

Abstract
Prior research has demonstrated that adolescent delinquency and depression are prospectively related to adult alcohol use and that adolescent religiosity may influence these relationships. However, such associations have not been investigated using person-centered approaches that provide nuanced explorations of these constructs. Using data from the National Longitudinal Study of Adolescent to Adult Health, we examined whether adolescent delinquency and depression differentiated typologies of adult alcohol users and whether these relationships varied across religiosity profiles. Three typologies of self-identified Christian adolescents and 4 types of adult alcohol users were identified via latent profile analysis. Delinquency and depression were related to increased likelihood of membership in heavy drinking or problematic alcohol use profiles, but this relationship was most evident among those likely to be involved in religious practices. These results demonstrate the importance of person-centered approaches in characterizing the influences of internalizing and externalizing behaviors on subsequent patterns of alcohol use.
Keywords: latent profile analysis, alcohol use, adolescence, delinquency, depression, religiosity
Introduction
A recent national survey estimated that 139.7 million individuals over 12 years of age currently drink alcohol, accounting for a substantial portion (43.6%) of the total US population.1 Although most individuals consume alcohol in moderate amounts with no adverse effects, others use alcohol to a problematic degree. Excessive alcohol use has been correlated with 200 other health problems, and deaths involving alcohol use are the fourth leading preventable cause of death in the United States.2,3 In addition, early initiation into alcohol use is related to increased likelihood of heavy drinking and alcohol-related problems.4 As such, identifying behavioral antecedents in adolescence, a developmental period in which alcohol initiation frequently occurs, has particular importance for preventing the development of problematic alcohol use. Research that establishes identifiable behavioral antecedents to alcohol use in adolescence, and in turn distinguishes those most at risk of developing subsequent alcohol-related problems, may lead to preemptive interventions that prevent escalation into problematic drinking.
Pathways to alcohol use
Robust evidence for 2 distinct but related behavioral pathways to alcohol use has emerged within the literature. The first, an externalizing pathway, is characterized by impulsive, antisocial, and/or delinquent behavior and is posited to result from behavioral undercontrol or dysregulation.4,5 Such conduct is presumed to be some of the first behaviorally maladaptive correlates of later substance use. Indeed, previous research demonstrates that childhood and early adolescent externalizing problems are predictive of an earlier initiation into substance use,6 late adolescent alcohol use,7 and alcohol dependence in young adulthood.8 Specifically, delinquent behavior is frequently antecedent to substance use, suggesting that adolescents may typically begin to use alcohol only after previous engagement in delinquent activity; longitudinal studies have further substantiated this temporal ordering.9,10 Thus, previous research suggests not only that delinquency and alcohol use are correlated but also that delinquency is often temporally precedent to alcohol use.
An alternate, internalizing pathway to alcohol use, wherein individuals use alcohol as a purported means of coping with symptoms of negative emotionality and behavioral inhibition, has also been reflected in the literature.11 Prospective analyses point to positive associations between major depressive disorder at age 11 and the initiation and regular use of alcohol by age 14.5 In addition, a cross-lagged panel analysis designed to explore direction of causation suggested that depression at age 12 was positively associated with alcohol use at age 15, but that the reverse did not hold true.12 Moreover, the influence of adolescent internalizing problems on alcohol use appears to persist into adulthood, but with different effects. Evidence from 2 separate large-scale, longitudinal studies report that early adolescent internalizing problems13 and late adolescent depressed affect14 were negatively related to alcohol use throughout early and mid-adulthood. It would seem that while early internalizing symptoms are generally associated with increased risk of alcohol use within adolescence, they are conversely somewhat protective of the same alcohol-related behaviors in adulthood. These findings highlight the complex role of internalizing symptoms in the development of alcohol use.
Although both pathways have been linked to alcohol use separately, it is unlikely that either pathway operates in isolation. Rather, internalizing and externalizing problems are dynamic and tend to co-occur,15–19 evidenced by frequent comorbidity of conduct disorder and depression in adolescents.20,21 In addition, the emergence of both internalizing and externalizing problems predates adolescent alcohol use.22,23 In instances when internalizing and externalizing problems co-occur, the specific interplay between these behaviors may differentially affect the likelihood of alcohol use. For example, one study found that while the presence of both internalizing and externalizing problems was predictive of later adolescent alcohol use, this relationship was not as strong as the relationship between displaying only externalizing problems and later alcohol use.24 It appears that in this case, internalizing problems may interact with externalizing problems in such a way that this conditional association selectively functions as a protective factor against alcohol use. Such findings demonstrate that these constructs operate in synchrony and that an individual’s pathway to alcohol use may vary as a function of both internalizing and externalizing problems.17,24
Heterogeneity of alcohol use
Just as the various pathways leading to alcohol use are not homogeneous, patterns of alcohol use behaviors (eg, frequencies and quantities of consumption, and frequencies of binge drinking or intoxication) are more complex than a dichotomy of problematic or nonproblematic use. To capture these nuances, researchers have used person-centered approaches to identify typologies of alcohol users. Person-centered approaches, including cluster analysis and latent class analysis, among others, identify homogeneous subgroups of individuals who share similar characteristics within a heterogeneous population; in turn, we can assess whether and how different subgroups are qualitatively different from other subgroups.25,26
Person-centered approaches have been used to identify subgroups of individuals with similar patterns of alcohol use behaviors.27–30 In their recent study, Donovan and Chung28 used latent profile analysis (LPA) to identify 4 prototypical response patterns across a set of alcohol use indicators, which they conventionally referred to as the abstainers, low-intake drinkers, nonproblem drinkers, and problem drinkers. Given such heterogeneity in patterns of alcohol use, as well as the complex interplay among behavioral antecedents associated with increased alcohol use, it is of interest to identify additional behavioral antecedents that may be related to greater odds of nonproblem drinking or abstinence, remembering that such antecedents may be equally nuanced.
Religiosity as a protective factor
Previous research has identified contextual factors correlated with lower levels of alcohol use, as well as decreased prevalence of delinquency and depression. Religiosity is one such factor that is generally considered to serve a protective function with respect to alcohol use and its developmental correlates31–35 and for which small but significant negative associations with delinquency,36–40 depressive symptoms,41–44 and alcohol use45–47 have been identified via cross-sectional and prospective analyses. Most studies have used single item or composite measures as indicators of one’s religiousness, typically reflecting one’s frequency of religious service attendance, or how important religion is to an individual. Even though these studies have attempted to examine associations with various aspects of religiosity, the analyses have primarily been variable centered. However, several recent studies have sought to examine typologies of individuals with qualitatively distinct patterns of responding to religiosity-focused indicators.48–51 Results of these studies suggest the presence of between 3 and 5 prototypical latent religiosity groups during adolescence; the discrepancies in the number of religiosity profiles identified across these analyses may be the result of considerable heterogeneity in the religiosity indicators used in each analysis. Further investigation into latent typologies of religious individuals based on commonly used indicators of religiosity is needed to elucidate the number and specific characteristics of adolescent religiosity typologies.
In addition, some research has invoked variable-centered approaches to explore the ways in which members of religiosity profiles differ in terms of delinquency, depression, and alcohol use. For example, Salas-Wright et al51 found that adolescents who were members of latent profiles with high levels of both public and private religiosity had the lowest levels of alcohol use and delinquency. In addition, Park et al49 identified 4 groups of religious/spiritual individuals; interestingly, those most likely to be members of the highly religious and minimally religious profiles had the lowest levels of depressive symptoms. However, the associations with religiosity examined in each of these studies were exclusively cross-sectional, thereby precluding any examination of developmentally informative associations between typologies of religiosity and behavioral correlates. We expanded on this limitation in this study by examining cross-temporal associations among patterns of religiosity, behavioral antecedents, and subsequent patterns of alcohol use.
The present study
In this study, we provided a number of contributions to the literature on these processes. First, we examined typologies of both religiosity and alcohol use to uncover nuances across homogeneous subgroups of self-identified Christian adolescents and adult alcohol users. Next, we explored relationships between adolescent delinquency/depressive symptoms and adulthood alcohol use typology in response to a void of longitudinal examinations of behavioral antecedents to patterns of alcohol use. Finally, these relationships were further examined within the context of latent profiles of religiosity to determine the extent to which the associations between delinquency, depression, and alcohol use varied across discrete patterns of religiosity. Given that there is variation in the characteristics of typologies of both religiosity and alcohol use in the literature,27–29,49–51 and that it would be difficult to make predictions about the relationships among all nuances within typologies of these constructs, all analyses were considered exploratory.
