

Summary
The aim of the present study was to examine burn patient health status, quality of life and work status 16.2 (1.7) [mean (SD)] years after burn injury, and to compare the findings with similar questionnaire data from the same people obtained 11.5 years earlier. Data on burn-specific health (BSHS-N), generic health (SF-36), overall quality of life (QOLS), injury characteristics, socio-demography and work were obtained in 2001 from 95 adult burn patients. In 2013, 78 participants were still eligible, and 34 of them (age: 53.4 [9.4] [mean (SD)], total body surface burn: 17.8% [12.7%]; full thickness injury: 4.4% [5.1%]) answered a follow up study. In 2001, the burn patients reported impaired health status, but an overall quality of life comparable to the Norwegian general population. In particular, the participants were satisfied with their close relationships. At follow up 11.5 years later, the perceived burn-specific and generic health remained unchanged, whereas overall quality of life had improved significantly (QOLS score 77.2 (10.2) vs. 73.1 (12.1), p=0.003), with the largest improvements in the items related to satisfaction with helping others, work, physical active pastimes and independence. The results indicate that self-perceived functioning and wellbeing expressed by burn-specific and generic health status remain stable after the first years post injury. The improvement in overall quality of life 16.2 years post injury suggests long-term processes of growth.
Keywords: burns, health, quality of life, outcome
Abstract
Le but de cette étude était d’évaluer l’état de santé, la qualité de vie et le rapport au travail 16,2 ± 1,7 ans après une brûlure, et de comparées ces données à celles obtenues auprès des mêmes patients 11,5 ans plus tôt. Les données spécifiques (BSHS-N) et générales (SF36) sur la qualité de vie, celles la brûlures, socio-démographiques et liées au travail avaient été colligées auprès de 95 brûlés adultes en 2001. Soixante dix huit d’entre eux étaient encore susceptibles de participer à l’étude en 2013, et 34 d’entre eux ont accepté de la faire. Ils étaient âgés de 53,4+/-9,4 ans, avaient été brûlés sur 17,8+/-12,7 % dont 4,4+/-5,1 % de profond. En 2001, ils considéraient que leur santé était atteinte mais les données de qualité de vie étaient comparables à celles de la population norvégienne. En particulier, les patients étaient satisfaits des relations avec leurs proches. Onze ans et demi plus tard, leur perception de leur santé, via les échelles spécifique aux brûlés comme générale, était inchangée quand l’amélioration de leur qualité de vie était significative (score QOL 77,2+/-10,2 VS 73,1+/- 12,1 ; p=0,03), les améliorations les plus nettes concernant leur capacité à aider autrui, le travail, l’activité physique de loisir et l’indépendance. Ce résultats indiquent que la perception de santé reste inchangée après les premières années suivant la brûlure quand l’amélioration de la qualité de vie 16,2 ans après suggère un processus évoluant sur le long terme.
Introduction
Major burns may have long lasting impact on the quality of people’s lives, with persisting problems related to scarring, contractures, weakness, thermoregulation, itching, pain, sleep, body image and psychosocial wellbeing.1 In addition to the direct consequences of the burn, the intensive care treatment may also cause cognitive, affective or behavioural challenges.2 Consistently, burn injured individuals have reported limitations in health-related quality of life compared to general population norms.3-8
Factors affecting perceived outcomes are related to the severity of burn injury, patient personality and mechanisms of coping, and the socio-economic and living situation of the patient. The extent of full thickness injury, number of operations, location of injury to face hands and feet, impaired hand function and joint contractures have all been reported as injury-specific threats to patient self-perceived health.3,5,7,9,11 Moreover, pain and discomfort, pre- and post-injury psychopathology and substance abuse seem to impair health and functioning.5,6,11,12 Partnership, living situation and employment are also factors strongly associated with self-reported functioning and wellbeing after burns.5,9,13 On the other hand, social support, self-efficacy, optimism, resilience or feelings of post-traumatic growth seem to improve perceived recovery after burns.3,14,15
Improvements in self-perceived physical and psychological health status, as well as quality of life, are to be expected the first months and years after discharge.4,6,7,16-20 The largest improvements have been reported in questionnaire subscales related to moving, usual activities, hand function, work and treatment regimens, whereas problems with heat sensitivity, body image and work have been documented to give the largest burn-specific problems.8,19-21 Compared to general population norms, burn patients seem to experience significant limitations related to pain/discomfort, usual activities, self-care and anxiety/depression (as assessed by the questionnaire EQ5D),6,7 as well as in physical functioning, role performance, body pain, social functioning and general health (as assessed by the questionnaire SF-36). 3,5,8 Overall, impairment of physical health status seems to already improve substantially in the first few months after burn injury, whereas mental health status seems to be more stable in the first phase of recovery, with possible improvements in the following years.4,6,7
