

Abstract
Previous research offers evidence that psychological factors influence an injured athlete during the rehabilitation process. Our first objective was to conduct a systematic review and meta-analysis of the results from all published studies that examined the relationships among negative affective responses after sport injuries, rehabilitation adherence, and return to play (RTP). The second objective was to use a meta-analytic path analysis to investigate whether an indirect effect existed between negative affective responses and RTP through rehabilitation adherence. This literature review resulted in seven studies providing 14 effect sizes. The results from the meta-analysis showed that negative affective responses had a negative effect on successful RTP, whereas rehabilitation adherence had a positive effect on RTP. The results from the meta-analytic path analysis showed a weak and nonsignificant indirect effect of negative affective responses on RTP via rehabilitation adherence. These results underline the importance of providing supportive environments for injured athletes to increase the chances of successful RTP via a decrease in negative affective responses and increase in rehabilitation adherence.
Keywords: affective responses, rehabilitation behaviors, return to play, sport injuries
Introduction
Sport injuries are a major problem related to sport participation.1–3 Research has shown that injuries can have major negative consequences on an athlete’s athletic career (e.g., career termination)4,5 and can severely affect his/her well-being.6–8 Given the potential negative outcomes related to sport injuries, one important aspect of sport injury rehabilitation is to facilitate the rehabilitation process to increase the chances of a successful rehabilitation outcome. To better understand the factors that might influence both the rehabilitation process and the likelihood of return to play (RTP), several theoretical frameworks have been developed. One theoretical framework developed to explain responses to sport injuries and the recovery process following sport injuries is the dynamic biopsychosocial cycles of post sport injury response and recovery framework.9 According to this framework, an athlete’s interpretation of the situation of being injured will influence the magnitude of negative affective responses. The magnitude of negative affective responses is, in turn, suggested to influence an athlete’s behaviors (e.g., rehabilitation adherence). An athlete’s choice of behaviors will then be related to the rehabilitation outcomes (e.g., RTP). During the past 10 years, interest in psychological factors’ influences on the rehabilitation process and outcomes has progressively increased. This increased interest has resulted in several published review articles.10–15 One of the main conclusions of these reviews is that negative psychological responses can decrease the likelihood of a successful RTP.
In these review articles, however, only the direct effects of psychological variables on rehabilitation outcomes were examined; indirect effects have so far been neglected in the literature. This is a bit surprising because biological and rehabilitation behaviors have been suggested to mediate the relationship between psychological factors and rehabilitation outcomes.9,13 Given the suggestion that behaviors (e.g., rehabilitation adherence) mediate the relationship between psychological factors (e.g., affective responses) and rehabilitation outcomes (e.g., RTP), it is of interest to test the empirical support for this assumption.
Our first objective was to conduct a systematic review and meta-analysis of the results from all published studies that examined the relationships between negative affective responses after a sport injury, rehabilitation adherence, and RTP. The second objective was to use a meta-analytic path analysis to investigate the indirect effect of negative affective responses on RTP through rehabilitation adherence.
Methods
Literature search
We searched the electronic databases of Science Direct, Web of Science, PubMed, and PsycINFO using combinations of the following keywords: “sport injury”, “psychology”, “return to play”, and “return to sport”. Boolean expressions and MeSH terms were used along with truncations adjusted to each database’s guidelines. In addition, we searched published review articles for additional studies.10–15
Studies were considered for inclusion if: 1) they had used prospective or cross-sectional designs; 2) they were published in peer-review journals; 3) they were written in English; 4) the athletes were injured when the first psychometric data were collected; and 5) they investigated any of the relationships between negative affective responses, adherence to rehabilitation, and RTP. In our study, different criteria were used for data extraction. The specific negative responses that Wiese-Bjornstal9 listed guided the selection of negative affective responses. For adherence to rehabilitation, subjective or objective reports on adherence to a prespecified rehabilitation plan were considered an inclusion criterion. RTP was defined as the length of time from the injury to the time when the athlete was playing sports again. One of the included studies, however, used a slightly different definition. Heredia et al16 defined RTP as the length of time between the date when the athlete was declared medically fit and the date when the athlete returned to play. The Heredia et al study was, however, relevant to our research question and it was therefore included despite using a slightly different RTP definition. Effect sizes were calculated for relationships among the variables of interest (i.e., negative affective responses, adherence to rehabilitation, RTP). The full literature search process is illustrated in Figure 1, and a summary of all studies included in the meta-analysis is reported in Table 1.