Methods
Sample
The National Longitudinal Study of Adolescent to Adult Health (Add Health) is a nationally representative survey of American adolescents, providing data on a wide range of health behaviors, attitudes, and environmental factors, including demographics, family relationships, sexual behavior, deviance, and substance use.52 The first wave of data collection consisted of in-school surveys of more than 90 000 US students in 7th to 12th grades during the 1994-1995 school year. Approximately 12 000 of these students were randomly selected to participate in detailed in-home interviews. These adolescents were followed up at wave 2 (1996, approximately ages 12-20), wave 3 (2001-2002, approximately ages 18-26), and wave 4 (2008-2009, approximately ages 24-32). For detailed sampling information, see Harris et al.52
The data from a portion of the in-home sample were de-identified and made available for public use. We reduced this sample to consist only of white, African American, or Hispanic individuals who self-reported Catholic or Protestant religious affiliation and had no missing responses to any of the 5 religiosity items at waves 1 and 2. We also restricted the sample to individuals who had complete responses to alcohol use items at wave 4. These restrictions were put into place to use the maximal amount of complete data, as religiosity items were not assessed among those who did not report a religious affiliation. The final sample consisted of 2610 individuals (55.5% female). These adolescents had a mean age of 15.57 years at wave 1 and consisted of 63.2% white, 24.4% African American, and 12.5% Hispanic individuals. Nearly three-fourths (73.1%) of the sample identified as Protestant at wave 1. The sample had a moderate average adulthood alcohol intake (measured at wave 4), drinking approximately 60 days per year (just more than once per week), consuming an average of 2.75 drinks per occasion.
Measures
Demographics
All demographic data reflect adolescent responses at wave 1. Sex was dummy coded (female = 1). Age was calculated by subtracting participants’ date of birth from the date of their in-home interview. Effect coding was used to derive 2 indicators of race, with whites serving as the reference group in comparison with both African Americans and Hispanics.
Delinquency
Nonviolent delinquent behavior was assessed via 5 items in the wave 1 in-home interview, reflecting the frequency of engagement in these behaviors within the previous 12 months (see Table 1 for item wording). These items were selected from a study by Kuhl et al.53 Individuals responded on a scale where 0 = “never,” 1 = “1 or 2 times,” 2 = “3 or 4 times,” and 3 = “5 or more times” (α = .63).
Table 1.
Specific items used for delinquency and depression at wave 1.
| Delinquency (W1) | Depression (W1) |
|---|---|
| Deliberately damage property that did not belong to you Steal something worth more than $50 Steal something worth less than $50 Go into a house or building to steal something Sell marijuana or other drugs |
You were bothered by things that did not usually bother you You felt that you could not shake off the blues You felt that you were just as good as other peoplea You had trouble keeping your mind on what you were doing You felt depressed You felt that you were too tired to do things You enjoyed lifea You felt sad You felt that people disliked you |
All delinquency items were on a scale of 0 = “never,” 1 = “1 or 2 times,” 2 = “3 or 4 times,” and 3 = “5 or more times.” All depression items were on a scale of 0 = “never or rarely” to 3 = “most or all of the time.”
The item was reverse scored.
Depression
Depressive symptoms were assessed via the Center for Epidemiologic Studies Depression Scale (CES-D).54 Nine items from this scale were selected for analysis, as Jacobson and Newman55 demonstrated that a reduced number of items in the CES-D reflect a unidimensional depression construct. Participants were asked how often a number of statements were true of them during the past week (on a scale from 0 = “never or rarely” to 3 = “most or all of the time,” α = .78) (see Table 1 for specific item wordings). Items were recoded, so higher values represented more frequent presence of depressive symptoms.
Religiosity
Religiosity was assessed from items in the wave 2 questionnaire. Items consisted of frequency of religious service attendance and frequency of attendance at other religiously affiliated activities, such as youth group or choir (both on a scale from 1 = “once a week or more” to 4 = “never”), frequency of personal prayer (1 = “at least once a day” to 5 = “never”), belief in the inerrancy of scripture (1 = “agree” or 2 = “disagree”), and importance of religion in one’s life (1 = “very important” to 4 = “not important at all”). All items were recoded, so higher response values indicated more frequent practice or stronger belief. Coefficient alpha for these items indicated good internal consistency (α = .70). In addition, a single item asked about respondent’s religious affiliation and was dichotomously coded into Catholic = 0 and Protestant = 1.
Alcohol use
Items to assess adulthood alcohol use were taken from the wave 4 questionnaire and were identical to those used in a study by Donovan and Chung.28 The first item asked whether the participant had ever had a drink of alcohol more than 2 or 3 times, to which respondents could answer “yes” or “no.” Three separate items measured the number of days in the past year on which the respondent (1) drank alcohol, (2) drank 5 or more drinks in a row, and (3) was drunk or very high on alcohol. Response categories consisted of 0 = “none,” 1 = “1 or 2 days,” 2 = “once a month or less,” 3 = “2 or 3 days a month,” 4 = “1 or 2 days a week,” 5 = “3 to 5 days a week,” and 6 = “every day or almost every day.” One item asked about the quantity of alcohol consumed per drinking occasion, to which participants responded with a number from 1 to 18.
Alcohol-related consequences were also assessed at wave 4. Four items asked about the frequency of experiencing consequences, and each item was responded to on a 3-point scale, where 0 = “never,” 1 = “1 time,” and 2 = “more than 1 time.” These 4 items covered the frequency with which consuming alcohol (1) disrupted responsibilities in school or the workplace, (2) led to situations that may have put oneself or others at risk, (3) led to legal problems or arrest, and (4) led to relationship problems with family, friends, or colleagues. Coefficient alpha across all items was .62.
A composite measure of adolescent alcohol use was created by multiplying the quantity of alcohol consumed by frequency of alcohol use at wave 1. This was used as a control variable in all analyses predicting wave 4 alcohol use, as quantity by frequency indices of alcohol use is one of the easiest ways to assess total volume of alcohol consumption and is commonly used in alcohol research.56
Analytic plan
A number of steps were taken to reduce the data before the final models were constructed. All analyses were conducted in Mplus version 7.2.57 First, factor scores of delinquency and depression were extracted via confirmatory factor analysis (CFA). We also performed exploratory factor analyses (EFAs) to substantiate the unidimensionality of both constructs; this was done to ensure that the items used to extract factor scores via CFA were definitively representative of a single latent construct within the sample of interest.
Next, LPAs were conducted with respect to wave 2 religiosity and wave 4 alcohol use indicators. LPA is a person-centered analytic technique that examines response patterns across a set of items, classifying cases based on the likelihood of sharing discrete homogeneous patterns of responses.58 In doing so, LPA tests a series of models comparing k profiles with k − 1 profiles (eg, a 2-profile model compared with a 1-profile model), proceeding until the extraction of an additional profile (ie, 3 versus 2 profiles and 4 versus 3 profiles) results in a significant decrement in model fit. Importantly, each model yields posterior probabilities of membership for every individual with respect to each of the k prototypical item response patterns (ie, profiles), such that the sum of those probabilities equals 1.
In the absence of a criterion standard for determining the best number of profiles in LPA, model selection was based on several criteria. Bayesian information criterion (BIC) is an indicator of model fit where decreased values across successive models suggest improved fit.59 Because BIC may continue to decrease across successive models in large samples, additional fit measures were also considered. Entropy measures the amount of organization or accuracy in determining profile membership on a scale from 0 to 1, with increasing values indicating better classification of profile membership.60 The theoretical fit of the model, number of individuals in resulting profiles, and significance levels (P-values) from the Vuong-Lo-Mendell-Rubin Likelihood Ratio test were also considered.61,62 For a complete list of considerations in identifying appropriate profile structure in LPA, see Nylund et al.59
After the best fitting models were selected, we assessed main effects via multinomial logistic regression, wherein the latent categorical variable representing alcohol use response patterns was regressed on delinquency, depression, and a delinquency by depression interaction term. Demographic covariates of age, race, and sex, in addition to covariates of wave 1 alcohol use and Catholic/Protestant identification, were included in these and all subsequent models. We ran comparable models with multiple reference profiles to obtain odds ratios (OR) of all pairwise comparisons among the alcohol use profiles. Although logistic regression is most commonly carried out using a single reference profile, having multiple reference profiles allowed us to understand the likelihood of demonstrating any one pattern of alcohol use in comparison with any other pattern of alcohol use; using a single reference profile would limit our ability to examine the relative risk of developing a particular pattern of alcohol use in relation to other patterns. Next, we examined these same effects among those who were most likely to be members of each religiosity profile. These conditional effects were accounted for by separate model specifications for each religiosity latent profile; that is, the multinomial logistic regression of the latent categorical variable representing alcohol use on depression and delinquency was conditioned on the profile-specific parameters of each religiosity latent profile.57,63
Results
Data reduction
Delinquency and depression factors
Exploratory factor analyses confirmed unidimensional delinquency and depression constructs. Factor loadings for the 5 delinquency items ranged from 0.65 to 0.87, and factor loadings for the 9 depression items ranged from 0.39 to 0.89. Eigenvalues for the delinquency items supported a 1-factor model with an eigenvalue of 3.38 accounting for 67.6% of the variance, and the depression items similarly loaded onto a single factor; the eigenvalue for the 1-factor model was 4.28 and accounted for 47.5% of the variance.
