

Abstract
Background:
Investigating psychological mechanisms that modulate pain, such as those that might be accessed by manipulation of context, is of great interest to researchers seeking to better understand and treat pain. The aim of this study was to better understand the interaction between pain sensitivity, and contexts with inherent emotional and social salience – by exploiting modern immersive virtual reality (VR) technology.
Methods:
A within-subjects, randomised, double-blinded, repeated measures (RM) design was used. In total, 25 healthy participants were exposed to neutral, pleasant, threatening, socially positive and socially negative contexts, using an Oculus Rift DK2. Pressure pain thresholds (PPTs) were recorded in each context, as well as prior to and following the procedure. We also investigated whether trait anxiety and pain catastrophisation interacted with the relationship between the different contexts and pain.
Results:
Pressure pain sensitivity was not modulated by context (p = 0.48). Anxiety and pain catastrophisation were not significantly associated with PPTs, nor did they interact with the relationship between context and PPTs.
Conclusion:
Contrary to our hypothesis, socially and emotionally salient contexts did not influence pain thresholds. In light of other research, we suggest that pain outcomes might only be tenable to manipulation by contextual cues if they specifically manipulate the meaning of the pain-eliciting stimulus, rather than manipulate psychological state generally – as per the current study. Future research might exploit immersive VR technology to better explore the link between noxious stimuli and contexts that directly alter its threat value.
Keywords: Chronic pain, psychological factors, anxiety, pain catastrophising, fear of pain
Introduction
The idea that perception is the linear result of sensory input has long been refuted by human susceptibility to a plethora of illusory phenomena and decades of psychophysical science.1,2 While the principles underlying, for example, the visual perception of objects, depth and colour have been extensively investigated, extrapolation of this kind of perceptual science to the field of pain is in its infancy. Pain is a complex perception subserving bodily protection.3 As such pain is likely to depend not only on noxious input from threatened tissues but the integration of other sensory cues and emotional factors which might alter the interpretation of such sensory data.4 Indeed, evidence confirms that pain is modulated not only by noxious stimuli but also by non-noxious elements – such as mood, meaning, expectations, motivation and attention – that may depend on factors such as past experience, psychological state, expectations and context.5–8
While the relationship between context and pain is not well investigated, research has shed some light. For example, pleasant contexts tend to reduce pain through distraction,9 while hyper-attentiveness towards bodily sensations tends to increase pain.10 Context can also modulate pain by altering the meaning of the stimulus.11,12 For example, when asking subjects to rate the intensity of a noxious stimulus, the perceived intensity of the stimulus can be manipulated by enhancing its perceived threat – through verbal suggestions of potential harm.13,14 However, the influence of threat and other psychological variables which may be manipulated by contextual cues is not necessarily unidirectional. For example, stress-induced analgesia is a phenomenon whereby induction of a threatened state results in a decrease, rather than increase in pain15 in contrast to studies showing that presentation of threatening cues increases pain.16
Studies examining the effects of non-noxious sensory and contextual variables on pain have typically delivered discrete verbal, visual, tactile or auditory cues, and then asked subjects to rate the intensity of concurrent noxious stimulation.16–20 Unfortunately, in these experimental settings, the potential power of these sensory and contextual variables to elucidate interactions between under-studied psychological variables21 and pain may be stifled by the chasm separating real-world scenarios, and the laboratory attempts to mimic them. While virtual reality (VR) has improved exponentially over recent time, its benefit over conventional tools in psychological research has been known for over a decade.22 That is, VR can provide more realistic, credible and immersive stimuli – since the person is perceptually surrounded by the virtual environment, and is embodied within it.22 Thus, there are now exciting opportunities to closely simulate real-world contexts to better understand interactions between visual contextual stimuli and pain.
This study aimed to investigate the differential influences of pleasant, threatening, socially positive and socially negative contexts on pressure pain thresholds (PPTs). We hypothesised that PPTs would be decreased in the threatening and socially negative contexts, and increased in the pleasant and socially positive contexts, relative to neutral contexts. We also aimed to explore whether pain catastrophising and anxiety interacted with the relationship between context and pain threshold. We hypothesised that higher levels of pain catastrophisation and anxiety would reduce pain sensitivity induced by the socially negative and threatening contexts.
Methods
Ethics statement
This study was approved by the institutional research ethics board for human research (Reference number: AHS/23/15/HREC). Written informed consent was obtained from each individual, with participants rights protected and research conducted according to the Declaration of Helsinki.
Participants
Participants were recruited through local university campus advertisements, social media and word of mouth. Participants were excluded if they had an injury within the previous 3 months; a history of chronic pain; psychiatric impairment; impaired neurological, vascular or metabolic function that impaired sensory discrimination; severely impaired vision; high sensitivity to motion sickness; a history of vertigo or epilepsy; or were under 18 or over 65 years old. Participants did not receive any rewards (monetary or otherwise, for example, course credits) for participating.