Figure 1.
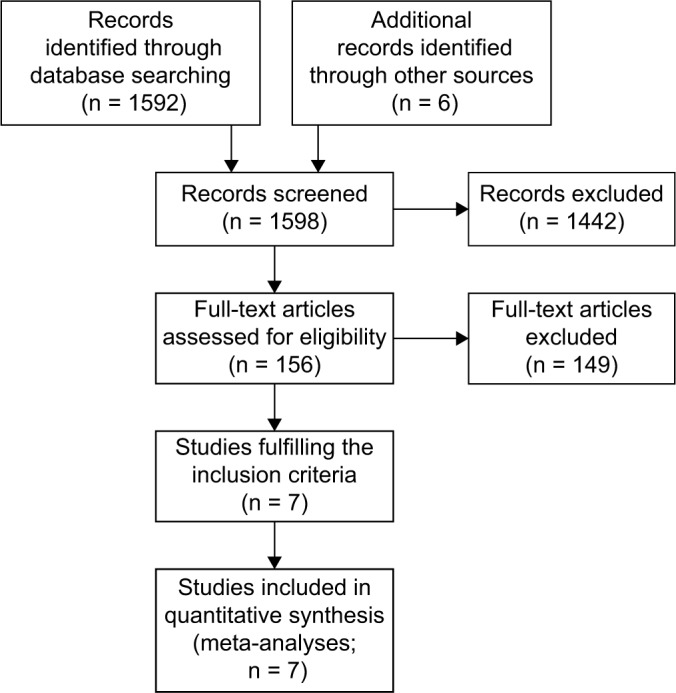
Description of the selection process for included studies.
Table 1.
Overview of the studies included in the meta-analysis
| Study | Design | Population | n | Injuries | Variables | Definition of RTP |
|---|---|---|---|---|---|---|
| Brewer et al35 | Prospective study | Competitive and recreational athletes | 95 | Acute ACL injury | Negative responses, adherence | NA |
| Heredia et al16 | Prospective study | Competitive athletes | 20 | All types of injuries | Negative responses, adherence, RTP | The period between the date when the athlete was declared medically fit and the data on which the athlete returned to play |
| Lentz et al36 | Prospective study | Injured athletes | 60 | Acute ACL injury | Negative responses, RTP | RTP |
| Lu and Hsu37 | Cross-sectional study | Collegiate student athletes | 224 | All types of injuries | Negative responses, adherence | NA |
| Muller et al38 | Prospective study | Injured athletes | 40 | Acute ACL injury | Negative responses, RTP | RTP 7 months after surgery |
| Podlog et al39 | Cross-sectional study | High-school students (study 1), collegiate athletes (study 2) | 118 (study 1) 105 (study 2) |
All types of injuries | Negative responses, adherence | NA |
| Shin et al40 | Prospective study | Competitive athletes | 40 | All types of injuries | Adherence, RTP | RTP |
Note: n, sample size.
Abbreviations: RTP, return to play; ACL, anterior cruciate ligament; NA, not available.
An additional inclusion criterion was that the studies presented statistical data necessary for the calculation of zero-inflated Pearson’s r effect sizes. Common reasons for the exclusion of studies were as follows: 1) the psychometric data were collected retrospectively, after the athletes had returned to sport activities; 2) the outcome variable was subjective knee function; and 3) the studies were review articles.
Meta-analytic procedures
By applying a meta-analytic procedure to a systematic review procedure, it is possible to collectively test a statistical synthesis of research findings. We used the zero-inflated correlation coefficients as effect-size estimates. In the calculation of the coefficients for the relationships among the three variables of interest, we first transformed all effect sizes to Fisher’s z correlations. In the second step, we corrected the Fisher’s z correlations by weighting the sample-size estimates. In the third step, we used the weighted Fisher’s z correlations to calculate the average Fisher’s z correlation for the relationships among the three variables. Fourth, we transformed the average Fisher’s z correlation into zero-inflated standardized correlation coefficients. For all calculations, we used the Comprehensive Meta-Analysis software.17 The results are reported using mean effect sizes (r) or beta (β) values in combination with 95% confidence intervals (CIs). A result of p < 0.05 was considered to be statistically significant.
