
Fig. 1.
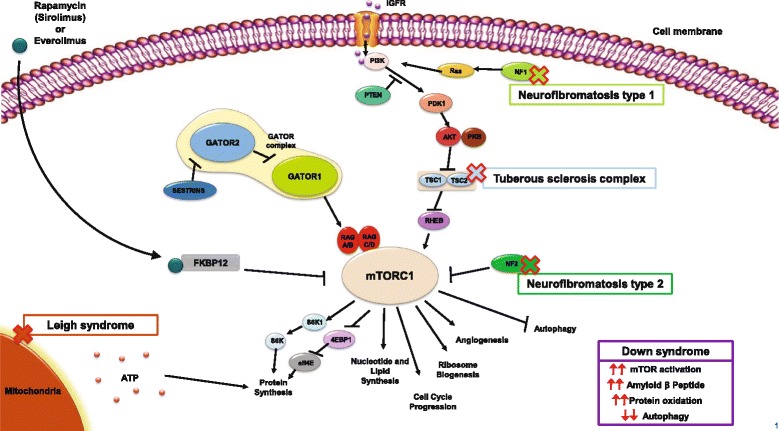
The mammalian target of rapamycin (mTOR) signaling pathway and possible involvement of rare diseases in the pathway. Stimulants such as insulin-like growth factor bind to tyrosine kinase receptors, which leads to the phosphorylation of phosphatidylinositol 3-kinase (PI3K) [23]. A cascade of subsequent phosphorylation events results in the activation of protein kinase B (AKT), which in turn phosphorylates and inhibits the TSC1/TSC2 complex, a negative regulator of mTOR that is directed against the positive regulator Ras homolog enriched in brain (Rheb). As a result, inhibition of the TSC1/TSC2 complex results in the activation of mTOR [23–25]. NF1-encoded neurofibromin and NF2-encoded Merlin proteins also act as negative regulators of the mTOR pathway. Neurofibromin functions as a Ras-GTPase activating protein that inhibits the actions of Ras on PI3K [26], while Merlin acts directly on mTOR complex 1 (mTORC1) [27]. Sirolimus and everolimus both bind to and form complexes with FK506-binding protein-12 (FKBP12), resulting in the inhibition of mTORC1 activity [24]. While mechanisms are complex and not fully clear in Leigh and Down syndrome, evidence has shown a relationship between mTOR activity and ATP (Leigh syndrome), and decreased autophagy with increased protein production and oxidation with mTOR hyperactivation (Down syndrome) [62, 65, 66]