The recovery pattern after burns is dynamic and not yet fully understood, and few follow up studies with observation time more than 10 years have been published. The present study is a follow up of a survey 11.5 years earlier on patient perceived health and quality of life after burn injury.5,22 In this study health was defined according to the World Health Organisation as: “A state of complete physical, mental and social wellbeing and not merely the absence of disease and infirmity”,23 whereas overall quality of life was operationally defined as: “Satisfaction with physical and material wellbeing, relations to others, social and community activities, personal development, fulfilment and recreation, as well as independence”.24 In 2001, the participants reported impaired health compared to general population norms, whereas their overall quality of life was comparable to age and gender adjusted findings from the Norwegian general population.5 The extent of full thickness injury, location of full thickness injury to face or foot, chronic pain, psychological illness, non-burn physical illnesses, unemployment and single living significantly limited the experience of health.5,22 The same factors were also significantly associated with reduced overall quality of life, except for the burn-specific factors on extent and location of burn injury.5
Knowledge on the dynamics and trajectories of recovery may be of value for our understanding of the impact of burn injury and the need for long term follow up and support from the burn team. The specific aim of this study was to examine burn-specific and generic health status, quality of life and work status 16.2 years after burn injury, and to compare the findings with similar questionnaire data from the same people 11.5 years earlier.
Materials and methods
Participants
All adult patients, 18 years or older, and admitted for burn injury to the national Burn Centre, Haukeland University Hospital, Bergen, Norway from 1995 to 2000 were included in the questionnaire study, and data collected in 2001 was used.5,22,25 Ninety-five patients agreed to take part an average 47 (SD: 23.8) months after injury. In 2013, 82 participants from the same study were still alive. Patients who had been in hospital less than two days (n=4) were excluded, leaving 78 participants eligible for the follow-up study.
Clinical characteristics and questionnaire data
Data on injury characteristics and treatment were obtained from medical records. Demographic information and data on patients’ reported burn-specific health, generic health and overall quality of life were obtained from questionnaires completed by the participants at each time point of inquiry.
The Norwegian version of the abbreviated Burn-Specific Health Scale (BSHS-N) was used to obtain information on burn-specific health status.25 BSHS-N comprises 80 items divided into four domains, asking for physical (20 items), mental (30 items), social (15 items) and general health (15 items), and the first three domains are again divided into seven subdomains.
The Physical Health domain comprises the subdomains Mobility and Self-care (10 items), Hand Function (5 items) and Role Activities (5 items). The Mental Health domain consists of the subdomains Body Image (7 items) and Affective (23 items).
The Social Health domain includes the two subdomains Family and Friends (12 items) and Sexual Activity (3 items). Responses to the items are given on a scale from 0 (extremely) to 4 (not at all). The answers were given as percentages of maximum scores (0-100) for the whole questionnaire or each domain or subdomain, where higher scale scores indicate better burn-specific health. One item of the questionnaire asking for suicidal thoughts (item 35) was omitted and replaced by a calculated mean of the mental health domain at follow up because of the offensive nature of the question and length of time after injury.
The Norwegian version of the SF-36 questionnaire was used to assess burn patient reported generic health.5,26,27 The instrument has been validated in a burn population.28 The SF-36 comprises 36 items addressing eight different health concepts, with the domains Physical Functioning, Role Physical, Body Pain, Mental Health, Role Emotional, Social Functioning, Vitality and General Health. The answers were transformed into scale scores 0-100 for each of the SF-36 domains, where higher scores represent better self-perceived health status.26 Overall quality of life was assessed by the Norwegian version of The Quality of Life Scale (QOLS).5,24,29 The questionnaire consists of 16 items asking for degree of satisfaction with important aspects of people’s lives. The answers are given on a seven point scale, from very dissatisfied to very satisfied. The total sum score was transformed into a 0-100 scale score, in which higher scores represent better overall quality of life.