Based on further pilot data analysis (n = 13), which showed an overall effect size of partial η2 = 0.07, a minimum of 22 participants were required to reveal an effect of condition with 80% power and alpha set to 0.05. In total, 25 participants were recruited to satisfy both power and counterbalancing requirements.
Stimulus material and apparatus
A VR head mounted display (Oculus Rift DK2, California), and headphones were utilised to deliver the contextual stimuli. Participants were seated in an armchair with back and arm support. Mechanical pain thresholds were tested using a 40 kPa/s rate-controlled pressure algometer (Somedic, Sweden) applied over the tibialis anterior muscle.
Scene selection procedure
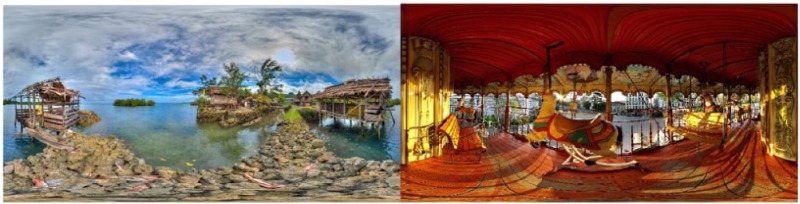
VR contexts were carefully selected to match the five context categories. VR contexts were constructed from 360° photographs. In the first phase of the selection process, the experimenters created a database of virtual scenes in each of the five categories through a process of consensus. In the second phase, four individuals were exposed to each of the scenes in VR, and asked to rate their emotional response to the scenes using the Self-Assessment Manikin (SAM) scale. The SAM scale is a 5-point visual scale divided into the domains of (1) Pleasure, (2) Arousal and (3) Dominance/Control. These data were then used to choose the final two images for each category according to the following criteria: (1) Neutral scenes: rated as most neutral with respect to pleasure and dominance; (2) Pleasurable scenes: rated as most pleasurable; (3) Socially positive scenes: rated as most pleasurable and least dominating; (4) Socially negative scenes: rated as least pleasurable and most dominating; and (5) Threatening scenes: those rated as most dominating. The examiners then performed a consensus process to select sound effects that appropriately augmented the visual contexts. The pleasant, socially positive, socially negative, threatening and neutral contexts are shown in Appendix 1.
Experimental design
A within-subjects, randomised, double-blinded, repeated measures (RM) design was used. Five different orders of scene presentations were determined using a combination of counterbalancing and randomisation, to reduce potential order effects. Specifically, the first and last categories presented were counterbalanced, with the middle categories randomised. It was seen as most important to balance the first and last scenes, since any effect of order would likely exert it main influence there. Each tester was assigned a role for the duration of the study. The tester responsible for testing PPTs was blinded to scene. A second tester, also blinded, recorded and entered the PPT data. A third tester was responsible for delivery of each context, but did not interact with the participant. The participants understood that the experiment related to VR and pain sensitivity, but were blinded to the experimental hypothesis as well as their threshold results after each trial.
Prior to the experiment, a pilot study was performed (n = 6) to determine the algometer operator. The algometer operator with the smallest within-participant PPT variability (6.54%) was selected to perform this task for all participants. Following the last participant, data were de-coded, extracted and analysed by investigators not involved with data collection.
Outcome measure
PPTs were collected by applying the algometer perpendicularly to the skin over the superior third of the tibialis anterior muscle belly. The algometer was re-positioned with an overlap of approximately 50% after each trial to decrease the potential for habituation or sensitisation effects. PPT measures in each context were adjusted relative to measures obtained for the neutral scenes (i.e. PPTContext1 = (PPTContext1 − PPTNeutralContext)/PPTNeutralContext). The order of PPT application (left vs right leg) throughout the experiment was randomised and counterbalanced. The testing protocol is demonstrated in Figure 1.
Figure 1.

Testing protocol with ‘*’ indicating each PPT measure. Four pressure pain thresholds were measured in each context (twice in each scene, one on each leg with 30 s interstimulus interval), and in the pre- and post-experiment period (two on each leg). PPTs were measured in the final 30 s of each scene.