Alcohol use model selection and identification
Prior to inclusion in LPA, the wave 4 alcohol use items were recoded in accordance with thresholds previously determined to be empirically significant in the Add Health sample at wave 1.28 Whether an individual had ever had a drink was dichotomously recoded (0 = “No” and 1 = “Yes”). The items capturing drinking frequency, frequency of getting drunk, and frequency of binge drinking were recoded into 3 response categories (0 = “None,” 1 = “Once/year to 2-3 days/month,” and 2 = “Once/week plus”). The item measuring the average consumption during a single drinking episode was recoded into 4 response categories (0 = “None,” 1 = “1 drink,” 2 = “2-6 drinks,” and 3 = “7 + drinks”). Finally, the sum of negative consequences was dichotomously recoded (0 = “0-2 consequences” and 1 = “3 + consequences”).
Model selection criteria for 2-profile LPA model through 5-profile LPA model can be found in Table 2. All fit indices (except for entropy, which did not substantially change) consistently improved across the 2-profile LPA model through 5-profile model. However, the 4-profile model was selected over the 5-profile model, as the 5-profile model produced one profile containing 34 individuals (0.01% of the sample), which was insufficient to draw any meaningful comparisons. (We did not include respondents who reported having no religion in any of the analyses. However, a separate LPA of wave 4 alcohol use items did demonstrate that a 4-profile model also fits best among these individuals, suggesting that these results are robust to the exclusion of nonreligious respondents. The result of this analysis is available from the authors upon request.) Average alcohol use characteristics of the resulting 4 response patterns are graphically depicted in Figure 1, and Table 3 provides the same characteristics in their original units. We adopted the profile names provided by Donovan and Chung28 to facilitate comparison between our analyses.
Table 2.
Model selection criteria for latent profile analysis of wave 4 alcohol use variables.
| Number of profiles |
||||
|---|---|---|---|---|
| 2 | 3 | 4 | 5 | |
| BIC | 26 325.62 | 23 980.23 | 23 027.89 | 23 041.55 |
| Entropy | 1.00 | 0.89 | 0.91 | 0.89 |
| P-value (k versus k − 1) | .00 | .00 | .00 | .00 |
Abbreviation: BIC, Bayesian information criterion.
P-values are derived from Vuong-Lo-Mendell-Rubin Likelihood Ratio Test. Boldface type denotes criterion values for selected model.
Figure 1.

Average standardized responses to wave 4 alcohol use items by hard-coded membership in alcohol use latent profiles.
Table 3.
Characteristics of wave 4 alcohol use profiles in original units.
| Alcohol use profiles |
||||
|---|---|---|---|---|
| Abstainers | Low-intake | Nonproblem | Problem | |
| Days drink | 0.00 | 25.77 | 85.20 | 203.93 |
| Drinks | 0.00 | 2.47 | 3.87 | 6.33 |
| Days 5 + drinks | 0.00 | 1.03 | 13.75 | 153.63 |
| Days drunk | 0.00 | 0.70 | 10.47 | 103.94 |
| Consequences | 0.23 | 0.35 | 1.62 | 2.72 |
Days drink = number of days per year participants drink alcohol; Drinks = number of drinks per drinking occasion; Days 5 + drinks = number of days per year participants drank 5 or more drinks in a single drinking occasion; Days drunk = number of days per year participants became intoxicated or were very high on alcohol; Consequences = sum of alcohol-related consequences (range from 0 to 8).
The profile that best characterized the largest portion of the sample (N = 894, 34.3%) yielded mean item responses that were consistently 0.5 SD above the sample means. This response pattern was referred to as the nonproblem drinkers. Individuals most likely to demonstrate this pattern on average consumed nearly 4 drinks per drinking occasion and drank just more than 85 days per year (approximately 25% of days per year). In addition, they reported being intoxicated 10 days per year and engaging in binge drinking nearly 14 days per year on average, but reported experiencing 1 to 2 alcohol-related consequences in their lifetime.
A second response pattern was representative of 26.9% of the sample (N = 705) and was named the abstainers. This profile was characterized by those who rarely or never drank alcohol, as demonstrated by average reports of both quantity and frequency of alcohol use nearly 2 full SDs below those most likely to be members of the nonproblem drinkers. On average, individuals most likely to be members of the abstainers reported no instances of binge drinking or intoxication, nearly 1 SD below the sample mean.
The next response pattern was representative of a similar proportion of the sample (N = 696, 26.6%). This profile was referred to as the low-intake drinkers and was characterized by individuals who, on average, reported comparatively modest quantities (2.5 drinks) and frequencies (26 days per year) of alcohol consumption, both of which were 1.5 SDs above those most likely to be members of the abstainers. In contrast, these individuals were similar to members of the abstainers profile with respect to average levels of binge drinking, intoxication, and alcohol-related consequences.
The final profile was representative of the smallest proportion of the sample (N = 317, 12.1%) and was characterized by holding the highest mean frequencies across all alcohol use items. Compared with those most likely to be members of the nonproblem drinkers, individuals most likely to display this response pattern (named problem drinkers) were on average 1.5 SDs higher on binge drinking frequency (154 days per year), a full standard deviation higher on frequency of intoxication (104 days per year), and nearly 0.5 SD higher on number of alcohol-related consequences (2.72).
Religiosity latent profile model selection and identification
We explored models for 2 through 4 profiles of religiosity items. As seen in Table 4, BIC values continually decreased across the 2-profile model to 4-profile model, but the 4-profile model exhibited a significant decrement in model fit (P = .66). Thus, the 3-profile model was selected. To facilitate comparison among the profiles, mean item responses among individuals most likely to be members of each religiosity profile based on their highest posterior probability of membership are graphically depicted in Figure 2. In addition, the proportions of item response endorsements among those most likely to be members of each profile are available in Table 5.
Table 4.
Model selection criteria for latent profile analyses on wave 2 religiosity variables.
| Number of profiles |
|||
|---|---|---|---|
| 2 | 3 | 4 | |
| BIC | 33 448.94 | 33 124.07 | 33 012.90 |
| Entropy | 0.74 | 0.69 | 0.66 |
| P-value (k versus k − 1) | .00 | .00 | .66 |
Abbreviation: BIC, Bayesian information criteria.
P-values are derived from Vuong-Lo-Mendell-Rubin Likelihood Ratio Test. Boldface type denotes criterion values for selected model.
Figure 2.

Average standardized responses to wave 2 religion items by hard-coded membership in religiosity latent profiles.
Table 5.
Items measuring religiosity for wave 2 latent profile analysis.
| Item | M (SD) | Response | Loyal | Reserved | Apathetic |
|---|---|---|---|---|---|
| Frequency of religious service attendance | 3.10 (1.02) | ||||
| 1 | 0.3 | 3.1 | 61.4 | ||
| 2 | 0.4 | 39.1 | 33.0 | ||
| 3 | 16.6 | 37.0 | 3.5 | ||
| 4 | 82.7 | 20.5 | 1.8 | ||
| Frequency of attendance at other religiously affiliated activities, such as youth group or choir | 2.31 (1.24) | ||||
| 1 | 13.9 | 55.0 | 93.6 | ||
| 2 | 9.6 | 26.8 | 2.9 | ||
| 3 | 25.9 | 14.0 | 1.5 | ||
| 4 | 50.5 | 4.2 | 1.8 | ||
| Frequency of personal prayer | 4.01 (1.26) | ||||
| 1 | 0.3 | 3.1 | 44.7 | ||
| 2 | 1.1 | 13.1 | 26.9 | ||
| 3 | 1.3 | 19.0 | 6.4 | ||
| 4 | 22.6 | 36.6 | 5.8 | ||
| 5 | 74.7 | 28.1 | 16.1 | ||
| Belief in the inerrancy of scripture | 1.81 (0.39) | ||||
| 1 | 5.9 | 24.5 | 46.8 | ||
| 2 | 92.3 | 71.4 | 44.7 | ||
| Importance of religion in one’s life | 3.48 (0.62) | ||||
| 1 | 0 | 0 | 0 | ||
| 2 | 0.2 | 6.1 | 35.1 | ||
| 3 | 14.1 | 73.2 | 28.7 | ||
| 4 | 85.8 | 20.7 | 36.0 |
Frequency of religious service attendance and frequency of attendance at other religiously affiliated activities are on a scale from 1 = “never” to 4 = “once a week or more.” Frequency of personal prayer is on a scale of 1 = “never” to 5 = “once a day or more.” Belief in the inerrancy of scripture is on a scale of 1 = “disagree” or 2 = “agree.” Importance of religion is on a scale of 1 = “not important at all” to 4 = “very important.” Columns with religiosity profile names represent the proportion of individuals most likely to be members of that profile endorsing each item response.
The most representative profile accounted for 49.0% of the sample (N = 1279) and was characterized by the highest mean levels of religiosity. This profile was conventionally referred to as the loyal. On average, members of this profile prayed and attended religious services and activities more frequently than members of any other profile, demonstrating item frequencies consistently 0.5 SD above the sample mean.
