

Abstract
Aims
The Intraosseous Transcutaneous Amputation Prosthesis (ITAP) may improve quality of life for amputees by avoiding soft-tissue complications associated with socket prostheses and by improving sensory feedback and function. It relies on the formation of a seal between the soft tissues and the implant and currently has a flange with drilled holes to promote dermal attachment. Despite this, infection remains a significant risk. This study explored alternative strategies to enhance soft-tissue integration.
Materials and Methods
The effect of ITAP pins with a fully porous titanium alloy flange with interconnected pores on soft-tissue integration was investigated. The flanges were coated with fibronectin-functionalised hydroxyapatite and silver coatings, which have been shown to have an antibacterial effect, while also promoting viable fibroblast growth in vitro. The ITAP pins were implanted along the length of ovine tibias, and histological assessment was undertaken four weeks post-operatively.
Results
The porous titanium alloy flange reduced epithelial downgrowth and increased soft-tissue integration compared with the current drilled flange. The addition of coatings did not enhance these effects.
Conclusion
These results indicate that a fully porous titanium alloy flange has the potential to increase the soft-tissue seal around ITAP and reduce susceptibility to infection compared with the current design.
Cite this article: Bone Joint J 2017;99-B:393–400.
Keywords: Amputation, Soft-tissue integration, Transcutaneous, Prosthesis
The Intraosseous Amputation Prosthesis (ITAP) (Stanmore Implants Worldwide Ltd, Elstree, United Kingdom) is an osseointegrated, transcutaneous titanium alloy implant that penetrates the skin to attach an external prosthesis. It avoids many of the common problems of conventional socket prostheses, such as discomfort, excessive perspiration, pressure sores caused by non-uniform pressure distribution over the stump and the need for repeated fittings due to poor fit.1-3 Osseointegrated transcutaneous prostheses are able to avoid these problems because the forces that would be encountered by the soft tissues of the stump with the use of a socket prosthesis are transferred directly to the skeleton.
Achievement of a seal between the soft tissues and the implant is necessary to avoid infection. Soft-tissue attachment to the implant prevents epithelial downgrowth (the migration of epithelial cells downwards and parallel to the side of the implant), which may lead to marsupialisation (pocket-formation) of the soft tissues and thereby a route for organisms to enter the underlying soft tissues.4 In order to achieve soft-tissue integration, fibroblasts must win the ‘race for the surface’ against bacteria. The ‘race for the surface’ describes the competition between eukaryotic cell and bacterial adhesion on the implant’s surface.5,6 In the case of ITAP, fibroblasts need to adhere to the surface before bacteria. If fibroblasts win the ‘race’, the implant would be covered by a cellular layer, making the surface less available for bacterial attachment. This would lead to successful tissue integration. However, bacteria may win the ‘race’ establishing biofilm formation, which may be difficult to eradicate. The current ITAP design has a flange with drilled holes to increase soft-tissue integration. Infection, nevertheless, remains a risk.
This study aimed to investigate if surface modifications and coatings could improve soft-tissue integration by enabling fibroblasts to win the ‘race for the surface’ against bacteria. Fully porous titanium (i.e. with interconnected pores) has been shown to increase tissue integration, as pores allow migration and proliferation of cells, ingrowth of blood vessels and consequently tissue formation within the porous structure.7,8 Other osseointegrated prosthetic designs have shown improvements in soft-tissue integration with porous-coated implants, but have not eliminated the problem of marsupialisation.9 A fully porous ITAP flange has not previously been investigated. Fibronectin-functionalised hydroxyapatite (HAFn) has been shown to enhance in vitro fibroblast adhesion and, when applied to drilled-holed implants, has improved in vivo soft-tissue integration.10,11 However, it is known that bacteria often adhere to surfaces that promote soft-tissue integration and therefore, the presence of an antimicrobial coating during the early post-operative period before a robust seal has formed may be of value to prevent bacteria from adhering before fibroblasts attach. Silver has a broad spectrum of antimicrobial activity and can be incorporated into fibronectin-functionalised hydroxyapatite coatings using an electrochemical deposition technique.12,13 An advantage of the electrochemical deposition technique is that it may be used to coat complex structures (such as a porous flange). More commonly used line-of-sight techniques, such as plasma spraying, would not be able to do this.14 Fibronectin-functionalised hydroxyapatite coatings with silver (HAAgFn) have been shown to prevent bacterial colonisation while promoting viable fibroblast attachment in vitro.15
The hypothesis of this in vivo study is that a fully porous ITAP flange would increase soft-tissue integration over the current drilled-hole design and that HAAgFn coatings would further increase soft-tissue integration.
