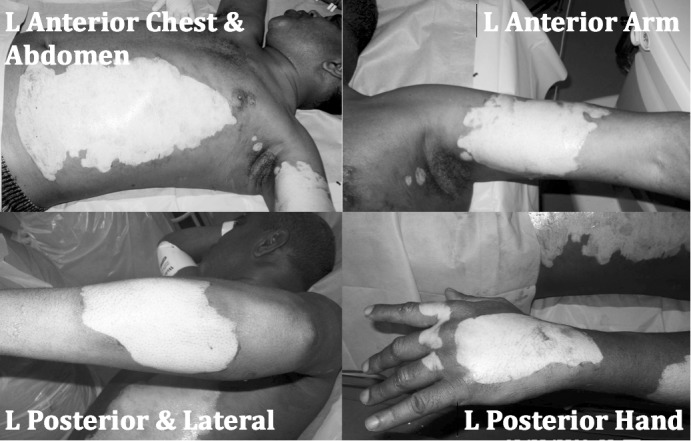
Fig. 2. A case from the study where a 48-year old male sustained 7.5% scald burns after opening a car radiator. The injuries show typical distribution on the hand, forearm, upper arm and anterior chest on the side of the dominant upper limb.
Discussion
We have presented the findings of a retrospective study of motor vehicle radiator burns over an eight-year period. This study is interesting as, to the best of our knowledge, the topic has not been reviewed for over a decade. Initial studies first described in the 1970s focused on mechanisms, distribution and the management of injuries. The most recent study conducted in 2004 showed that whilst prevention efforts had improved, motor vehicle radiator burns continued to be a problem.3 We carried out this study to determine current epidemiology of this type of injury and to see if current prevention efforts following recent studies have been effective and made a difference to previous trends. We looked at all cases referred to our tertiary burns unit between 2007-2015, and additionally reviewed the number of cases between 2007-2010 and 2011- 2015 to help identify the current trend. Similar to other studies, we found a high male to female ratio regarding motor vehicle radiator burn injuries. It is clear from previous reports that motor vehicle radiator burns most commonly occur in the summer months when radiators are most likely to overheat.1-2 In our study, whilst the summer months still had the highest number of injuries, other months also saw a high incidence. This may reflect changes in global climate and a higher number of motorists.
The demographics of the cases reviewed and the pattern of injuries in our study are in keeping with other previous studies. 1,4-5 The anterior aspects of the hand, upper limb, chest and face are most commonly injured. This reflects how a jet of heated fluid and steam is generated when the patients open the caps. The anatomical distribution of affected areas is significant in that they can result in days lost from employment, and psychological issues related to body image. The average healing time was 14.2 days. The majority of these burns were successfully managed conservatively with dressings. All cases were managed with visits to the outpatient burns dressing clinic. There were no cases of other associated injuries, including ocular injuries resulting in visual loss. Previous studies have shown cases involving ocular injury, classified as minor however.5 Two cases required admission for overnight stay and pain management. Given the overall findings, one could argue that small burn injuries can be managed by local hospitals without referral to a burns unit. Sözen et al. have shown the effectiveness of patient education and introducing and applying the principles of burns management in local hospitals.6 This would improve the efficiency of service provision and burn resources utilization.
What is most apparent when comparing our findings with studies presented over a decade ago is that the severity of car radiator burns per year appears to have decreased. However, burns sustained from motor vehicle radiators continue to be a problem. In a previous review of all 107 cases of motor vehicle-related burns over a 13-year period, it was found that car radiator-related burns accounted for only 13% of cases of motor vehicle-associated burns.1 However, in our 8 year study of 68 motor vehicle-related burns, car radiators were responsible for 95.6% (65/68) of total injuries. Our study showed a mean %TBSA of 2.1% in comparison to other studies that have reported %TBSA means ranging from 11% to 23%.3,5 Studies conducted pre-2006 showed that a significant number of patients required hospital admission, and in severe cases even needed intensive care input and surgical management as a result of large deep/full thickness burns from vehicle radiators.7-8 The injuries in our study were considered minor in comparison to those described in studies from a decade ago. We suggest that an increase in the ratio of car radiator burns compared to other types of motor vehicle burns reflects a relative decrease in other motor vehicle burn mechanisms. This in turn may reflect safer motor vehicles that are less prone to fires.