The next most representative profile accounted for 37.9% of the sample (N = 989) and demonstrated at or slightly below mean levels of religiosity. Specifically, individuals most likely to display this response pattern (referred to as the reserved) were a full standard deviation below likely members of the loyal group with respect to both the importance of religiosity and attendance at religious activities. However, those most likely to be members of the reserved were on average less than 0.5 SD below those most likely to be members of the loyal regarding belief in the inerrancy of scripture.
The final profile was representative of the smallest proportion of the sample (N = 342, 13.1%) and was referred to as the apathetic. The defining characteristics of this response pattern were mean frequencies of attendance at religious services and prayers that were 2 full SDs below the means for those most likely to be members of the loyal. Interestingly, those most likely to be members of the apathetic profile were similar to members of the reserved regarding importance of religion, but were on average at least 0.5 SD lower than members of the reserved on all other items.
Prediction of alcohol use profiles
First, the predictive effects of delinquency and depression on alcohol use profiles were examined. Table 6 provides the ORs related to likelihood of membership in the alcohol use profiles as predicted by delinquency and depression separately, as well as the interaction between them. Delinquency differentiated between likelihood of membership in nearly all comparisons between adult alcohol use profiles. Specifically, each increase of 1 SD in delinquency was associated with more than a 2-fold increase in the likelihood of membership in the problem drinkers group relative to both the abstainers (OR = 2.14, P < .01) and the low-intake drinkers (OR = 2.35, P < .01). Odds of membership in the nonproblem drinkers group evidenced similar, though somewhat more modest increases per unit change in delinquency relative to the abstainers (OR = 1.76, P < .01) and the low-intake drinkers (OR = 1.94, P < .01). Adolescent delinquency did not, however, significantly differentiate membership in the problem drinkers versus nonproblem drinkers, or in the abstainers versus low-intake drinkers.
Table 6.
ORs for membership in alcohol use profiles conditioned on religiosity latent profile memberships, predicted by delinquency and depression.
| Predictor | Condition | Abstainers reference |
Low-intake reference |
Nonproblem reference |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Problem |
Nonproblem |
Low-intake |
Problem |
Nonproblem |
Problem |
||||||||
| OR | P | OR | P | OR | P | OR | P | OR | P | OR | P | ||
| Delinquency | Unconditional | 2.137 | .000 | 1.761 | .000 | 1.103 | .530 | 2.353 | .000 | 1.942 | .000 | 1.212 | .184 |
| Loyal | 8.264 | .002 | 2.674 | .035 | 1.000 | .999 | 8.264 | .002 | 2.882 | .036 | 3.086 | .104 | |
| Reserved | 1.214 | .511 | 1.443 | .146 | 1.170 | .527 | 1.418 | .227 | 1.686 | .043 | 0.841 | .508 | |
| Apathetic | 1.656 | .075 | 1.420 | .186 | 1.239 | .480 | 2.049 | .013 | 1.761 | .043 | 1.164 | .515 | |
| Depression | Unconditional | 1.059 | .681 | 0.782 | .019 | 1.076 | .482 | 1.139 | .361 | 0.532 | .129 | 1.353 | .023 |
| Loyal | 4.831 | .004 | 0.386 | .031 | 1.008 | .974 | 4.878 | .001 | 0.386 | .046 | 12.500 | .000 | |
| Reserved | 0.779 | .418 | 0.980 | .921 | 1.112 | .616 | 0.890 | .679 | 1.091 | .688 | 0.776 | .428 | |
| Apathetic | 0.647 | .074 | 0.484 | .000 | 1.256 | .309 | 0.813 | .415 | 0.608 | .024 | 1.339 | .203 | |
| Del. × dep. | Unconditional | 1.003 | .992 | 0.929 | .779 | 0.843 | .509 | 1.190 | .526 | 1.101 | .712 | 1.081 | .790 |
| Loyal | – | – | 2.410 | .515 | 0.007 | .015 | – | – | 333.333 | .014 | – | – | |
| Reserved | 1.056 | .926 | 0.772 | .627 | 0.519 | .270 | 1.786 | .227 | 1.304 | .567 | 1.370 | .574 | |
| Apathetic | 1.178 | .720 | 1.079 | .869 | 1.772 | .168 | 0.665 | .264 | 0.609 | .208 | 1.092 | .839 | |
Abbreviation: ORs, odds ratios.
Condition refers to the conditions under which the relationship between delinquency/depression and alcohol use was examined. Unconditional models reflect the effect of the predictor on differentiation among alcohol use profiles among all members of the sample. Loyal, Reserved, and Apathetic conditions reflect the effect of the predictor on differentiation among alcohol use profiles, conditioned on the religiosity profile of interest (ie, the effect of delinquency on alcohol use only among those most likely to be members of the loyal religiosity profile). All models control for demographic covariates.
The effects of depression on alcohol use were more obscure. Depression did not appear to differentiate between those most likely to be low-intake drinkers and members of the other 3 profiles, as well as between those most likely to be members of the problem drinkers and the abstainers. Interestingly, however, for every unit increase in depressive symptomatology, individuals were slightly less likely to be members of the nonproblem drinkers in comparison with the abstainers (OR = 0.78, P = .02), but equally more likely to be members of the problem drinkers when compared with the nonproblem drinkers (OR = 1.35, P = .02). The delinquency by depression interaction did not significantly differentiate among likelihood of membership in adult alcohol use profiles.
Religiosity profile–specific prediction of alcohol use profiles
Next, we assessed the extent to which the relationship between delinquency and depression and likelihood of membership in alcohol use profiles differed among those most likely to be members of discrete religiosity profiles (ie, these relationships were conditioned on posterior probabilities of religiosity profile membership). Table 6 also provides ORs and significance levels for associations between delinquency and/or depression and alcohol use profiles when conditioned on membership in each religiosity profile. When conditioned on likelihood of membership in the loyal religiosity profile, each unit increase in delinquency was associated with an increased likelihood of membership in the problem drinkers and nonproblem drinkers relative to both abstainers and low-intake drinkers. For example, given membership in the loyal religiosity profile, individuals were nearly 3 times as likely to be members of the nonproblem drinkers as they were to be low-intake drinkers (OR = 2.88, P = .04). Among those most likely to be members of the reserved religiosity profile, a 1 SD increase in delinquency was associated with an increased likelihood of membership in the nonproblem compared with low-intake drinkers (OR = 1.69, P = .04). Finally, when conditioned on membership in the apathetic religiosity profile, a commensurate increase in delinquency was associated with an increased likelihood of membership in the problem drinkers (OR = 2.05, P = .01) and nonproblem drinkers (OR = 1.76, P = .04) in comparison with the low-intake drinkers.
Increased depression was associated with increased likelihood of membership in the problem drinkers when compared with the abstainers (OR = 4.83, P = .01), low-intake drinkers (OR = 4.87, P = .01), and nonproblem drinkers (OR = 12.50, P < .01), but these relationships were only significant among those who were most likely to be members of the loyal religiosity profile. Among those most likely to be members of the apathetic profile, depression significantly differentiated between likelihood of membership in the nonproblem drinkers compared with the abstainers (OR = .48, P < .001) and in the nonproblem drinkers compared with the low-intake drinkers (OR = .61, P = .02). Depression did not differentiate between any of the alcohol use profiles when conditioned on the reserved religiosity profile.
The delinquency by depression interaction significantly predicted likelihood of membership in alcohol use profile when conditioned on likelihood of membership in the loyal religiosity profile. (Certain ORs were undefined [see Table 6]. This was due to an extremely small cell size when examining relationships between the delinquency by depression interaction predicting likelihood of membership in the problem drinkers when conditioned on likelihood of membership in the loyal religiosity profile [n = 8; see Table 7].) Among those most likely to be members of the loyal profile, the delinquency by depression interaction significantly differentiated among those most likely to be members of the low-intake drinkers compared with the nonproblem drinkers (OR = 333.333, P = .01). This interaction is graphically depicted in Figure 3. Overall, the magnitude of the difference between probabilities of membership in each profile increased as a function of increasing delinquency, that is, individuals were more likely to be a member of the nonproblem drinkers and less likely to be a member of the low-intake drinkers as delinquency increased. However, at low levels of depression, individuals were always more likely to be members of the nonproblem drinkers, whereas at high levels of depression individuals were slightly more likely to be members of the low-intake drinkers when they engaged in low levels of delinquency, but were more likely to be members of the nonproblem drinkers when they had high levels of delinquency.
Table 7.