Materials and Methods
Transcutaneous pin designs and coatings
Transcutaneous pins with a laser-sintered porous titanium alloy flange (pore size 700 μm and strut size 300 μm, porosity 18%) (Eurocoatings, Trentino, Italy) were used (Fig. 1a, Table I). The flanges were either uncoated (PT) or coated with electrochemically deposited hydroxyapatite (PT-HA), hydroxyapatite (HA) with fibronectin (PT-HAFn), HA with silver (PT-HAAg) or HA with silver and fibronectin (PT-HAAgFn). The details of the surface preparation and electrochemical deposition process is available in the supplementary material. The current ITAP drilled-flange (DF) design, which consists of a flat flange with drilled holes (with a diameter of 700 μm) and a tapered intraosseous stem was used as a control (Fig. 1b, Table I). The flange and the stem are coated with plasma sprayed HA (Plasma Biotal Ltd, Buxton, United Kingdom). An uncoated straight pin (SP) without a flange was included as a control for the DF design.
Figs. 1a - 1b.
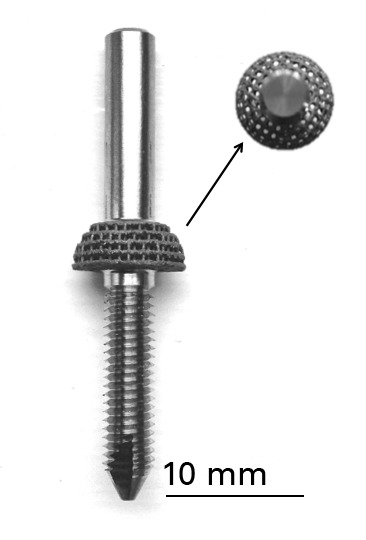
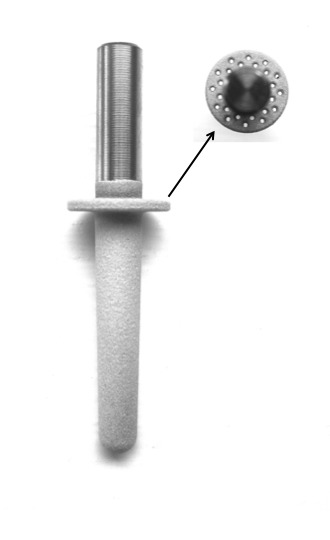
Diagrams showing an Intraosseous Amputation Prosthesis pin with a (a) porous titanium alloy flange and (b) drilled flange.
Table I.
Transcutaneous flanged-pin dimensions
| Dimension (mm) | PT | DF |
|---|---|---|
| Total pin length | 45 | 47 |
| Length of transcutaneous portion | 19.2 | 17 |
| Length of intraosseous portion | 21.5 | 29 |
| Flange length | 4.3 | 1 |
| Pin diameter | 5 | 5 |
| Flange diameter | 11 | 11 |
| Thread pitch | 0.8 | - |
| Core diameter | 4.2 | - |
PT, porous titanium alloy flange; DF, drilled flange
Surface characterisation
Scanning electron microscopy (SEM) was performed to visualise the surface topography and morphology of all coatings on the outer surface of the implants and to measure the thickness of HA and HAAg coatings on the outer surface of the implant and within the central pores. Energy-dispersive X-ray spectroscopy analysis was performed to determine the Ca/P ratio of HA coatings and to measure the atomic percentage of Ag within coatings. A full description of this technique is available in the supplementary material.
Silver release
The amount of silver released into fetal calf serum from PT-HAAg was measured over a four-week period, with PT-HA used as a control. The flanges were placed in 5 mL of fetal calf serum at room temperature. Flanges were removed at four, eight and 24 hours and then on days 2, 3, 4, 5, 8, 11, 14, 18 and 28. Flanges were placed into fresh fetal calf serum solution at each time point. Inductively Coupled Plasma Mass Spectrometry (ICP-MS) (Trace Element Laboratory, London, United Kingdom) was used to quantify the silver content in elution fluids.
Animal model
The study was performed under a Project License and a Personal License according to the United Kingdom Home Office Scientific Procedures Act 1986. Skeletally mature female sheep (mules) (n = 6) weighing between 66 kg and 88 kg were used. Transcutaneous pins were implanted along the length of the sheep tibia. Details of the surgical procedure are included in the supplementary material.
Hard grade resin-histological processing
The specimens were fixed in 10% formal saline. Following this, they underwent ascending graded alcohol dehydration and defatting in chloroform. They were embedded in LR White Resin (London Resin Company Ltd, Reading, United Kingdom). The histological sectioning process is described in the supplementary material.
Hard grade resin-histological analysis
Two sections were analysed for each implant. The following outcomes were measured:
- epithelial downgrowth (mm)
- percentage epithelial attachment
- percentage dermal attachment.
A line intercept method was used for these measurements (Fig. 2).4 The thickness of the epithelial and dermal tissue layers was measured and expressed as a percentage of the thickness of these layers in contact with the implant surface.
Fig. 2.

Schematic diagram showing the measurements for epithelial downgrowth, epithelial and subepithelial attachment for a flanged implant.
A semi-quantitative estimate was used to express the percentage of the pore filled with soft tissue and the density of the tissue within the pore compared with that outside it. Fibroblast nuclei within the inner pores were counted within a defined area and the number per mm2 calculated. The blood vessels within the inner pores were counted within a defined area and number of blood vessels per mm2 was calculated.