Analysis
When comparing sample characteristics between responders and non-responders, Mann-Witney U-tests were used for the non-parametric and t-test for the parametric continuous data. Furthermore, Chi-square tests were used to test sample characteristics for the qualitative categorical data. Because of the small sample size and answers given on ordinal scales, nonparametric tests were chosen for the patient reported outcome data.30 Comparison of patient reported outcome scores between 2001 and 2013, and comparisons of SF-36 outcomes with age and gender specific general population norms were conducted by related sample Wilcoxon signed ranked tests.30,31 In order to identify factors associated with limitation in health and quality of life, Spearman’s rho correlation was used to test bivariate correlation between non-parametric continuous variables, and Mann-Whitney U test for comparison of health and quality of life between participants working or not.30,32All p-values were two-sided, and p > 0.05 was considered statistically significant. The statistical package SPSS version 19 (SPSS Inc., Ill., USA) was used for the analyses.
Ethics and approval
The study was performed according to The Code of Ethics of the World Medical Association (Declaration of Helsinki). All participants signed a letter of informed consent, which included permission to store information and take contact for a follow up study. The study was approved by the Regional Committee for Medical and Health Research Ethics (2001 and 2013/105/REK Vest), the Norwegian Registry of Data-Security (2001) and the Norwegian Directorate for Health and Social Welfare (2001).
Results
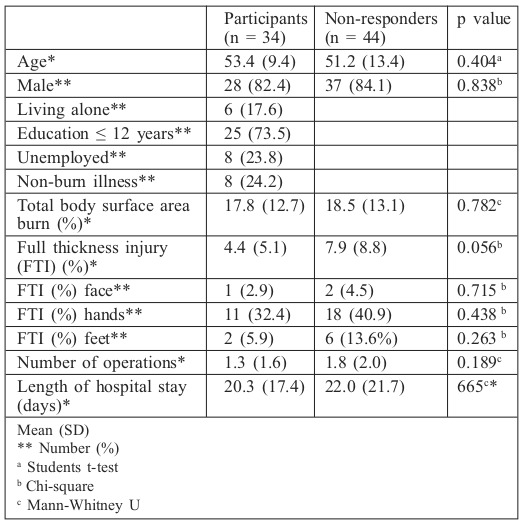
Out of 78 eligible patients, 34 (age 37-74 years) answered the follow-up study, giving a response rate of 43.6% and a time since injury of 16.2 (1.7) [mean (SD)] years. The majority were men, and average total body surface area burned was 17.8% (Table I). There were no significant differences between responder and non-responder age, gender or injury severity (Table I). Furthermore, in 2001 responders and non-responders reported similar levels of health and quality of life outcomes (not shown), except for the SF-36 domain Social functioning, in which the participants answering the follow-up study had better scores than the non-responders (mean 88.6 (SD 17.8) vs. mean 77.0 (SD 26.7), p=0.042).
Table I. Participant characteristics.
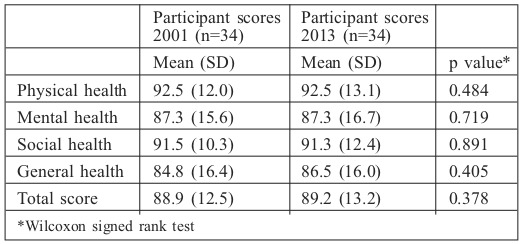
At follow up in 2013, self-reported burn-specific health status had not changed over the past 11.5 years (Table II). The lowest BSHS-N scores were in the two subdomains role-activities and affective, and the general health domain. Answers to single items on the BSHS-N revealed that the 10 lowest scores were for items on work performance, physical active pastimes, loss of energy, loss of strength, loss of old friends, itching, emotional problems and worries about own health. Eight participants (23.5%) still reported itching to some or a great extent, and 9 (26.5%) still had intrusive thoughts and images of the accident.
Table II. Burn-specific health status (BSHS-N).
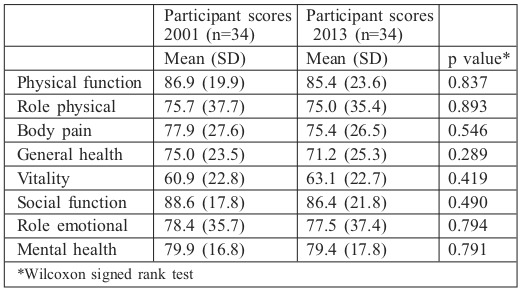
For generic health, there were no significant differences in SF-36 scores between the 2001 and 2013 measurements (Table III). Self-evaluation of own general health was the domain showing the biggest change, with a 4-point decrease. Vitality had the biggest positive change (2.2 point increase). In 2013, the SF-36 scores were not significantly different to age and gender matched population norms.31
Table III. Generic health status (SF-36).