Numbers of individuals in religiosity-alcohol use profile combinations.
| Alcohol use profile | Religiosity profile |
|||||||
|---|---|---|---|---|---|---|---|---|
| Loyal | Reserved | Apathetic | Total | |||||
| Problem | 8 | 2.5% | 161 | 50.9% | 147 | 46.5% | 316 | 100.0% |
| 1.4% | 13.5% | 17.5% | ||||||
| Nonproblem | 227 | 32.1% | 305 | 43.1% | 176 | 24.9% | 708 | 100.0% |
| 39.1% | 25.6% | 21.0% | ||||||
| Low-intake | 110 | 12.5% | 439 | 49.7% | 334 | 37.8% | 883 | 100.0% |
| 19.0% | 36.9% | 39.8% | ||||||
| Abstainers | 235 | 33.4% | 286 | 40.7% | 182 | 25.9% | 703 | 100.0% |
| 40.5% | 24.0% | 21.7% | ||||||
| Total | 580 | 1191 | 839 | 2610 | ||||
| 100.0% | 100.0% | 100.0% | ||||||
Religiosity profiles were derived from wave 2 responses (Mage = 16.5), whereas alcohol use profiles were derived from wave 4 responses (Mage = 28.5). Percentages to the right of the cell reflect proportion of the religiosity profile in the respective alcohol use profile; percentages below the cell reflect the proportion of the alcohol use profile in that particular religiosity profile. Percentages may be off by 0.1% due to rounding. These ns were taken from the full model; they will not match with the unconditional latent profile analysis models in Figures 2 and 3.
Figure 3.
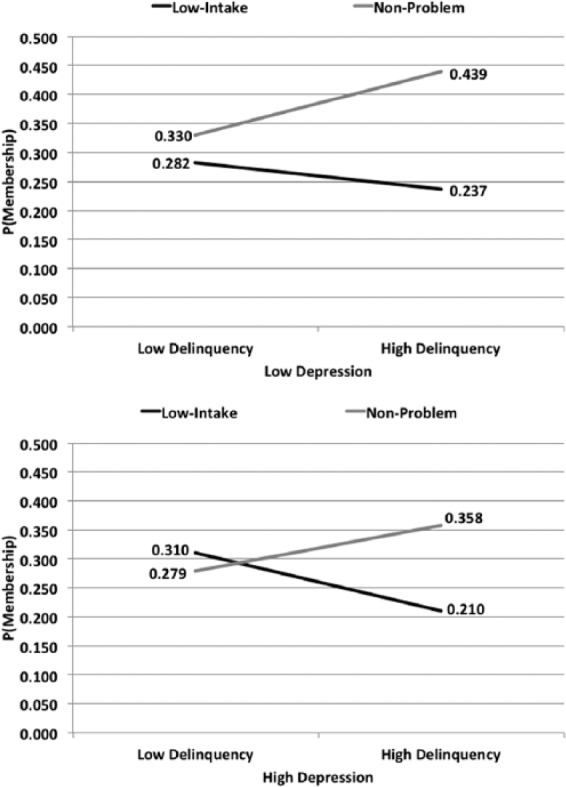
Delinquency by depression interaction in predicting likelihood of membership in the low-intake drinkers compared with the nonproblem drinkers. Figures depict this interaction only among those most likely to be members of the loyal religiosity profile. High/low values of delinquency and depression are based on median splits and are presented for illustrative purposes only.
Also, only among those most likely to be members of the loyal religiosity profile, the delinquency by depression interaction differentiated between those who were more likely to be members of the low-intake drinkers compared with the abstainers (OR = .01, P = .02; see Figure 4). Regardless of depression level, the likelihood of membership in the low-intake drinkers and abstainers decreased with increasing delinquency. However, among those with high levels of depression, individuals were always more likely to be a member of the abstainers, whereas at low levels of depression individuals were more likely to be members of the abstainers when they also engaged in low levels of delinquency, but were more likely to be members of the low-intake drinkers when they engaged in high levels of delinquency.
Figure 4.
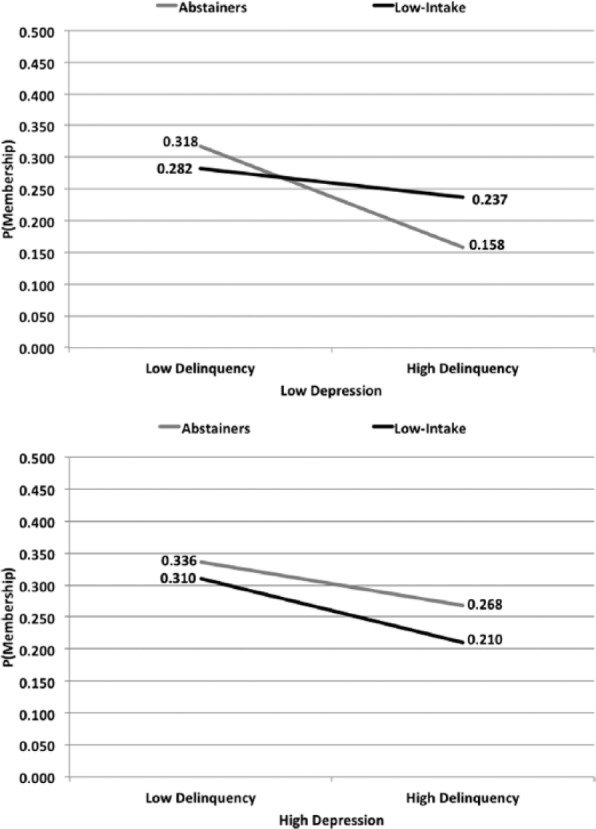
Delinquency by depression interaction in predicting likelihood of membership in the abstainers compared with the low-intake drinkers. Figures depict this interaction only among those most likely to be members of the loyal religiosity profile. High/low values of delinquency and depression are based on median splits and are presented for illustrative purposes only.
Discussion
This examination of behavioral antecedents to adulthood alcohol use suggests that adolescent delinquency and depression may serve to differentiate typologies of alcohol users in adulthood and that the magnitude of these relationships may be associated with one’s likelihood of exhibiting unique patterns of religious behaviors among self-identified Christians.
Delinquency
First, engaging in delinquent activities during adolescence was related to an increased likelihood of heavier drinking in adulthood, irrespective of experiencing alcohol-related consequences (represented by a high likelihood of membership in the nonproblem drinkers and problem drinkers). However, these effects were seen primarily among those who were likely to demonstrate high mean item responses to religiosity-focused indicators. These results support previous literature linking adolescent delinquency to adult alcohol use64; however, these results are indicative of a more nuanced relationship with religiosity than has been expressed in previous literature.33,34,38,48,65,66 For instance, some may suggest that encountering only a few individuals who were likely to be members of both the loyal profile and problem drinkers is indicative of a protective effect of religiosity against the effect of delinquency on the development of problematic drinking patterns (see Table 7). However, we see differential effects of delinquency on likelihood of membership in the problem drinkers across religiosity profiles, demonstrating that delinquency is still a risk factor for development of particular patterns of alcohol use, and the extent of this risk may be associated with particular patterns of religiosity.
There are a number of potential explanations for why such nuanced associations were uncovered in this analysis. First, it may be that those who are “more” religious (in this case, those who identify as Christian and participate frequently in religious services and activities) experience psychologic reactance. Reactance refers to one’s tendency to act in a manner inconsistent with prescribed behavior as retaliation against feeling that one’s autonomy has been challenged.67 Strongly religious individuals may feel that the behavioral mandates set by their religion (such as proscribing the consumption of alcohol) challenge their individual autonomy and drink heavily as a response to this perceived deficit of control. Previous studies have also shown that national crime rates increase as a function of national religiosity68 potentially due to religious individuals’ expectations to receive grace or be forgiven for committing transgressions. It may be that individuals who are highly religious continue to take part in heavy drinking because they expect to be forgiven for such behavior. Another potential explanation is that those most likely to be members of the loyal religiosity profile demonstrate a more “mature” religiosity that permits nonhazardous drinking; future research should seek to substantiate this theoretical possibility.
However, it is most likely that the person-centered approach to examining religiosity in this study may provide a more robust explanation of our findings. Although Benda and Corwyn65 posited that a multidimensional examination of religiosity may reveal complex ways through which religiosity protects against delinquency, previous studies have mainly applied variable-centered approaches, using single item or composite measures of religious service attendance, strength of evangelism (including identity as a born-again Christian), personal religiosity, and religious affiliation or church membership.38,48,65,66 These variable-centered approaches assume that variables relate to each other in the same way across all types of individuals,25,26 leaving the potential for interactions among underlying facets of these variables to remain latent. As such, it may be that the particular pattern of religiosity demonstrated by members of the loyal profile is not most effective in buffering against the influence of delinquent peers. Other studies using person-centered approaches to religiosity have inferred that qualitatively different types of religious individuals engaged in varying levels of delinquent behavior.51 As such, our analysis has replicated this effect and has provided additional evidence that a synthesis of varying levels of religious beliefs and practices (as opposed to indices of low, medium, and high religiosity) could provide additional information about characteristics of diverse individuals that is complementary to that obtained by a variable-centered approach.