Statistical analysis
This was performed using SPSS version 21.0 software (IBM, Armonk, New York). The Kruskal-Wallis test was used to identify differences between groups. Paired Mann-Whitney U tests were used to determine differences between implant types. A p-value < 0.05 was considered statistically significant. Data are presented as median values and 95% confidence intervals (CI).
Results
Surface characterisation-surface topography, coating thickness and elemental composition
The electrochemically deposited coatings on the porous titanium alloy flanges contained a combination of plate-like, needle-shaped and globular crystals similar to that observed on solid discs in previous in vitro studies.15 SEM images are shown in Figure 3.
Figs. 3a - 3b.
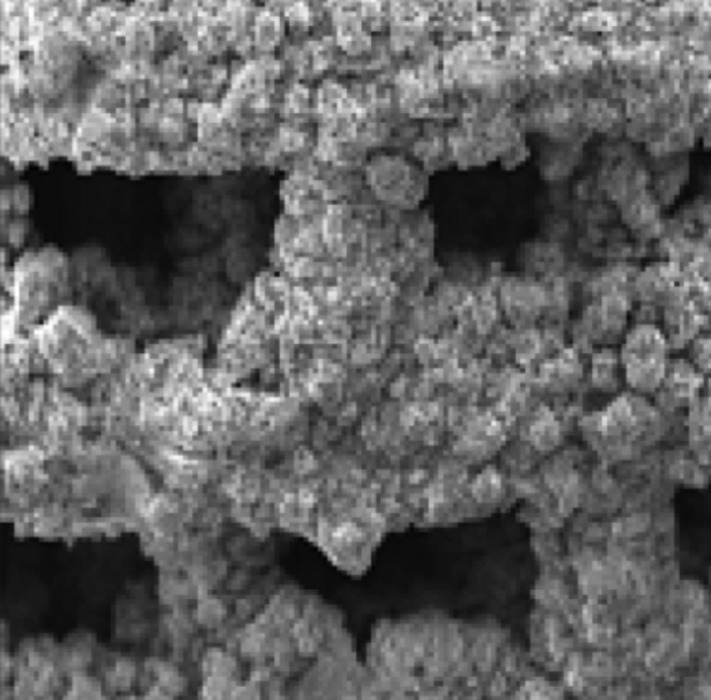
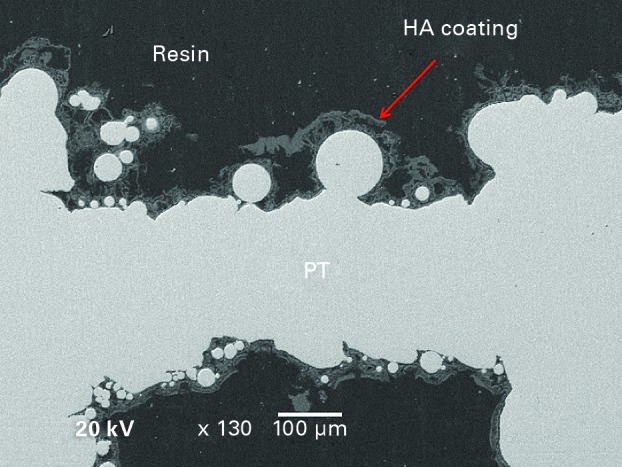
Scanning electron micrographs of (a) the outer surface of a hydroxyapatite (HA) with silver and fibronectin-coated implant (× 50 magnification) and (b) a section through the centre of a hydroxyapatite coated implant (PT) showing the coating on the innermost pores.
The median calcium:phosphate atomic percentage ratio for electrochemically deposited HA coatings was 1.74 (95% CI 1.62 to 1.86). This indicated that these HA coatings were close in composition to pure stoichiometric HA. The thickness of coatings is presented in Table II. Table III shows the silver atomic percentages of HAAg/Fn coatings.
Table II.
Thickness of coatings
| Surface | Coating thickness (μm) median value (95% confidence interval) |
|---|---|
| PT-HA (outer surface) | 47 (30 to 76) |
| PT-HA (inner pores) | 36 (12 to 55) |
| PT-HAAg (outer surface) | 56 (24 to 101) |
| PT-HAAg (inner pores) | 46 (31 to 82) |
PT-HA, hydroxyapatite coated flange; PT-HAAg, hydroxyapatite with silver coated flange
Table III.
Silver percentages within PT-HAAg and PT-HAAgFn coatings measured by energy-dispersive X-ray spectroscopy analysis
| Surface | Ag atomic % median value (95% confidence interval) |
|---|---|
| PT-HAAg | 0.700 (0.582 to 0.757) |
| PT-HAAgFn | 0.610 (0.591 to 0.652) |
PT-HAAg, hydroxyapatite with silver coated flange; PT-HAAgFn, hydroxyapatite with silver and fibronectin coated flange
Silver release
The silver release was greatest over the first 24 hours, and gradually reduced over time (4.14 μmol/L at 28 days). The rate of release was slowest between days 11 and 28. Silver continued to be released throughout the 28-day test period (Table IV).