We used the I2 statistic as a measure of heterogeneity among studies. The I2 estimate indicates the degree of inconsistency among the magnitudes of the coefficients within each category of relationships. We calculated a fail-safe number (FSN) for each relationship tested in the meta-analysis. The FSN is used to indicate how many additional studies with mean null results would be needed to reduce the combined statistical significance to a specific alpha level (e.g., 0.05).
Both Wiese-Bjornstal9 and Brewer13 suggested that rehabilitation adherence potentially mediates the relationship between psychological variables and rehabilitation outcomes, and a meta-analytic path analysis is a useful approach for testing this proposed indirect association. To test the indirect effect of negative affective responses on RTP via rehabilitation adherence, we conducted a meta-analytic path analysis within a meta-analysis structural equation modeling (MASEM) framework.18 Prior to the analysis, we inserted the zero-inflated correlation coefficients into a correlation matrix. Based on this correlation matrix, we used Mplus version 7.419 to conduct the path analysis. To test the indirect effect, the Sobel method with a 95% CI was used. In addition, in line with previous recommendations, we used the harmonic mean as the sample size in our analysis.20
Results
An overview of the study characteristics, heterogeneity assessment, and FSNs is provided in Tables 1 and 2. The results from the meta-analysis showed a negative and statistically significant relationship between negative affective responses after sport injury and RTP (r = −0.32, 95% CI [−0.42, −0.21]). Moreover, the relationship between rehabilitation adherence and RTP was positive and statistically significant (r = 0.54, 95% CI [0.34, 0.69]).
Table 2.
Results of meta-analyses and homogeneity tests for the relationships between negative responses after injury, rehabilitation adherence, and return to sport
| Relationship | k | n | Effect size (r) | 95% CI | FSN | I2(%) |
|---|---|---|---|---|---|---|
| Negative responses-rehabilitation adherence | 9 | 1058 | −0.11 | −0.15, 0.07 | 20 | 20 |
| Negative responses-return to sport | 3 | 120 | −0.32 | −0.42, −0.21 | 7 | 0 |
| Rehabilitation adherence-return to sport | 2 | 60 | 0.54 | 0.34, 0.69 | NA | 0 |
Notes: k, number of effect sizes; n, total number of participants.
Abbreviations: CI, confidence interval; FSN, fail-safe number; NA, not available.
The results from the meta-analytic path analysis showed a statistically significant effect of negative affective responses on RTP (β = −0.26, 95% CI [−0.41, −0.12], p < 0.001). Also, a positive and statistically significant effect of rehabilitation adherence on RTP (β = 0.51, 95% CI [0.38, 0.64], p < 0.001) was found. Negative affective responses had a small and not statistically significant effect on rehabilitation adherence (β = −0.11, 95% CI [−0.29, 0.07], p = 0.23). Negative affective responses and rehabilitation adherence explained 36.0% of the variance in RTP, whereas negative affective responses explained 1.2% of the variance in rehabilitation adherence. The indirect effect of negative affective responses on RTP via rehabilitation adherence was small and not statistically significant (standardized estimate = −0.06, 95% CI [−0.15, 0.04], p = 0.23).
Discussion
Both negative affective responses after injury occurrence and rehabilitation adherence had direct effects on RTP. More specifically, low levels of negative affective responses and high compliance with a rehabilitation program were associated with a higher likelihood of successful RTP. In addition, the results showed a weak, and not statistically significant, indirect effect of negative affective responses on RTP.
The negative effect of negative affective responses on RTP has been found in previous studies.21 One potential explanation for this relationship is that psychological stress seems to influence the wound-repair process.22 More specifically, a meta-analysis showed a strong negative relationship between psychological distress and wound healing.23 High stress levels are, for example, associated with physiological stress responses.24 These stress responses can, in turn, retard the inflammatory phase and increase the risk of infection.22 Another potential explanation for the relationship is that low levels of negative affective responses, such as anxiety and fear, will increase the likelihood of an athlete’s having confidence in the formerly injured body part.25 An athlete with confidence in his/her body is probably more likely to return to sports at an earlier stage than an athlete who is not confident in that the body will cope with the physical load related to participation in the sport activity.
Only two of the studies included in the meta-analysis focused on the relationship between rehabilitation adherence and RTP. The magnitude of this effect should therefore be interpreted with caution. Nevertheless, a strong positive effect of rehabilitation adherence on RTP was found. Compliance with a rehabilitation program, recommended by a physiotherapist, is one important aspect related to an increased chance of RTP.26 Adhering to the recommended training program will increase the chance of the injured body part to recover and heal, which in turn will increase the chance of a successful comeback.