Depression
Depression was also predictive of particular types of adulthood alcohol use. Adolescents who experienced more symptoms of depression were (1) less likely to drink heavily and (2) more likely to either abstain from drinking or to demonstrate a problematic pattern of alcohol use. As with delinquency, these relationships varied across religiosity profiles. Given that previous research has found a negative relationship between adolescent depression and adult alcohol use,5,12–14 the finding that depression in adolescence was related to decreased likelihood of membership in low-consuming or abstaining profiles is not surprising. Depressive symptoms, part of a larger category of internalizing symptoms, may be associated with decreased alcohol use in adulthood due to a later initiation into alcohol use. Initiation into alcohol use is strongly tied to social interaction,69 and because adolescents with depressive symptoms may avoid social interaction, they may be less likely to begin drinking, in turn decreasing their risk of developing maladaptive alcohol use patterns. However, that depression was also related to an increased likelihood of problematic drinking patterns, particularly among those who were most likely to demonstrate strong engagement with religious behaviors, is of interest. Although depression has been linked to an increase in problematic drinking, these effects have mainly been found during adolescence.16 Future research must further investigate this association to substantiate the nature of the relationship between depression and alcohol use across time.
The results of this study do not necessarily provide support to the presence of a direct internalizing pathway to alcohol use11 in the context of alcohol use operationalized as a latent categorical variable. Depression differentially predicted likelihood of membership in alcohol use profiles, and this change in operationalization of alcohol use (ie, examining latent profiles of alcohol use rather than indices of frequency/quantity of consumption) demonstrates that depression may be related to lower likelihoods of particular combinations of alcohol use behaviors, rather than indices or alcohol use composite scores used in previous research.70 Given that these results also differ according to the pattern of religiosity one is most likely to exhibit, it may be that the particular pattern exhibited by those most likely to be members of the loyal religiosity profile is particularly protective against the effects of depression on alcohol use.
Depression by delinquency interaction
Examination of the delinquency by depression interaction demonstrated that among those most likely to be members of the loyal religiosity profile, the likelihood of heavy drinking still increased as a function of delinquency, but those who also reported depressive symptoms were less likely to demonstrate heavy drinking patterns than those who did not experience depressive symptoms. These results suggest that delinquency may be a more robust predictor of particular kinds of alcohol use, such that delinquency is inversely related to abstaining or low levels of consumption, but that the extent to which delinquency predicts heavy alcohol use may be dependent on co-occurring depressive symptoms. These findings substantiate those of Colder et al,24 who found that externalizing problems were more effective predictors of later alcohol use when adolescents were only displaying externalizing problems. However, when externalizing problems were coupled with internalizing problems, the relationship between these predictors and alcohol use was weaker. It appears that while delinquency in adolescence indicates that individuals may engage in some kind of alcohol use as an adult, as has been previously demonstrated,5,12 the extent to which this alcohol use will consist of binge drinking and/or intoxication may be dependent on comorbid depression.
Limitations
These findings must be appreciated in light of a number of limitations. First, membership in the loyal profile was related to particularly strong and significant odds of membership in each alcohol use profile when compared with the problem drinkers; however, only 8 individuals were members of both the loyal religiosity profile and the problem drinkers (see Table 7). So, even though comparisons between the problem drinkers and any other alcohol use profile within the loyal profile resulted in extremely large and significant ORs, these results may be different if a larger cell size were available. However, considering that when conditioned on likelihood of membership in the loyal profile increased delinquency was still associated with increased likelihood of membership in the nonproblem drinkers when compared with the abstainers (a comparison with an appropriate cell size, albeit demonstrating a slightly weaker effect), it is likely that the general trend of results is valid, although the true extent of the effect is in need of further replication. As such, we suggest that definitive conclusions about the relationships between the predictors and alcohol use profiles using the problem drinkers as a reference group when conditioned on membership in the loyal religiosity profile should be made only after future work has replicated these results.
As with all secondary data analyses, we were limited to the items available in the Add Health questionnaire. The indicators used in the religiosity LPA assessed a limited number of religious beliefs and behaviors, and the resulting religiosity profiles should be appreciated in light of the specific indicators used. Along these lines, 2 available indicators reflect frequency of attendance at religious services and at religiously affiliated activities. These indicators may be more reflective of parents’ religiosity and church attendance, rather than the adolescent’s autonomous choice to attend services.33,71 Consequently, the profiles may be different if other indicators were included. We encourage future research in this area to examine profiles of religiosity with different combinations of religious beliefs and practices. Given that religiosity indicators were not assessed among those who did not indicate affiliation with an established religious tradition, we are also missing a very specific demographic whose inclusion may have influenced the patterns of religiosity present in the latent profiles. The observed sample appeared to be quite religious, so these religiosity patterns may not be representative of more secular populations. In addition, religiosity was assessed in 1996, and the results may not generalize to adolescents today (see the Pew Research Center72 for an examination of societal changes in religiosity). Finally, entropy in the religiosity LPA was lower than what is typically accepted (see Table 4). This entropy value suggests that we have greater classification error, which may cloud our predictive ability. Because we did not use the results of the religiosity LPA as a predictor or outcome in a 2-stage analysis where classification error is more costly, we accepted the low entropy value in this analysis with the understanding that cases may not be perfectly classified.
Although we were able to assess the effects of adolescent predictors on likelihood of membership in adult alcohol use profiles across those who were likely to demonstrate 3 discrete patterns of religiosity, we were unable to conduct a formal test of moderation effects. Thus, care must be taken to avoid comparing the results of analyses conducted with respect to discrete religiosity profiles and/or between individual religiosity profiles and the full sample (ie, the unconditional model). This is a current limitation of mixture modeling, but suggestive of an area for potential methodologic development. Until such procedures are developed, we are precluded from formally assessing a mechanistic role of religiosity when conceptualized as a latent categorical variable via traditional mediation or moderation. Although our results are suggestive of a mechanistic role of religiosity as a moderator, it will be prudent for methodologists to reassess these results with additional methods. In addition, mixture modeling in general is a probabilistic technique, which means we do not have complete certainty in our religiosity profile assignments and alcohol use classifications. The profiles presented here should be regarded as prototypical item response patterns that have a high likelihood of existing in the population.
An additional limitation is related to our examination of delinquency and depression at baseline, religion 1 year post baseline, and alcohol use outcomes 13 years post baseline. This leaves a large period of time unaccounted for, in which significant events may have occurred but were not captured by data collection. For instance, it may be that some individuals became dependent on alcohol, subsequently went into treatment, and are now represented in the abstainers; these individuals may be qualitatively different from those who have never drank or drink infrequently. Also, the reciprocal effects of delinquency and depression may differentially influence adult alcohol use profiles.73 Parallel process models that track these influences at each time point may provide a more nuanced understanding of how these intertwined factors predict alcohol use.
Other limitations include a reduction in sample from the original, nationally representative Add Health sample. Although such reductions were made to make meaningful comparisons using all available data, this practice reduces the generalizability of our findings. Such reduction in sample may have influenced the examination of the protective effects of religion on delinquency, similar to the ways in which the relationship between delinquency and religion varies depending on the region of the country in which the sample is taken.74 Furthermore, the delinquency items had relatively low internal consistency reliability. Although these items were selected to specifically relate to dimensions of delinquency that have been previously shown to be associated with religiosity and alcohol use,36 future work should expand the dimensions of delinquency assessed to increase the reliability of this measure. In addition, we did not include measures of socioeconomic status in these analyses (eg, total household income and parental level of education) because examining the effects of these factors was beyond the scope of this project, thus limiting our ability to account for additional environmental factors in the development of alcohol use and the initial levels of adolescent delinquency. Finally, we did not account for a number of other variables that have been related to the development of alcohol use, such as social support,31 peer alcohol use,64 and self-regulation.75,76 Future research should include additional auxiliary variables, such as those just mentioned, to understand the complex mechanisms through which these typologies develop across time.
Conclusions
This is the first attempt to examine the role of latent profiles of religiosity in internalizing and/or externalizing pathways to alcohol use patterns. The results of these analyses suggest that delinquency and depression are predictive of alcohol use patterns, but such associations appear to vary among individuals with different patterns of religiosity. Person-centered examinations of religiosity, such as that used in this analysis, are pertinent, considering a societal trend of decreasing affiliation with organized religion.50,72 Even though fewer Americans are identifying with traditional religious denominations, this does not mean that they avoid existential thinking or attendance at religious activities; person-centered approaches will continue to be useful to identify nuances in such patterns of unorganized religious behaviors or beliefs. Future research should continue examining the composition of adolescent religiosity profiles across a wide range of religious and nonreligious individuals, psychosocial correlates of those profiles, and the stability of religiosity patterns over time.