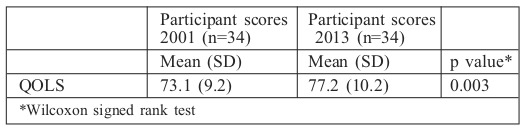
Notably, overall quality of life had improved significantly over the 11.5 years to follow up (Table IV). The biggest improvements were in items related to satisfaction with physical active pastimes, independence, work and helping and encouraging others.
Table IV. Overall quality of life (QOLS).
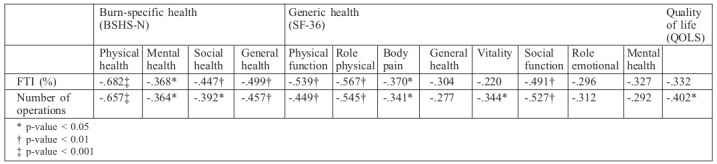
At follow up, there were still significant associations between extent of full thickness injury or number of operations in the acute phase of burn care and reduced scores in all domains of BSHS-N, as well as in physical functioning, physical role performance, body pain, vitality and social functioning of the SF-36 (Table V). The number of operations was also significantly associated with reduced overall quality of life at follow up.
Table V. Relationship between burn injury characteristics and patient reported health and quality of life.
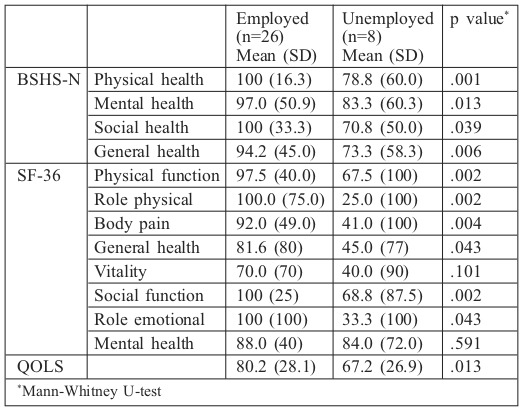
The percentage of participants not working at follow up was 23% (Table I). Being employed was important for perceived health and quality of life, and participants not working had significantly reduced scores in all health status domains and overall quality of life, except for the SF-36 domains mental health and vitality (Table VI). Moreover, 14 participants (42.1%) reported having a better job than before, nine participants (27.3%) had experienced work accommodations and eight had completed re-education (23.5%) after their burn injury.
Table VI. The effect of work status on health and quality of life.
Discussion
The main findings of this study are that 16.2 years post injury, self-perceived burn-specific and generic health status remained stable compared to data from the same participants 11.5 years earlier, whereas overall quality of life had improved significantly. This is consistent with earlier studies, indicating that the largest perceived improvements of burn patient health occur during the first years after discharge,4,16 and suggests that after this initial period of improvement, many burn patients experience persisting reductions in burn-specific and generic health.4,7,20 The present study indicates that in spite of a stable health status, satisfaction with life seems to steadily improve at least 15 years post-injury.
At follow up, the role-activities subdomain scores were the lowest in BSHS-N, suggesting persisting challenges with work performance and physical active past-times.9,20,33 Consistently, limitations with regard to work performance was the single item with the lowest score.
This is in accordance with earlier findings indicating that major burn injuries may be a larger threat to complex functioning than to self-care activities.9 Moreover, loss of strength and emotional problems were among the single items with the lowest scores, a finding that may indicate impaired role fulfillment and an association between emotional distress and burn-specific health status.16 Furthermore, about one in four participants still reported to have disturbing thoughts and memories from the accident.
Intrusive memories are a component of post-traumatic stress disorder, a condition associated with reduced health-related quality of life.7
Overall, the current findings on burn-specific health status 16.2 years after burn injury are comparable with findings from studies with substantially shorter observation periods.9,22,25
At follow up, disturbing itching persisted in about one in four participants. The majority of burn patients experience itching, and during the first years after injury itching can reportedly be predicted by number of surgical procedures and presence of post-traumatic stress symptoms.34 Even though the prevalence of itching seems to decrease with time, 44% of burn survivors have reported mild to moderate symptoms of pruritus between four to ten years after injury.35 The present study indicates that disturbing itching may persist for more than 15 years post burn in a significant fraction of patients.