It is well known that motor vehicle radiator burn injuries are preventable and prevention strategies have been discussed for over a decade.2,7 Current prevention strategies include safety instructions in vehicle manuals, strategic placement of car radiators within the front bonnet, and hazard labels on radiator caps to warn motorists not to the remove the cap whilst still hot. Current radiator caps also have valve mechanisms that lower internal pressure before the cap can be fully opened. Motor vehicle breakdown cover companies also provide safety information regarding overheated engines. While these safety measures may have reduced the severity of burn injuries, one could question why this type of injury still occurs. Our study shows a significant number of burns from motor vehicle radiators over an 8-year period, and there does not appear to be a reduction in this type of injury compared to studies dating back to the 1990s.4-5
One can suggest that whilst manufacturers have improved motor vehicle design and safety features, the patient factor still remains an issue. The public must be aware that there is a limit as to how many safety features motor vehicle manufacturers can design, and the main concern our study raises is that patients seem to lack insight and knowledge regarding motor vehicle safety. Our findings suggest that 66.2% of injuries occurred as a result of immediate attempts to open radiator caps in overheated cars. Only a minority of injuries occurred when the individuals were in close proximity to the radiator as it exploded. In addition, only 3 patients were wearing gloves and long sleeved tops. Given that these cases occurred in the auto keep warm in the cold.
Based on this discussion, it is clear that the equipment factor impacting the severity of motor vehicle burns has been addressed by manufacturers, leaving the human education factor still lacking, thus people continue to open the radiator cap in the same manner as a decade ago. There should be an awareness campaign to educate motorists and new drivers on radiator safety, and about avoiding lifting bonnets or opening radiator caps immediately following vehicle breakdown. This should be reinforced in motor vehicle magazines, leaflets issued by the Driving Vehicle License Agency, and as a more vigorous part of driving license examinations (theory and practical components) for new motorists.
We appreciate that there are limitations to this study, including its retrospective nature, small number of cases, and the difficulty in determining exact date of 100% re-epithelisation since these cases were mostly managed as outpatients. Patients were given a follow-up date, which means they may have actually achieved 100% coverage before the mean 14.2 days. Also not investigated in this study was whether or not patients were offered psychotherapy support and how satisfied patients were with their image after the burn wound had healed.
Conclusion
Burns resulting from motor vehicle radiators in this era following the introduction of safety measures by vehicle manufacturers are mostly minor injuries and can potentially be managed conservatively as an outpatient. This is in contrast to findings from studies conducted over a decade ago where radiator burns appeared to cause larger %TBSA. More importantly, motor vehicle radiator burn injuries are preventable. Current prevention methods have reduced the severity of injuries, however the public needs further educating. Despite the safety features incorporated into motor vehicles by manufacturers, a high proportion of injuries occur from attempts to immediately open the radiator cap following vehicle breakdown. We suggest a more rigorous safety component is implemented in both the theory and practical examination for new drivers, stressing the need to allow a period of cooling before attempting to open the bonnet or radiator cap of a broken-down vehicle.
Acknowledgments
Acknowledgements.No funding was received for this work.
Conflict of interest:None
References
- 1.Papaevangelou J, Batchelor JS, Roberts AH. Motor vehicle-related burns: A review of 107 cases. Burns. 1995;21(1):36–38. doi: 10.1016/0305-4179(95)90779-y. [DOI] [PubMed] [Google Scholar]
- 2.Rabbitts A, Alden NE, Conlin T, Yurt RW. Car radiator burns: a prevention issue. J Burn Care Rehabil. 2004;25(5):452–455. doi: 10.1097/01.bcr.0000138292.02559.a1. [DOI] [PubMed] [Google Scholar]
- 3.Barillo DJ, Cioffi WG, McManus WF, Pruitt BA Jr. Thermal trauma resulting from motor vehicle operation or maintenance. Accid Anal Prev. 1995;27(6):829–833. doi: 10.1016/0001-4575(95)00024-0. [DOI] [PubMed] [Google Scholar]
- 4.Baker AA, Attalla MF, Ekiabi SA, Al Ghoul A. Car radiator burns: a report on 72 cases. Burns. 1989;15(4):265–267. doi: 10.1016/0305-4179(89)90047-8. [DOI] [PubMed] [Google Scholar]
- 5.O’Neil N, Purdue G, Hunt J. Burns caused by automobile radiators: a continuing problem. J Burn Care Rehabil. 1992;13(4):422–425. doi: 10.1097/00004630-199207000-00007. [DOI] [PubMed] [Google Scholar]
- 6.Sözen I, Guldogan CE, Kismet K, Sabuncuoğlu MZ, Yasti AC. Outpatient burn management and unnecessary referrals. Ulus Travma Acil Cerrahi Derg. 2015;21(1):27–33. doi: 10.5505/tjtes.2015.89217. [DOI] [PubMed] [Google Scholar]
- 7.Benmeir P, Rosenberg L, Sagi A, Ben-Yakar Y. Radiator scald burns: a preventable hazard. Burns. 1990;16(2):135–136. doi: 10.1016/0305-4179(90)90174-u. [DOI] [PubMed] [Google Scholar]
- 8.Renz BM, Sherman R. Automobile carburetor- and radiator-related burns. J Burn Care Rehabil. 1992;13(4):414–421. doi: 10.1097/00004630-199207000-00006. [DOI] [PubMed] [Google Scholar]