In addition, we were able to replicate the alcohol use profile structure previously identified by Donovan and Chung28 in wave 1 of Add Health using data from the same sample of individuals at wave 4. The persistence of this structure across a span of 13 years suggests that these profiles may remain stable over time. However, we did not assess stability/change in profile membership at the level of the individual (eg, were those most likely to be members of the abstainers at wave 1 still most likely to be members of the abstainers at wave 4?). By identifying such patterns, and factors that may accounting for individual variability in profile membership over time (eg, self-regulation, stressful life events, and treatment seeking), future studies may further inform our understanding of developmentally normative versus atypical drinking processes (eg, are early nonproblem drinkers at increased risk of being subsequent problem drinkers?).
These results highlight the nuanced pathways through which delinquency and depression influence subsequent patterns of alcohol use, demonstrating the importance of examining antecedents to alcohol use within an individual’s unique environmental context. As such, to estimate the extent to which religiosity may function as a protective factor against alcohol use, those working with delinquent or depressed youth must assess an individual’s entire pattern of religiosity-focused practices or behaviors. Further research is also needed to identify whether specific types of externalizing behaviors other than delinquency (eg. antisocial behavior, aggression, and drug use) or specific types of internalizing problems other than depression (eg, social anxiety and excessive withdrawal) are prospectively related to particular patterns of alcohol use so that these specific behavioral antecedents can also be targeted in prevention or intervention efforts.
Footnotes
Peer Review:Five peer reviewers contributed to the peer review report. Reviewers’ reports totaled 2874 words, excluding any confidential comments to the academic editor.
Funding:The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research uses data from Add Health, a program project directed by Kathleen Mullan Harris and designed by J Richard Udry, Peter S Bearman, and Kathleen Mullan Harris at the University of North Carolina at Chapel Hill, and funded by grant P01-HD31921 from the Eunice Kennedy Shriver National Institute of Child Health and Human Development, with cooperative funding from 23 other federal agencies and foundations. Special acknowledgment is due Ronald R Rindfuss and Barbara Entwisle for assistance in the original design. Information on how to obtain the Add Health data files is available on the Add Health website (http://www.cpc.unc.edu/addhealth). No direct support was received from grant P01-HD31921 for this analysis. Preparation of this manuscript was funded in part by a Mentored Research Scientist Development Award K01-AA020333 to Shawn Latendresse from the National Institute on Alcohol Abuse and Alcoholism.
Declaration of conflicting interests:The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Author Contributions: MAH, WCR, and SJL conceived and designed the experiments. MAH and SJL analyzed the data. MAH wrote the first draft of the manuscript. SJL contributed to the writing of the manuscript. MAH, WCR, and SJL agree with manuscript results and conclusions. MAH, WCR, and SJL jointly developed the structure and arguments for the paper. MAH, WCR, and SJL made critical revisions and approved final version. All authors reviewed and approved the final manuscript.
References
- 1. Center for Behavioral Health Statistics and Quality. Behavioral Health Trends in the United States: Results From the 2014 National Survey on Drug Use and Health. 2015. https://www.samhsa.gov/data/sites/default/files/NSDUH-FRR1-2014/NSDUH-FRR1-2014.pdf
- 2. World Health Organization. Global Status Report on Alcohol and Health. Geneva, Switzerland: World Health Organization; 2014. [Google Scholar]
- 3. Stahre M, Roeber J, Kanny D, Brewer RD, Zhang X. Contribution of excessive alcohol consumption to deaths and years of potential life lost in the United States. Prev Chronic Dis. 2014;11:E109. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Zucker RA. Anticipating problem alcohol use developmentally from childhood into middle adulthood: what have we learned? Addiction. 2008;103:100–108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. King SM, Iacono WG, McGue M. Childhood externalizing and internalizing psychopathology in the prediction of early substance use. Addiction. 2004;99:1548–1559. [DOI] [PubMed] [Google Scholar]
- 6. Chassin L, Pitts SC, DeLucia C, Todd M. A longitudinal study of children of alcoholics: predicting young adult substance use disorders, anxiety, and depression. J Abnorm Psychol. 1999;108:106–119. [DOI] [PubMed] [Google Scholar]
- 7. Adalbjarnardottir S, Rafnsson FD. Adolescent antisocial behavior and substance use: longitudinal analyses. Addict Behav. 2002;27:227–240. [DOI] [PubMed] [Google Scholar]
- 8. Guo J, Hawkins JD, Hill KG, Abbott RD. Childhood and adolescent predictors of alcohol abuse and dependence in young adulthood. J Stud Alcohol. 2001;62:754–762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Monahan KC, Rhew IC, Hawkins JD, Brown EC. Adolescent pathways to co-occurring problem behavior: the effects of peer delinquency and peer substance use. J Res Adolesc. 2014;24:630–645. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Wiesner M, Windle M. Young adult substance use and depression as a consequence of delinquency trajectories during middle adolescence. J Res Adolesc. 2006;16:239–264. [Google Scholar]
- 11. Hussong AM, Jones DJ, Stein GL, Baucom DH, Boeding S. An internalizing pathway to alcohol use and disorder. Psychol Addict Behav. 2011;25:390–404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Scholes-Balog KE, Hemphill SA, Patton GC, Toumbourou JW. Relationships between substance use and depressive symptoms: a longitudinal study of Australian adolescents. J Early Adolesc. 2015;35:538–561. [Google Scholar]
- 13. Maggs JL, Patrick ME, Feinstein L. Childhood and adolescent predictors of alcohol use and problems in adolescence and adulthood in the National Child Development Study. Addiction. 2008;103:7–22. [DOI] [PubMed] [Google Scholar]
- 14. Merline A, Jager J, Schulenberg JE. Adolescent risk factors for adult alcohol use and abuse: stability and change of predictive value across early and middle adulthood. Addiction. 2008;103:84–99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Gjone H, Stevenson J. The association between internalizing and externalizing behavior in childhood and early adolescence: genetic of environmental common influences? J Abnorm Child Psychol. 1997;25:277–286. [DOI] [PubMed] [Google Scholar]
- 16. Lilienfeld SO. Comorbidity between and within childhood externalizing and internalizing disorders: reflections and directions. J Abnorm Child Psychol. 2003;31:285–291. [DOI] [PubMed] [Google Scholar]
- 17. Loeber R, Burke JD. Developmental pathways in juvenile externalizing and internalizing problems. J Res Adolesc. 2011;21:34–46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Oland AA, Shaw DS. Pure versus co-occurring externalizing and internalizing symptoms in children: the potential role of socio-developmental milestones. Clin Child Fam Psychol Rev. 2005;8:247–270. [DOI] [PubMed] [Google Scholar]
- 19. Overbeek G, Biesecker G, Kerr M, Stattin H, Meeus W, Engels RCME. Co-occurrence of depressive moods and delinquency in early adolescence: the role of failure expectations, manipulativeness, and social contexts. Int J Behav Dev. 2006;30:433–443. [Google Scholar]
- 20. Loeber R, Keenan K. Interaction between conduct disorder and its comorbid conditions: effects of age and gender. Clin Psychol Rev. 1994;14:497–523. [Google Scholar]
- 21. Wolff JC, Ollendick TH. The comorbidity of conduct problems and depression in childhood and adolescence. Clin Child Fam Psychol Rev. 2006;9:201–220. [DOI] [PubMed] [Google Scholar]
- 22. Kumpulainen K. Psychiatric symptoms and deviance in early adolescence predict heavy alcohol use 3 years later. Addiction. 2000;95:1847–1857. [DOI] [PubMed] [Google Scholar]
- 23. McCarty CA, Wymbs BT, Mason WA, et al. Early adolescent growth in depression and conduct problem symptoms as predictors of later substance use impairment. J Abnorm Child Psychol. 2013;41:1041–1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Colder CR, Scalco M, Trucco EM, et al. Prospective associations of internalizing and externalizing problems and their co-occurrence with early adolescent substance use. J Abnorm Child Psychol. 2012;41:667–677. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Bergman LR, Trost K. The person-oriented versus the variable-oriented approach: are they complementary, opposites, or exploring different worlds? Merrill Palmer Q. 2006;52:601–632. [Google Scholar]
- 26. Laursen B, Hoff E. Person-centered and variable-centered approaches to longitudinal data. Merrill Palmer Q. 2006;52:377–389. [Google Scholar]