Table IV.
The release of silver from hydroxyapatite with silver coated flange over 28 days
| Time (days) | Silver release (umol/L) median value (95% confidence interval) |
|---|---|
| 1 | 101.5810 (46.7192 to 163.9788) |
| 2 | 27.6840 (0.5311 to 60.5682) |
| 3 | 21.9790 (3.5346 to 43.1121) |
| 4 | 23.5450 (3.5155 to 40.7465) |
| 5 | 19.4430 (6.0237 to 31.2776) |
| 8 | 12.1270 (-1.5545 to 27.2212) |
| 11 | 5.3860 (2.6626 to 7.5661) |
| 14 | 4.3950 (1.4158 to 6.5149) |
| 18 | 3.5550 (0.6460 to 5.4300) |
| 28 | 4.1400 (-1.0457 to 7.7223) |
Soft-tissue integration-epithelial downgrowth
SP resulted in the greatest degree of epidermal downgrowth. DF reduced epithelial downgrowth compared with SP (DF = 4.2 mm, SP = 6.1 mm; Mann-Whitney U test, p < 0.001). PT reduced epithelial downgrowth compared with DF (Mann-Whitney U test, p = 0.027). The addition of coatings to PT did not result in any further reduction in epidermal downgrowth. PT-HAFn, PT-HAAg and PT-HAAgFn reduced epidermal downgrowth compared with DF (Mann-Whitney U test, p = 0.003, p = 0.017 and p = 0.001 respectively). The reduction in epidermal downgrowth conferred by the PT-HA coating compared with DF did not reach statistical significance (Mann-Whitney U test, p = 0.052) (Table V).
Table V.
Epithelial downgrowth measurements associated with each implant
| Surface | Epithelial downgrowth (mm) median value (95% confidence interval) |
|---|---|
| Straight pin | 6.0753 (5.2082 to 8.7915) |
| DF | 4.2043 (2.6040 to 4.3087) |
| PT | 1.2900 (0.9936 to 3.1139) |
| PT-HA | 1.7826 (1.2789 to 3.3195) |
| PT-HAFn | 1.7655 (1.2074 to 2.3601) |
| PT-HAAg | 1.7562 (0.9242 to 2.9181) |
| PT-HAAgFn | 1.7888 (1.3366 to 2.1510) |
DF, drilled flange; PT, uncoated porous titanium alloy flange; PT-HA, hydroxyapatite coated flange; PT-HAFn, hydroxyapatite with fibronectin coated flange; PT-HAAg, hydroxyapatite with silver coated flange; PT-HAAgFn, hydroxyapatite with silver and fibronectin coated flange
Soft-tissue integration-percentage epithelial attachment
The epithelium did not attach to the SP and this implant was therefore associated with the lowest median percentage epithelial attachment (0%, interquartile range (IQR) 0% to 0%). The DF had a greater median percentage epithelial attachment, which was highly variable between implants (63.4%, IQR 0% to 100%) (Mann-Whitney U test, p = 0.045). There was no difference between DF and PT implants, irrespective of coating (Kruskal-Wallis test, p = 0.859).
Soft-tissue integration-percentage dermal attachment
The DF showed greater median dermal attachment than the SP (DF = 56.4%, SP = 0%; Mann-Whitney U test, p = 0.017). The PT component had greater median dermal attachment than DF (PT = 80.5%; Mann-Whitney U test, p = 0.020), with the addition of coatings conferring no statistically significant improvements in dermal attachment. Improved attachment was seen in PT-HAFn compared with PT-HA (Mann-Whitney U test, p = 0.023) and in PT-HAAgFn compared with PT-HAAg (Mann-Whitney U test, p = 0.039) (Fig. 4). Histological sections are shown in Figure 5.
Fig. 4.

Box-and-whisker plot showing the percentage dermal attachment to implants (SP, straight pin; DF, drilled flange; PT, uncoated porous titanium alloy flange; PT-HA, hydroxyapatite coated flange; PT-HAFn, hydroxyapatite with fibronectin coated flange; PT-HAAg, hydroxyapatite with silver coated flange; PT-HAAgFn, hydroxyapatite with silver and fibronectin coated flange).
Figs. 5a - 5d.