In 2013, the 34 participants reported SF-36 scores similar to those they reported in 2001, suggesting stable generic health and a pattern of recovery similar to that of burn-specific health. Moreover, health status in 2013 was not significantly different to age and gender matched general population norms.31
This is in contrast with the findings from 2001, when data from the 95 participants demonstrated impairments in five out of eight domains of SF-36 compared to norms,5 but is most likely explained by a selection bias typically seen in longitudinal studies in which the most resourceful people remain in the study.
Overall quality of life improved significantly over the last 11.5 years, demonstrating a pattern different to that of burn-specific and generic health. Already in 2001, about four years post injury, the participants reported an overall quality of life comparable to that of the general population, with the greatest satisfaction related to close family relations.5
In 2013, the improvements were related to items involving physical active pastimes, independence, work and helping and encouraging others. The increased QOLS scores suggest a process of post burn growth that increases with time.36
Despite the overall positive health and quality of life outcomes, the extent of full-thickness injury, number of operations and unemployment were significantly associated with impairments of both burn-specific and generic health status and overall quality of life at follow up 16.2 years post injury. This is in accordance with earlier reports with observation periods shorter than that of the present study,5,9,13,22,37 and indicates burn-related consequences that should be followed up by longterm medical and vocational counseling.
This study is limited by the relatively small sample size, ut is strengthened by the long follow up period with measurements at two time points more than 10 years apart. The use of a combination of questionnaires also allowed for the assessment of both burn-specific and generic health, as well as overall quality of life, and how these parameters had developed over time.
Conclusion
The present study indicates that self-perceived burn-specific and generic health status remain stable after the first years post injury, whereas overall quality of life seems to steadily improve through a long-term process of growth. Future clinical and research efforts should aim to reduce the burden of fullthickness injuries and surgical procedures and at the same time facilitate multidisciplinary follow-up programs directed at promoting health and quality of life.38,39
Acknowledgments
Acknowledgements.The authors thank all the participating burn patients for their contribution to this study.
References
- 1.Esselman PC, Thombs BD, Magyar-Russell G, Fauerbach JA. Burn rehabilitation: state of the science. Am J Phys Med Rehabil. 2006;85:383–413. doi: 10.1097/01.phm.0000202095.51037.a3. [DOI] [PubMed] [Google Scholar]
- 2.Elliott D, Davidson JE, Harvey MA, Bemis-Dougherty A. Exploring the scope of post-intensive care syndrome therapy and care: engagement of non-critical care providers and survivors in a second stakeholders meeting. Crit Care Med. 2014;42:2518–2526. doi: 10.1097/CCM.0000000000000525. [DOI] [PubMed] [Google Scholar]
- 3.Anzarut A, Chen M, Shankowsky H, Tredget EE. Quality-of-life and outcome predictors following massive burn injury. Plast Reconstr Surg. 2005;116:791–797. doi: 10.1097/01.prs.0000176257.22583.4b. [DOI] [PubMed] [Google Scholar]
- 4.Fauerbach JA, Lezotte D, Hills RA, Cromes GF. Burden of burn: a norm-based inquiry into the influence of burn size and distress on recovery of physical and psychosocial function. J Burn Care Rehabil. 2005;26:21–32. doi: 10.1097/01.bcr.0000150216.87940.ac. [DOI] [PubMed] [Google Scholar]
