
Figure 1.
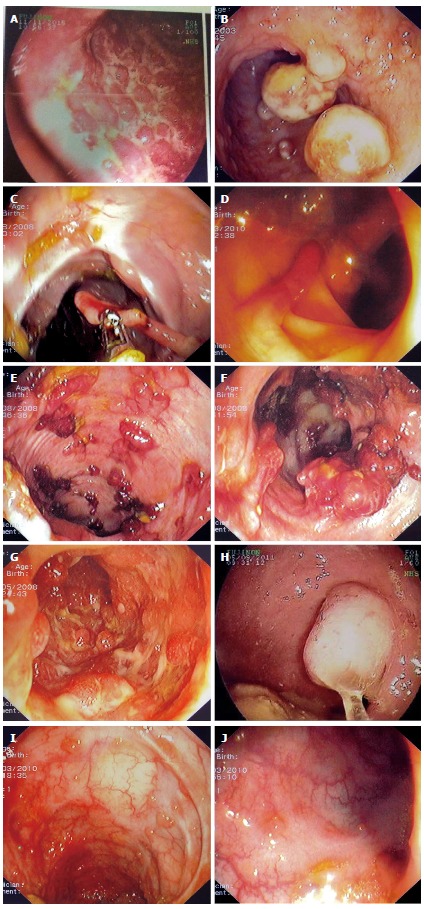
Examples of various types of pseudopolyps in different patients with inflammatory bowel disease. A: Endoscopic picture of deep ulcers and residual islets of surviving mucosa, the "true" pseudopolyps; B: Localized pseudopolyps of varying size up to 1.6 cm with discrete borders, pale surface, exudates on surface and varying forms. Biopsy of the polyps revealed inflammatory infiltration of lymphocytes, distortion and branching of the crypts compatible with post inflammatory pseudopolyps; C: Long filiform pseudopolyp located in the transverse colon captured with biopsy forceps; D: Localized filiform pseudopolyposis located in sigmoid colon; E: Post-inflammatory generalized pseudopolyposis; F: Cluster of pseudopolyps in sigmoid colon with 2.5 cm size, creating a giant localized pseudopolyp. Multiple biopsies of the polyp showed lined epithelium with a core of connective tissue and vessels with inflammatory infiltration which confirmed the diagnosis of pseudopolyp; G: Multiple pseudopolyps stubble the sigmoid colon. In this case, surveillance for dysplasia-associated lesion or mass can be challenging because of the intense inflammation and the multiple pseudopolyps; H: Pseudopolyp or adenoma-like mass? Solitary polyp with 1.5 cm size and broad-based with discrete borders but without exudates, amenable to endoscopic removal and having a pale surface. Histology after removal of the polyp with electrocautery showed villous adenoma with mild dysplasia, and without dysplasia in the surrounding mucosa or elsewhere in the colon, compatible with adenoma-like mass; I: Localized post-inflammatory pseudopolyps; J: Localized pseudopolyps of 0.3 cm maximum size, located in sigmoid colon with discrete borders and pale, glistering surface. Endoscopic characteristics were adequate for recognition of pseudopolyps without the need for biopsies or further intervention.