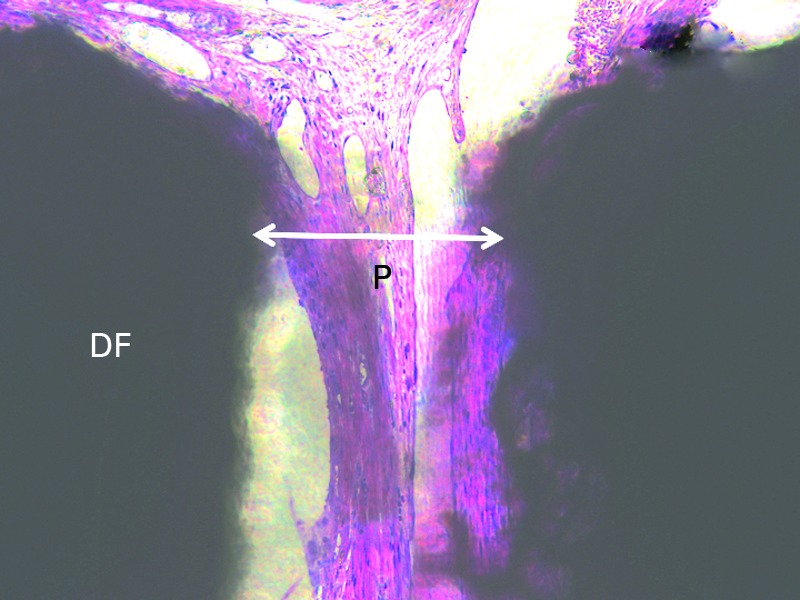
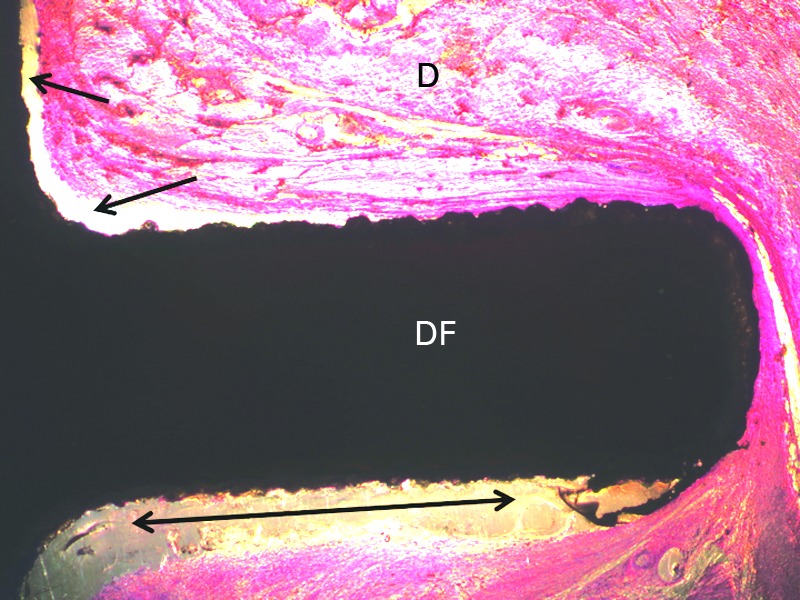
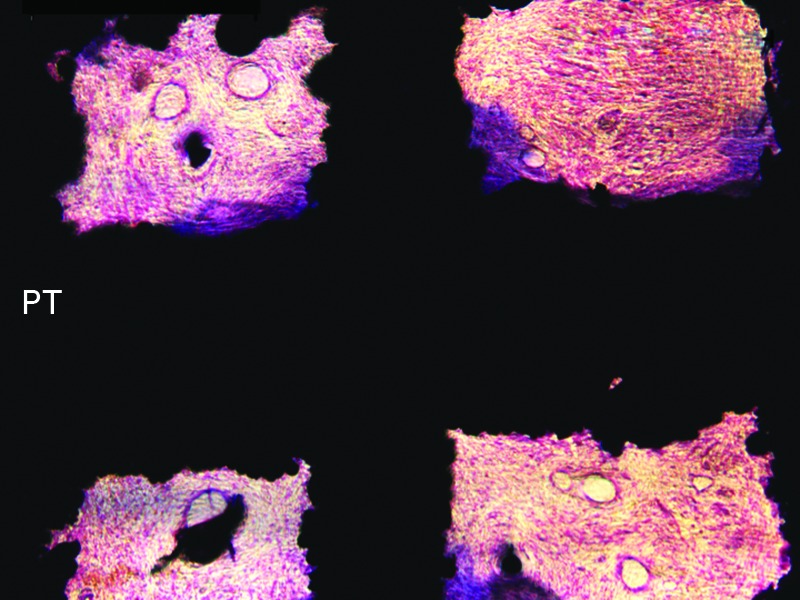

Histological sections showing (a) incomplete soft-tissue fill within a drilled flange (DF) pore (P); (b) areas of lack of the dermal tissue (D) attachment to the flange of a DF implant (arrows); (c) intimate contact between uncoated porous titanium alloy flange (PT) pore edges and soft-tissue PT. Increased collagen deposition is seen at the pore periphery and (d) the dermis attaching to hydroxyapatite with fibronectin coated flange flange.
Soft-tissue integration-percentage soft-tissue fill
The median percentage soft-tissue fill within the inner pores of PT was significantly greater than that of the DF (PT = 90%, DF = 65%; Mann-Whitney U test, p < 0.001). The addition of coatings did not result in any increases in percentage soft-tissue fill (Table VI). Histological sections are shown in Figure 5.
Table VI.