- 5.Moi AL, Wentzel-Larsen T, Salemark L, Wahl AK. Impaired generic health status but perception of good quality of life in survivors of burn injury. J Trauma. 2006;61:961–968. doi: 10.1097/01.ta.0000195988.57939.9a. [DOI] [PubMed] [Google Scholar]
- 6.Oster C, Willebrand M, Ekselius L. Health-related quality of life 2 years to 7 years after burn injury. J Trauma. 2011;71:1435–1441. doi: 10.1097/TA.0b013e318208fc74. [DOI] [PubMed] [Google Scholar]
- 7.van Loey NE, van Beeck EF, Faber BW, van de Schoot R. Healthrelated quality of life after burns: a prospective multicenter cohort study with 18 months follow-up. J Trauma. 2012;72:513–520. doi: 10.1097/ta.0b013e3182199072. [DOI] [PubMed] [Google Scholar]
- 8.Xie B, Xiao SC, Zhu SH, Xia ZF. Evaluation of long term health-related quality of life in extensive burns: a 12-year experience in a burn center. Burns. 2012;38:348–355. doi: 10.1016/j.burns.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 9.Kildal M, Andersson G, Gerdin B. Health status in Swedish burn patients.Assessment utilising three variants of the Burn Specific Health Scale. Burns. 2002;28:639–645. doi: 10.1016/s0305-4179(02)00111-0. [DOI] [PubMed] [Google Scholar]
- 10.Leblebici B, Adam M, Bagis S, Tarim AM. Quality of life after burn injury: the impact of joint contracture. J Burn Care Res. 2006;27:864–868. doi: 10.1097/01.BCR.0000245652.26648.36. [DOI] [PubMed] [Google Scholar]
- 11.Palmu R, Partonen T, Suominen K, Saarni SI. Health-related quality of life 6 months after burns among hospitalized patients: Predictive importance of mental disorders and burn severity. Burns. 2015;41:742–748. doi: 10.1016/j.burns.2014.11.006. [DOI] [PubMed] [Google Scholar]
- 12.Low AJ, Dyster-Aas J, Willebrand M, Ekselius L. Psychiatric morbidity predicts perceived burn-specific health 1 year after a burn. Gen Hosp Psychiatry. 2012;34:146–152. doi: 10.1016/j.genhosppsych.2011.12.001. [DOI] [PubMed] [Google Scholar]
- 13.Dyster-Aas J, Kildal M, Willebrand M. Return to work and health-related quality of life after burn injury. J Rehabil Med. 2007;39:49–55. doi: 10.2340/16501977-0005. [DOI] [PubMed] [Google Scholar]
- 14.Wallis H, Renneberg B, Ripper S, Germann G. Emotional distress and psychosocial resources in patients recovering from severe burn injury. J Burn Care Res. 2006;27:734–741. doi: 10.1097/01.BCR.0000238094.33426.0D. [DOI] [PubMed] [Google Scholar]
- 15.Bosmans MW, Hofland HW, De Jong AE, Van Loey NE. Coping with burns: the role of coping self-efficacy in the recovery from traumatic stress following burn injuries. J Behav Med. 2015;38:642–651. doi: 10.1007/s10865-015-9638-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cromes GF, Holavanahalli R, Kowalske K, Helm P. Predictors of quality of life as measured by the Burn Specific Health Scale in persons with major burn injury. J Burn Care Rehabil. 2002;23:229–234. doi: 10.1097/00004630-200205000-00016. [DOI] [PubMed] [Google Scholar]
- 17.Klein MB, Lezotte DC, Heltshe S, Fauerbach S. Functional and psychosocial outcomes of older adults after burn injury: results from a multicenter database of severe burn injury. J Burn Care Res. 2011;32:66–78. doi: 10.1097/BCR.0b013e318203336a. [DOI] [PubMed] [Google Scholar]
- 18.Edgar DW, Homer L, Phillips M, Gurfinkel R. The influence of advancing age on quality of life and rate of recovery after treatment for burn. Burns. 2013;39:1067–1072. doi: 10.1016/j.burns.2013.05.017. [DOI] [PubMed] [Google Scholar]
- 19.Oster C, Willebrand M, Ekselius L. Burn-specific health 2 years to 7 years after burn injury. J Trauma. 2013;74:1119–1124. doi: 10.1097/TA.0b013e318283cca0. [DOI] [PubMed] [Google Scholar]
- 20.Wasiak J, Paul E, Lee SJ, Mahar P. Patterns of recovery over 12 months following a burn injury in Australia. Injury. 2014;45:1459–1464. doi: 10.1016/j.injury.2014.02.018. [DOI] [PubMed] [Google Scholar]
- 21.Koljonen V, Laitila M, Sintonen H, Roine RP. Health-related quality of life of hospitalized patients with burns-comparison with general population and a 2-year follow-up. Burns. 2013;39:451–457. doi: 10.1016/j.burns.2012.07.024. [DOI] [PubMed] [Google Scholar]