- 27. Barnes GM, Welte JW. Patterns and predictors of alcohol use among 7-12th grade students in New York State. J Stud Alcohol. 1986;47:53–62. [DOI] [PubMed] [Google Scholar]
- 28. Donovan JE, Chung T. Progressive elaboration and cross-validation of a latent class typology of adolescent alcohol involvement in a national sample. J Stud Alcohol Drugs. 2015;76:419–429. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29. Windle M. An alcohol involvement typology for adolescents: convergent validity and longitudinal stability. J Stud Alcohol. 1996;57:627–637. [DOI] [PubMed] [Google Scholar]
- 30. Kuvaas NJ, Dvorak RD, Pearson MR, Lamis DA, Sargent EM. Self-regulation and alcohol use involvement: a latent class analysis. Addict Behav. 2014;39:146–152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31. Borders TF, Curran GM, Mattox R, Booth BM. Religiousness among at-risk drinkers: is it prospectively associated with the development or maintenance of an alcohol-use disorder? J Stud Alcohol Drugs. 2010;71:136–142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Koenig HG. Handbook of Religion and Health. 2nd ed. Oxford, England: Oxford University Press; 2012. [Google Scholar]
- 33. Smith C. Theorizing religious effects among American adolescents. J Sci Study Relig. 2003;42:17–30. [Google Scholar]
- 34. Wallace JM, Forman TA. Religion’s role in promoting health and reducing risk among American youth. Health Educ Behav. 1998;25:721–741. [DOI] [PubMed] [Google Scholar]
- 35. Wills TA, Yaeger AM, Sandy JM. Buffering effect of religiosity for adolescent substance use. Psychol Addict Behav. 2003;17:24–31. [DOI] [PubMed] [Google Scholar]
- 36. Benda BB. An examination of a reciprocal relationship between religiosity and different forms of delinquency within a theoretical model. J Res Crime Delinquency. 1997;34:163–186. [Google Scholar]
- 37. Regnerus MD. Linked lives, faith, and behavior: intergenerational religious influence on adolescent delinquency. J Sci Study Relig. 2003;42:189–203. [Google Scholar]
- 38. Regnerus MD. Moral communities and adolescent delinquency: religious contexts and community social control. Sociol Q. 2003;44:523–554. [Google Scholar]
- 39. Wallace LH, Moak SC, Moore NT. Religion as an insulator of delinquency in schools. Am J Crim Justice. 2005;29:217–233. [Google Scholar]
- 40. Laird RD, Marks LD, Marrero MD. Religiosity, self-control, and antisocial behavior: religiosity as a promotive and protective factor. J Appl Dev Psychol. 2011;32:78–85. [Google Scholar]
- 41. Kim-Spoon J, Longo GS, McCullough ME. Adolescents who are less religious than their parents are at risk for externalizing and internalizing symptoms: the mediating role of parent-adolescent relationship quality. J Fam Psychol. 2012;26:636–641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Pearce MJ, Little TD, Perez JE. Religiousness and depressive symptoms among adolescents. J Clin Child Adolesc Psychol. 2003;32:267–276. [DOI] [PubMed] [Google Scholar]
- 43. Schapman AM, Inderbitzen-Nolan HM. The role of religious behaviour in adolescent depressive and anxious symptomatology. J Adolesc. 2002;25:631–643. [DOI] [PubMed] [Google Scholar]
- 44. Wright LS, Frost CJ, Wisecarver SJ. Church attendance, meaningfulness of religion, and depressive symptomatology among adolescents. J Youth Adolesc. 1993;22:559–568. [Google Scholar]
- 45. Chawla N, Larimer ME, Lee CM, Lewis MA, Neighbors C. Attitudes and perceived approval of drinking as mediators of the relationship between the importance of religion and alcohol use. J Stud Alcohol Drugs. 2007;68:410–418. [DOI] [PubMed] [Google Scholar]
- 46. Mason WA, Windle M. A longitudinal study of the effects of religiosity on adolescent alcohol use and alcohol-related problems. J Adolesc Res. 2002;17:346–363. [Google Scholar]
- 47. Nonnemaker JM, McNeely CA, Blum RW; National Longitudinal Study of Adolescent Health. Public and private domains of religiosity and adolescent health risk behaviors: evidence from the National Longitudinal Study of Adolescent Health. Soc Sci Med. 2003;57:2049–2054. [DOI] [PubMed] [Google Scholar]
- 48. Hodge D, Andereck K, Montoya H. The protective influence of spiritual-religious lifestyle profiles on tobacco use, alcohol use, and gambling. Soc Work Res. 2007;31:211–219. [Google Scholar]
- 49. Park NS, Lee BS, Sun F, Klemmack DL, Roff LL, Koenig HG. Typologies of religiousness/spirituality: implications for health and well-being. J Relig Health. 2013;52:828–839. [DOI] [PubMed] [Google Scholar]
- 50. Pearce LD, Foster EM, Hardie JH. A person-centered examination of adolescent religiosity using latent class analysis. J Sci Study Relig. 2013;52:57–79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51. Salas-Wright CP, Vaughn MG, Hodge DR, Perron BE. Religiosity profiles of American youth in relation to substance use, violence, and delinquency. J Youth Adolesc. 2012;41:1560–1575. [DOI] [PubMed] [Google Scholar]
- 52. Harris KM, Halpern CT, Whitsel E, et al. The National Longitudinal Study of Adolescent to Adult Health: research design. http://www.cpc.unc.edu/projects/addhealth/design. Published 2009.
- 53. Kuhl DC, Chavez JM, Swisher RR, Wilczak A. Social class, family formation, and delinquency in early adulthood. Sociol Perspect. 2016;59:345–367. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54. Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. [Google Scholar]
- 55. Jacobson NC, Newman MG. Avoidance mediates the relationship between anxiety and depression over a decade later. J Anxiety Disord. 2014;28:437–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Sobell LC, Sobell Mark B. Alcohol consumption measures. In: Allen JP, Columbus M, eds. Assessing Alcohol Problems: A Guide for Clinicians and Researchers. Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism; 1997:55–73. [Google Scholar]
- 57. Muthén LK, Muthén BO. Mplus User’s Guide. 7th ed. Los Angeles, CA: Muthén & Muthén; 1998. [Google Scholar]
- 58. Arminger G, Clogg CC, Sobel ME, eds. Handbook of Statistical Modeling for the Social and Behavioral Sciences. New York, NY: Plenum Press; 1995. [Google Scholar]
- 59. Nylund KL, Asparouhov T, Muthén BO. Deciding on the number of classes in latent class analysis and growth mixture modeling: a Monte Carlo simulation study. Struct Equ Model Multidiscip J. 2007;14:535–569. [Google Scholar]
- 60. Pastor DA, Barron KE, Miller BJ, Davis SL. A latent profile analysis of college students’ achievement goal orientation. Contemp Educ Psychol. 2007;32:8–47. [Google Scholar]
- 61. Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- 62. Vuong QH. Likelihood ratio tests for model selection and non-nested hypotheses. Econometrica. 1989;57:307–333. [Google Scholar]
- 63. Muthén BO, Asparouhov T. LTA in Mplus: transition probabilities influenced by covariates. Mplus Web Notes No 13. www.statmodel.com. Published 2011.
- 64. Mason WA, Hitchings JE, McMahon RJ, Spoth RL. A test of three alternative hypotheses regarding the effects of early delinquency on adolescent psychosocial functioning and substance involvement. J Abnorm Child Psychol. 2007;35:831–843. [DOI] [PubMed] [Google Scholar]
- 65. Benda BB, Corwyn RF. Religion and delinquency: the relationship after considering family and peer influences. J Sci Study Relig. 1997;36:81–92. [Google Scholar]
- 66. Herrenkohl TI, Hill KG, Chung I-J, Guo J, Abbott RD, Hawkins D. Protective factors against serious violent behavior in adolescence: a prospective study of aggressive children. Soc Work Res. 2003;27:179–191. [Google Scholar]
- 67. Brehm JW. A Theory of Psychological Reactance. Oxford, England: Academic Press; 1966. [Google Scholar]
- 68. Shariff AF, Rhemtulla M. Divergent effects of beliefs in heaven and hell on national crime rates. PLoS ONE. 2012;7:e39048. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69. Hussong AM. The settings of adolescent alcohol and drug use. J Youth Adolesc. 2000;29:107–119. [Google Scholar]
- 70. Mason WA, Hitchings JE, Spoth RL. Emergence of delinquency and depressed mood throughout adolescence as predictors of late adolescent problem substance use. Psychol Addict Behav. 2007;21:13–24. [DOI] [PubMed] [Google Scholar]
- 71. Hirschi T, Stark R. Hellfire and delinquency. Soc Probl. 1969;17:202–213. [Google Scholar]
- 72. Pew Research Center. America’s changing religious landscape. Pew Research Center Religion & Public Life Project. http://www.pewforum.org/2015/05/12/americas-changing-religious-landscape/. Published 2015. Accessed June 25, 2015.
- 73. Kim KJ, Conger RD, Elder GH, Jr, Lorenz FO. Reciprocal influences between stressful life events and adolescent internalizing and externalizing problems. Child Dev. 2003;74:127–143. [DOI] [PubMed] [Google Scholar]
- 74. Stark R. Religion as context: hellfire and delinquency one more time. Sociol Relig. 1996;57:163–173. [Google Scholar]
- 75. Desmond SA, Ulmer JT, Bader CD. Religion, self control, and substance use. Deviant Behav. 2013;34:384–406. [Google Scholar]
- 76. DeWall CN, Pond RS, Carter EC, et al. Explaining the relationship between religiousness and substance use: self-control matters. J Pers Soc Psychol. 2014;107:339–351. [DOI] [PubMed] [Google Scholar]