Number of cell nuclei/mm2 within the inner pores of each implant
| Surface | Cell nuclei/mm2median value (n, 95% confidence interval) |
|---|---|
| DF | 1520.5050 (1028.8516 to 2332.6951) |
| PT | 3922.6250 (2590.6413 to 5182.6021) |
| PT-HA | 2883.8250 (2029.4570 to 3891.7696) |
| PT-HAFn | 2945.8300 (2473.5655 to 3708.2709) |
| PT-HAAg | 3086.2450 (2595.8449 to 4017.1911) |
| PT-HAAgFn | 2606.3700 (1990.1559 to 4334.6132) |
DF, drilled flange; PT, uncoated porous titanium alloy flange; PT-HA, hydroxyapatite coated flange; PT-HAFn, hydroxyapatite with fibronectin coated flange; PT-HAAg, hydroxyapatite with silver coated flange; PT-HAAgFn, hydroxyapatite with silver and fibronectin coated flange
Soft-tissue integration-number of cell nuclei/mm2
There was a greater median density of cell nuclei within the inner pores of the PT flange than the DF (PT = 3922.6 mm2, DF = 1520.5 mm2; Mann-Whitney U test, p = 0.018). The addition of coatings was not associated with any change in density (Table VII).
Table VII.
Number of cell nuclei/mm2 within the inner pores of each implant
| Surface | Cell nuclei/mm2median value (n, 95% confidence interval) |
|---|---|
| DF | 1520.5050 (1028.8516 to 2332.6951) |
| PT | 3922.6250 (2590.6413 to 5182.6021) |
| PT-HA | 2883.8250 (2029.4570 to 3891.7696) |
| PT-HAFn | 2945.8300 (2473.5655 to 3708.2709) |
| PT-HAAg | 3086.2450 (2595.8449 to 4017.1911) |
| PT-HAAgFn | 2606.3700 (1990.1559 to 4334.6132) |
DF, drilled flange; PT, uncoated porous titanium alloy flange; PT-HA, hydroxyapatite coated flange; PT-HAFn, hydroxyapatite with fibronectin coated flange; PT-HAAg, hydroxyapatite with silver coated flange; PT-HAAgFn, hydroxyapatite with silver and fibronectin coated flange
Soft-tissue integration-number of blood vessels/mm2
There was a greater median density of blood vessels within the inner pores of the PT flange than the DF (PT = 213.2 mm2, DF = 0 mm2; Mann-Whitney U test, p = 0.002). Coatings did not result in further increases in blood vessel ingrowth.
Discussion
This study has shown for the first time that using a PT flange reduces epithelial downgrowth and increases dermal attachment and ingrowth of vascularised soft tissue into pores when compared with the standard drilled-hole ITAP flange. Other studies of the effect of porous titanium alloy on soft-tissue integration of transcutaneous pins have used porous coatings rather than a fully porous material, have assessed smaller pore sizes and have made comparisons with smooth implants rather than drilled-hole implants.9,16,17
The coatings did not show any statistically significant advantages over PT. The median dermal attachment of PT was 80% and the median soft-tissue fill was 90%. It may be difficult to achieve significant improvements or complete soft-tissue attachment with the animal model used in this study. In this study, the sheep were mobilised bearing full weight from the first post-operative day, which would create some movement at the skin-implant interface before the seal could form. In clinical practice in humans, there is a rest period where the implant is not loaded during the early wound-healing period. Increased bacterial exposure is also likely in an animal model, however, the sheep may have a higher resistance to bacterial infections than humans.
Although there were no statistically significant differences when coatings were added to PT, PT-HA lost some of the beneficial effects associated with PT. The reduction in epithelial downgrowth associated with PT-HA compared with DF was not statistically significant. PT with all other coatings significantly reduced epithelial downgrowth. Additionally, PT-HA was the only PT implant not associated with significantly improved blood vessel ingrowth compared with DF. The negative effect of HA may be due to increased bacterial colonisation when this coating is used on porous titanium, permitting bacteria to win the ‘race for the surface’.15 PT-HAFn did not have a negative effect although, similarly to HA, HAFn would be expected to promote adhesion of some bacterial strains.18-20 It is possible that when fibronectin is added to HA, despite its potential to increase bacterial colonisation, cells are able to win the ‘race for the surface’ due to early soft-tissue adherence allowing HAFn to overcome any loss of beneficial effects associated with HA.
Silver release was sustained over the 28 days at a slow rate indicating that the coating persists for 28 days. These were below levels that would cause systemic toxicity.21 The levels released remained above those shown to have bactericidal activity in vitro.12 HAAg coatings did not produce any adverse soft-tissue reactions suggesting that the levels of silver were safe. PT-HAAg was associated with increased vascularisation within the inner pores compared with PT-HA. Additionally, PT-HAAg/Fn maintained the beneficial effects that PT had on epithelial downgrowth and vascularity over DF that PT-HA had lost. This indicates that silver had some effect. The effect of silver coatings without HA or increasing the concentration of silver may have a different effect. It is possible that, despite not having a significant effect on soft-tissue attachment, silver could reduce bacterial colonisation, which could be of value in terms of preventing infection. If this were to be the case, the fact that this study has shown that there is no adverse soft-tissue reaction associated with silver, would be useful. Further data on bacterial colonisation on the implant surfaces in this study will be published separately.