- 22.Moi AL, Wentzel-Larsen T, Salemark L, Hanestad BR. Long-term risk factors for impaired burn-specific health and unemployment in patients with thermal injury. Burns. 2007;33:37–45. doi: 10.1016/j.burns.2006.06.002. [DOI] [PubMed] [Google Scholar]
- 23.World Health Organization. Constitution of the World Health Organization. ‘Basic Documents’, Geneva, WHO Executive Board and World Health Assembly. 2006 [Google Scholar]
- 24.Burckhardt CS, Anderson KL, Archenholtz B, Hagg O. The Flanagan Quality of Life Scale: Evidence of Construct Validity. Health Qual Life Outcomes. 2003;1:59. doi: 10.1186/1477-7525-1-59. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Moi AL, Wentzel-Larsen T, Salemark L, Hanestad B. Validation of a Norwegian version of the Burn Specific Health Scale. Burns. 2003;29:563–570. doi: 10.1016/s0305-4179(03)00146-3. [DOI] [PubMed] [Google Scholar]
- 26.Ware JE, Kosinski M, Gandek B. ‘SF-36 health survey manual & interpretation guide. QualityMetric Inc. 2000 [Google Scholar]
- 27.Loge JH, Kaasa S, Hjermstad MJ, Kvien TK. Translation and performance of the Norwegian SF-36 Health Survey in patients with rheumatoid arthritis. I. Data quality, scaling assumptions, reliability, and construct validity. J Clin Epidemiol. 1998;51:1069–1076. doi: 10.1016/s0895-4356(98)00098-5. [DOI] [PubMed] [Google Scholar]
- 28.Edgar D, Dawson A, Hankey G, Phillips M. Demonstration of the validity of the SF-36 for measurement of the temporal recovery of quality of life outcomes in burns survivors. Burns. 2010;36:1013–1020. doi: 10.1016/j.burns.2010.03.001. [DOI] [PubMed] [Google Scholar]
- 29.Wahl AK, Rustoen T, Hanestad BR, Lerdal A. Quality of life in the general Norwegian population, measured by the Quality of Life Scale (QOLS-N) Qual Life Res. 2004;13:1001–1009. doi: 10.1023/B:QURE.0000025583.28948.5b. [DOI] [PubMed] [Google Scholar]
- 30.Polit DF, Beck CT. Nursing research: generating and assessing evidence for nursing practic. Wolters Kluwer Health. 2012 [Google Scholar]
- 31.Loge JH, Kaasa S. Short form SF 36 (SF-36) health survey: normative data from the general Norwegian population. Scand J Soc Med. 1988;26:250–258. [PubMed] [Google Scholar]
- 32.Kinnear PR, Gray CD. SPSS 12 made simple. Psychology Press. 2004 [Google Scholar]
- 33.Renneberg B, Ripper S, Schulze J, Seehausen A. Quality of life and predictors of long-term outcome after severe burn injury. J Behavior Med. 2014;37:967–976. doi: 10.1007/s10865-013-9541-6. [DOI] [PubMed] [Google Scholar]
- 34.Van Loey NE, Bremer M, Faber AW, Middelkoop E. Itching following burns: epidemiology and predictors. Br J Dermatol. 2008;158:95–100. doi: 10.1111/j.1365-2133.2007.08278.x. [DOI] [PubMed] [Google Scholar]
- 35.Carrougher GJ, Martinez EM, McMullen KS, Fauerbach JA. Pruritus in adult burn survivors: postburn prevalence and risk factors associated with increased intensity. J Burn Care Res. 2013;34:94–101. doi: 10.1097/BCR.0b013e3182644c25. [DOI] [PubMed] [Google Scholar]
- 36.Baillie SE, Sellwood W, Wisely JA. Post-traumatic growth in adults following a burn. Burns. 2014;40:1089–1096. doi: 10.1016/j.burns.2014.04.007. [DOI] [PubMed] [Google Scholar]
- 37.Wasiak J, Lee SJ, Paul E, Mahar P. Predictors of health status and health-related quality of life 12 months after severe burn. Burns. 2014;40:568–574. doi: 10.1016/j.burns.2014.01.021. [DOI] [PubMed] [Google Scholar]
- 38.Stergiou-Kita M, Grigorovich A, Gomez M. Development of an interprofessional clinical practice guideline for vocational evaluation following severe burn. Burns. 2014;40:1149–1163. doi: 10.1016/j.burns.2014.01.001. [DOI] [PubMed] [Google Scholar]
- 39.Wiechman SA, Carrougher GJ, Esselman PC, Klein MB. An expanded delivery model for outpatient burn rehabilitation. J Burn Care Res. 2015;36:14–22. doi: 10.1097/BCR.0000000000000153. [DOI] [PubMed] [Google Scholar]