The path analysis showed that negative affective responses and rehabilitation adherence explained 36.0% of the variance in RTP. This result underlines the importance of considering psychological and behavioral factors in the injury rehabilitation process. There was a marginal, and not statistically significant, indirect effect of negative affective responses on RTP via rehabilitation adherence. This result contradicts the suggestion that behaviors will mediate the effect of negative affective responses on recovery as proposed in the dynamic biopsychosocial cycles of post sport injury response and recovery framework.9 That psychological factors (e.g., emotions) have a causal, but often indirect, influence on behaviors has been shown in numerous studies in psychology.27 The lack of a direct effect between negative affective responses and rehabilitation adherence (negative affective responses explained 1.2% of the variance in rehabilitation adherence) suggests that other variables might influence this relationship. Although a weak relationship (i.e., small effect size) was found between negative affective responses and rehabilitation adherence, associations might still exist between affective responses and other adaptive behaviors (e.g., help seeking, coping). Research on potentially adaptive behaviors other than rehabilitation adherence is warranted in future research.
Limitations and methodological considerations
This study has several limitations and methodological considerations that we want to address. First, the meta-analysis contains a small number of effect sizes. In particular, the estimate for the relationship between rehabilitation adherence and RTP as well as between negative affective responses and RTP (ks = 2 and 3) should be interpreted with caution because it is associated with low power.28 Nevertheless, research has highlighted that the meta-analyses of a few studies may still provide important information.29 Second, because few effect sizes were included in the analyses, no moderation analysis was possible to perform. Third, our decision to have RTP as our only rehabilitation outcome might have excluded studies that measured other relevant outcomes (e.g., knee function, pain). The reason for this decision was that we wanted to have an objective outcome that is meaningful for all members in the sporting community. Fourth, because we were interested in investigating both the direct and indirect paths among negative affective responses, rehabilitation adherence, and the dependent variable of RTP, we used a saturated model. The limitation of a saturated model is that it is impossible to evaluate model fit because this type of model always has perfect fit to data. A saturated model can be used if a researcher is “interested in estimating certain model parameters, with associated measures of instability.”30
Conclusion and practical recommendations
The results showed that both negative affective responses and rehabilitation adherence are related to a successful RTP after a sport injury. More specifically, both low levels of negative affective responses and high compliance with a rehabilitation plan were predictors of a successful RTP. Athletes should, therefore, work with stress management techniques to decrease the level of negative affective responses during the rehabilitation process, which in previous research has been related to successful rehabilitation outcomes.31,32 Learning to take responsibility and to view an injury as a challenge instead of as a threat (problem-focused coping) has been one successful strategy. For practitioners, it is important to design an environment that decreases negative affective responses and maximizes rehabilitation adherence. A high-quality social support system and autonomous motivation have been suggested as important factors for enhancing rehabilitation adherence and decreasing negative affective responses.33,34 We therefore suggest that information about how to create a supportive environment should be included in education modules for coaches, physiotherapists, and other practitioners working with injured athletes.
Footnotes
Disclosure
The authors report no conflicts of interest in this work.
References
- 1.Hägglund M, Waldén M, Ekstrand J. Injuries among male and female elite football players. Scand J Med Sci Sports. 2009;19(6):819–827. doi: 10.1111/j.1600-0838.2008.00861.x. [DOI] [PubMed] [Google Scholar]