It has been previously shown that if dermal attachment is achieved even without epithelial attachment, epithelial downgrowth is inhibited.4 Once epithelial downgrowth is prevented and keratinocytes in the epithelium come into contact with the implant surface, they may attach via hemidesmosomes and allow an epithelial seal to form in addition to the dermal seal.4,22,23 The porous flanges did not, however, significantly increase epithelial attachment, despite the increase in dermal attachment. Design modifications to increase epithelial attachment may be necessary, such as coating the transcutaneous portion of the implant with proteins that enhance keratinocyte attachment.23
There are several potential limitations of this study. Firstly, we measured soft-tissue contact rather than mechanical strength of attachment. However, other studies that have performed mechanical testing have shown that the histological findings support strength of attachment results.24,25 Secondly, the time period of four weeks for this study was short. It is known that as time increases soft-tissue attachment increases.24,26 The short time period which was selected as an assessment of early attachment is essential, as early soft-tissue attachment is the key factor affecting the outcome of the ‘race for the surface’.5,6 Longer periods of time would also make quantification of cell nuclei density challenging due to the proliferation of nuclei.
Although the main intended application of the findings from this research is for improving the success of ITAP, the findings could also be applied to other transcutaneous devices. For example, the addition of a porous flange to external fixator pins may have the potential to reduce infection rates by improving soft-tissue integration at the skin–implant interface. Furthermore, the coating HAAgFn may be more likely to produce favourable in vivo results for osseointegration than for soft-tissue integration due to the rough topography. Further investigation of porous metals coated with electrochemically deposited HAAg (with and without fibronectin) to assess the effect on osseointegration would be useful to determine if these coatings could play a role in preventing loosening and bacterial colonisation of the intraosseous portion of ITAP or for uncemented arthroplasty surgery. Additionally, this coating technique could be applied to endoprosthetic replacements with porous collars e.g. for tumour resection.
In conclusion, the results of this study indicate that a PT flange, without the addition of coatings, has the potential to increase the soft-tissue seal around ITAP, which would be expected to reduce the susceptibility of ITAP to infection compared with the current drilled-hole flange design. Further investigation of fibronectin and silver coatings without HA may be of value.
Take home message:
- A fully porous titanium alloy flange with interconnected pores improves soft-tissue integration. It reduces epithelial downgrowth and increases dermal attachment, cell nuclei density and blood vessel ingrowth compared with the current standard ITAP model.
- The addition of hydroxyapatite, silver and fibronectin coatings did not significantly improve soft-tissue integration.
- It is therefore postulated that a fully porous titanium alloy flange, without the addition of coatings, has the potential to reduce the susceptibility of ITAP to infection by increasing soft-tissue integration.
Footnotes
Supplementary material. Further information regarding the surface preparation, the surgical details and the histological section is included alongside the online version of this article at www.bjj.boneandjoint.org.uk.
References
- 1.Hagberg K, Brånemark R. Consequences of non-vascular trans-femoral amputation: a survey of quality of life, prosthetic use and problems. Prosthet Orthot Int 2001;25:186–194. [DOI] [PubMed] [Google Scholar]
- 2.Koc E, Tunca M, Akar A, et al. Skin problems in amputees: a descriptive study. Int J Dermatol 2008;47:463–466. [DOI] [PubMed] [Google Scholar]
- 3.Meulenbelt HE, Geertzen JH, Jonkman MF, Dijkstra PU. Skin problems of the stump in lower limb amputees: 1. A clinical study. Acta Derm Venereol 2011;91:173–177. [DOI] [PubMed] [Google Scholar]
- 4.Pendegrass CJ, Goodship AE, Blunn GW. Development of a soft tissue seal around bone-anchored transcutaneous amputation prostheses. Biomaterials 2006;27:4183–4191. [DOI] [PubMed] [Google Scholar]
- 5.Gristina AG. Biomaterial-centered infection: microbial adhesion versus tissue integration. Science 1987;237:1588–1595. [DOI] [PubMed] [Google Scholar]
- 6.Subbiahdoss G, Pidhatika B, Coullerez G, et al. Bacterial biofilm formation versus mammalian cell growth on titanium-based mono- and bi-functional coating. Eur Cell Mater 2010;19:205–213. [DOI] [PubMed] [Google Scholar]
- 7.Hulbert SF, Young FA, Mathews RS, et al. Potential of ceramic materials as permanently implantable skeletal prostheses. J Biomed Mater Res 1970;4:433–456. [DOI] [PubMed] [Google Scholar]
- 8.Kuboki Y, Takita H, Kobayashi D, et al. BMP-induced osteogenesis on the surface of hydroxyapatite with geometrically feasible and nonfeasible structures: topology of osteogenesis. J Biomed Mater Res 1998;39:190–199. [DOI] [PubMed] [Google Scholar]
- 9.Jeyapalina S, Beck JP, Bachus KN, Williams DL, Bloebaum RD. Efficacy of a porous-structured titanium subdermal barrier for preventing infection in percutaneous osseointegrated prostheses. J Orthop Res 2012;30:1304–1311. [DOI] [PubMed] [Google Scholar]
- 10.Pendegrass CJ, Middleton C, Blunn W. Fibronectin Functionalized Hydroxyapatite Coatings: Improving Dermal Fibroblast Adhesion In Vitro and In Vivo. Adv Eng Mater 2010;12:B365–B373. [Google Scholar]
- 11.Pendegrass CJ, El-Husseiny M, Blunn GW. The development of fibronectin-functionalised hydroxyapatite coatings to improve dermal fibroblast attachment in vitro. J Bone Joint Surg [Br] 2012;94-B:564–569. [DOI] [PubMed] [Google Scholar]
- 12.Ghani Y, Coathup MJ, Hing KA, Blunn GW. Development of a hydroxyapatite coating containing silver for the prevention of peri-prosthetic infection. J Orthop Res 2012;30:356–363. [DOI] [PubMed] [Google Scholar]
- 13.Brennan SA, Ní Fhoghlú C, Devitt BM, et al. Silver nanoparticles and their orthopaedic applications. Bone Joint J 2015;97-B:582–589. [DOI] [PubMed] [Google Scholar]
- 14.García-Gareta E, Hua J, Knowles JC, Blunn GW. Comparison of mesenchymal stem cell proliferation and differentiation between biomimetic and electrochemical coatings on different topographic surfaces. J Mater Sci Mater Med 2013;24:199–210. [DOI] [PubMed] [Google Scholar]
- 15.Chimutengwende-Gordon M, Pendegrass C, Bayston R, Blunn G. Preventing infection of osseointegrated transcutaneous implants: incorporation of silver into preconditioned fibronectin-functionalized hydroxyapatite coatings suppresses Staphylococcus aureus colonization while promoting viable fibroblast growth in vitro. Biointerphases 2014;9:031010. [DOI] [PubMed] [Google Scholar]
- 16.Isackson D, McGill LD, Bachus KN. Percutaneous implants with porous titanium dermal barriers: an in vivo evaluation of infection risk. Med Eng Phys 2011;33:418–426. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Farrell BJ, Prilutsky BI, Ritter JM, et al. Effects of pore size, implantation time, and nano-surface properties on rat skin ingrowth into percutaneous porous titanium implants. J Biomed Mater Res A 2014;102:1305–1315. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Dexter SJ, Pearson RG, Davies MC, Cámara M, Shakesheff KM. A comparison of the adhesion of mammalian cells and Staphylococcus epidermidis on fibronectin-modified polymer surfaces. J Biomed Mater Res 2001;56:222–227. [DOI] [PubMed] [Google Scholar]
- 19.Plotkowski MC, Filho MB, de Nazareth Meirelles M, Tournier JM, Puchelle E. Pseudomonas aeruginosa Binds to Soluble Cellular Fibronectin. Curr Microbiol 1993;26:91–95. [Google Scholar]
- 20.Bozzini S, Visai L, Pignatti P, Petersen TE, Speziale P. Multiple binding sites in fibronectin and the staphylococcal fibronectin receptor. Eur J Biochem 1992;207:327–333. [DOI] [PubMed] [Google Scholar]
- 21.Perrelli G, Piolatto G. Tentative reference values for gold, silver and platinum: literature data analysis. Sci Total Environ 1992;120:93–96. [DOI] [PubMed] [Google Scholar]
- 22.Pendegrass CJ, Goodship AE, Price JS, Blunn GW. Nature’s answer to breaching the skin barrier: an innovative development for amputees. J Anat 2006;209:59–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Gordon DJ, Bhagawati DD, Pendegrass CJ, Middleton CA, Blunn GW. Modification of titanium alloy surfaces for percutaneous implants by covalently attaching laminin. J Biomed Mater Res A 2010;94:586–593. [DOI] [PubMed] [Google Scholar]
- 24.LaBerge M, Bobyn JD, Rivard CH, Drouin G, Duval P. Study of soft tissue ingrowth into canine porous coated femoral implants designed for osteosarcomas management. J Biomed Mater Res 1990;24:959–971. [DOI] [PubMed] [Google Scholar]
- 25.Hacking SA, Bobyn JD, Toh K, Tanzer M, Krygier JJ. Fibrous tissue ingrowth and attachment to porous tantalum. J Biomed Mater Res 2000;52:631–638. [DOI] [PubMed] [Google Scholar]
- 26.Bobyn JD, Wilson GJ, MacGregor DC, Pilliar RM, Weatherly GC. Effect of pore size on the peel strength of attachment of fibrous tissue to porous-surfaced implants. J Biomed Mater Res 1982;16:571–584. [DOI] [PubMed] [Google Scholar]