- 2.Salman AF. Comparison of injuries between male and female handball players in junior and senior teams. Swed J Sci Res. 2014;1(4):1–15. [Google Scholar]
- 3.Tranaeus U, Johnson U, Engström B, Skillgate E, Werner S. A psychological injury prevention group intervention in Swedish floorball. Knee Surg Sports Traumatol Arthrosc. 2015;23(11):3414–3420. doi: 10.1007/s00167-014-3133-z. [DOI] [PubMed] [Google Scholar]
- 4.Stambulova N, Stephan Y, Järphag U. Athletic retirement: a cross-national comparison of elite French and Swedish athletes. Psychol Sport Exerc. 2007;8:101–118. [Google Scholar]
- 5.Park S, Lavallee D, Tod D. Athletes’ career transitions out of sport: a systematic review. Int Rev Sport Exerc Psychol. 2013;6:22–53. [Google Scholar]
- 6.Hagger MS, Chatzisarantis NLD, Griffin M, Thatcher J. Injury representations, coping, emotions, and functional outcomes in athletes with sports-related injuries: a test of self-regulation theory. J Appl Sport Psychol. 2005;35(11):2345–2374. [Google Scholar]
- 7.Drawer S, Fuller CW. Propensity for osteoarthritis and lower limb joint pain in retired professional soccer players. Br J Sports Med. 2001;35(6):402–408. doi: 10.1136/bjsm.35.6.402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Lohmander LS, Englund PM, Dahl LL, Roos EM. The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am J Sports Med. 2007;35(10):1756–1769. doi: 10.1177/0363546507307396. [DOI] [PubMed] [Google Scholar]
- 9.Wiese-Bjornstal DM. Psychology and socioculture affect injury risk, response, and recovery in high-intensity athletes: a consensus statement. Scand J Med Sci Sports. 2010;20(suppl 2):103–111. doi: 10.1111/j.1600-0838.2010.01195.x. [DOI] [PubMed] [Google Scholar]
- 10.Ardern CL, Taylor NF, Feller JA, Webster KE. A systematic review of the psychological factors associated with returning to sport following injury. Br J Sports Med. 2013;47(17):1120–1126. doi: 10.1136/bjsports-2012-091203. [DOI] [PubMed] [Google Scholar]
- 11.Forsdyke D, Smith A, Jones M, Gledhill A. Psychosocial factors associated with outcomes of sports injury rehabilitation in competitive athletes: a mixed studies systematic review. Br J Sports Med. 2016;50(9):537–544. doi: 10.1136/bjsports-2015-094850. [DOI] [PubMed] [Google Scholar]
- 12.Ardern C, Kvist J, Webster KE. Psychological aspects of anterior cruciate ligament injuries. Oper Tech Sports Med. 2016;24(1):77–83. [Google Scholar]
- 13.Brewer BW. The role of psychological factors in sport injury rehabilitation outcomes. Int Rev Sport Exerc Psychol. 2010;3:40–61. [Google Scholar]
- 14.Podlog L, Heil J, Schulte S. Psychosocial factors in sports injury rehabilitation and return to play. Phys Med Rehabil Clin N Am. 2014;25(4):915–930. doi: 10.1016/j.pmr.2014.06.011. [DOI] [PubMed] [Google Scholar]
- 15.Hamson-Utley JJ, Vazquez L. The comeback: rehabilitating the psychological injury. Athlet Ther Today. 2008;13(5):35–38. [Google Scholar]
- 16.Heredia RAS, Munox AR, Artaza JL. The effect of psychological response on recovery of sport injury. Res Sports Med. 2004;12(1):15–31. [Google Scholar]
- 17.Borenstein M, Hedges L, Higgins J, et al. Comprehensive Meta Analysis. Englewood: Biostat; 2009. [Google Scholar]
- 18.Card NA. Applied Meta-Analysis for Social. Science Research; New York, NY: Guilford Press; 2011. [Google Scholar]
- 19.Muthén L, Muthén B. Mplus User’s Guide. Vol. 6. Los Angeles, CA: Muthén & Muthén; 1998. [Google Scholar]
- 20.Viswesvaran C, Ones DS. Theory testing: combining psychometric meta-analysis and structural equations modeling. Pers Psychol. 1995;48(4):865–885. [Google Scholar]
- 21.Bauman J. Returning to play: the mind does matter. Clin J Sport Med. 2005;15(6):432–435. doi: 10.1097/01.jsm.0000186682.21040.82. [DOI] [PubMed] [Google Scholar]
- 22.Gouin J-P, Kiecolt-Glaser JK. The impact of psychological stress on wound healing: methods and mechanisms. Immunol Allergy Clin North Am. 2011;31(1):81–93. doi: 10.1016/j.iac.2010.09.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Walburn J, Vedhara K, Hankins M, Rixon L, Weinman J. Psychological stress and wound healing in humans: a systematic review and metaanalysis. J Psychosom Res. 2009;67(3):253–271. doi: 10.1016/j.jpsychores.2009.04.002. [DOI] [PubMed] [Google Scholar]
- 24.Lupien SJ, McEwen BS, Gunnar MR, Heim C. Effects of stress throughout the lifespan on the brain, behavior and cognition. Nat Rev Neurosci. 2009;10(6):434–445. doi: 10.1038/nrn2639. [DOI] [PubMed] [Google Scholar]
- 25.Podlog LW, Banham SM, Wadey R, Hannon J. Psychological readiness to return to competitive sport following injury: a qualitative study. Sport Psychol. 2015;29(1):1–14. [Google Scholar]
- 26.Bizzini M, Hancock D, Impellizzeri F. Suggestions from the field for return to sports participation following anterior cruciate ligament reconstruction: soccer. J Orthop Sports Phys Ther. 2012;42(4):304–312. doi: 10.2519/jospt.2012.4005. [DOI] [PubMed] [Google Scholar]
- 27.Baumeister RF, DeWall CN, Vohs KD, Alquist JL. Does emotion cause behavior (apart from making people do stupid, destructive things)? In: Agnew CR, Carlston DE, Graziano WG, Kelly JR, editors. Then a Miracle Occurs: Focusing on Behavior in Social Psychological Theory and Research. New York, NY: Oxford; 2010. pp. 119–136. [Google Scholar]
- 28.Valentine JC, Pigott TD, Rothstein HR. How many studies do you need? A primer on statistical power for meta-analysis. J Educ Behav Stat. 2010;35(2):215–247. [Google Scholar]
- 29.Goh JX, Hall JA, Rosenthal R. Mini meta-analysis of your own studies: some arguments on why and a primer on how. Soc Pers Psychol Compass. 2016;10:535–549. [Google Scholar]
- 30.Raykov T, Lee C-L, Marcoulides GA, et al. A commentary on the relationship between model fit and saturated path models in structural equation modeling applications. Educ PsycholMeas. 2013;73(6):1054–1068. [Google Scholar]
- 31.Cupal D, Brewer B. Effects of relaxation and guided imagery on knee strength, re-injury anxiety, and pain following anterior cruciate ligament reconstruction. RehabilPsychol. 2001;46:28–43. [Google Scholar]
- 32.Johnson U. Short-term psychological intervention: a study of long-term-injured competitive athletes. JSport Rehabil. 2000;9:207–218. [Google Scholar]
- 33.Chan DK, Lonsdale C, Ho PY, Yung PS, Chan KM. Patient motivation and adherence to postsurgery rehabilitation exercise recommendations: the influence of physiotherapists′ autonomy-supportive behaviors. Arch Phys Med Rehabil. 2009;90(12):1977–1982. doi: 10.1016/j.apmr.2009.05.024. [DOI] [PubMed] [Google Scholar]
- 34.Johnson U, Ivarsson A, Karlsson J, Hägglund M, Waldén M, Bärjesson M. Rehabilitation after first-time anterior cruciate ligament injury and reconstruction in female football players: a study of resilience factors. BMC Sports Sci Med Rehabil. 2016;8:20. doi: 10.1186/s13102-016-0046-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Brewer BW, Van Raalte JL, Cornelius AE, et al. Psychological factors, rehabilitation adherence, and rehabilitation outcome after anterior cruciate ligament reconstruction. Rehabil Psychol. 2000;45(1):20–37. doi: 10.1037/a0031297. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lentz TA, Zeppieri G, Jr, George SZ, et al. Comparison of physical impairment, functional, and psychosocial measures based on fear of reinjury/lack of confidence and return-to-sport status after ACL reconstruction. Am J Sports Med. 2015;43(2):345–353. doi: 10.1177/0363546514559707. [DOI] [PubMed] [Google Scholar]
- 37.Lu FJ, Hsu Y. Injured athletes’ rehabilitation beliefs and subjective well-being: the contribution of hope and social support. J Athl Train. 2013;48(1):92–98. doi: 10.4085/1062-6050-48.1.03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Müller U, Krüger-Franke M, Schmidt M, Rosemeyer B. Predictive parameters for return to pre-injury level of sport 6 months following anterior cruciate ligament reconstruction surgery. Knee Surg Sports TraumatolAdthrosc. 2015;23(12):3623–3631. doi: 10.1007/s00167-014-3261-5. [DOI] [PubMed] [Google Scholar]
- 39.Podlog L, Gao Z, Kenow L, et al. Injury rehabilitation overadherence: preliminary scale validation and relationships with athletic identity and self-presentation concerns. J Athl Train. 2013;48(3):372–381. doi: 10.4085/1062-6050-48.2.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Shin JT, Park R, Song WI, Kim SH, Kwon SM. The redevelopment and validation of the rehabilitation adherence questionnaire for injured athletes. Int J Rehabil Res. 2010;33(1):64–71. doi: 10.1097/MRR.0b013e32832fea39. [DOI] [PubMed] [Google Scholar]