Questionnaires
The Pain Catastrophisation Scale (PCS) and Generalised Anxiety Disorder 7-Item (GAD-7) questionnaires were completed at baseline. The PCS investigates catastrophic thinking about pain.23 It contains 13 statements and responders are asked to rate each statement based on their experience from 0 (not at all) to 4 (all of the time). A score greater or equal to 24 is considered to reflect a clinically significant level of pain catastrophisation,24 with research demonstrating that high levels of pain catastrophising is associated with future chronic low back pain and disability.25 The GAD-7 is used as a screening tool and severity measure for generalised anxiety disorder (GAD).26 The GAD-7 score is calculated by assigning scores of 0, 1, 2 and 3, to the response categories of ‘not at all’, ‘several days’, ‘more than half the days’ and ‘nearly every day’, respectively, and adding scores across the seven questions. Scores of 5, 10 and 15 are taken as the cut-off points for mild, moderate and severe anxiety, respectively. Both questionnaires are reliable upon repeat testing (r > 0.70) and have been validated for use in adult individuals.26–28
Experimental protocol
Informed consent was obtained and questionnaires and demographic forms were completed. The experimental procedure was then explained to each participant using a consistent and predetermined script. It was explained to participants that they were to explore each scene by turning fully to the right and return to the centre, and this would be followed by PPT measurement. Each participant was positioned in the chair with their feet flat on the floor. Two baseline PPTs were recorded for each of the right and left tibialis anterior muscles, and following this, the head mounted display and headphones were applied. Where necessary, participants were reminded to turn their head fully to the right and then return to the image centre. Duration of each scene totalled 60 s. After the last scene, the head mounted display and headphones were removed and post-experiment PPT measurements were taken. As a post-experiment manipulation check, participants were re-exposed to each scene and asked to rate each image on numerical rating scales (NRS), with respect to the following elements: scene immersiveness, arousal, level of fear, feeling of control and emotional valence (Appendix 2).
Data analysis
Raw data were analysed for normality through visual inspection of box and scatter plots. Paired t-tests investigated the difference between left- and right-sided PPTs. As there was no significant difference between sides, the average of the PPTs was calculated and used in further analyses. The effect of ORDER (1–5) on PPTs measured within VR immersion was analysed using one-way analysis of variance (ANOVA). The main effect of CONTEXT (pleasant, socially positive, socially negative and threatening) on PPTs measured within VR immersion, relative to neutral context, was analysed using RM analysis of covariance (ANCOVA), with gender and pain catastrophisation (PCS) or anxiety (GAD-7) entered as a covariate, as a result of their demonstrated relationship with pain thresholds.29–31 Initially, bivariate relationships between PCS and GAD-7 were investigated using Spearman’s rho. As a result of a significant correlation between the two variables (ρ = 0.41, p = 0.042), either PCS or GAD-7 was entered into separate RM ANCOVA models as covariates in conjunction with gender. For this analysis, adjusted PPT measures were utilised (relative to neutral context). As there was no significant difference between contexts, the average of all context PPTs was calculated and used in examining the effect of VR. The effect of VR (pre-, during and post-VR) on PPTs was analysed using one-way RM ANOVA. Assumptions for RM ANOVA were tested, including Mauchly’s Test of Sphericity. When Mauchly’s Test of Sphericity was violated (p < 0.05), Greenhouse-Geisser corrections were applied. Where significant effects of fixed factors were observed, pairwise comparisons using Bonferroni corrections for multiple comparisons were performed to investigate specific between-context differences. One-way ANOVA was used to investigate participant NRS ratings for immersiveness, arousal, level of fear, feeling of control and emotional valence for each category. Results were expressed in terms of statistical significance (p ⩽ 0.05), and effect size as partial eta squared.
Results
Participants
Twenty-five healthy volunteers (14 males, 11 females; mean = 21.3 ± 3.5 years) were recruited. Participants reported mild levels of anxiety (GAD-7 median [interquartile range]: 4 [1.5, 8]) and pain catastrophisation (PCS: 14 [6, 23]). Three individuals reported GAD-7 scores of ⩾10, indicating the presence of moderate anxiety,32 while five individuals reported the presence of clinically meaningful levels of pain catastrophisation (PCS ⩾ 24).24 Females reported higher levels (mean (± standard deviation (SD)); 6.6 (4.8)) of generalised anxiety than males (3.6 (2.6); t23 = 2.1, p = 0.05). There was no significant effect of gender on pain catastrophisation scores (t23 = 0.86, p = 0.40).
Manipulation check: participant ratings of contextual images
There was a significant difference in participants’ rating of the socially negative and threatening images for the ‘fear’ (F(1.9, 45.2) = 27.4, p < 0.00), ‘arousal’ (F(2.1, 51.2) = 25.7, p < 0.00), ‘control’ (F(1.9, 46.4) = 23.5, p < 0.00) and ‘emotional valence’ (F(2.3, 54.9) = 36.5, p < 0.00) NRS scales, when compared to the other contextual images (Table 1). There was no significant difference in participants’ rating of one’s sense of ‘immersiveness’ (F(2.7, 65.1) = 2.55, p = 0.07), among the various contextual images. Post hoc Bonferroni pairwise comparisons demonstrated that the socially negative and threatening images were more controlling (p < 0.00) and emotionally valent (p < 0.00) than the neutral, pleasant and socially positive images. Pleasant and socially positive scenes demonstrated the most positive valence scores, and were not statistically different than the neutral scenes (p > 0.057 for both). The socially negative and threatening images also resulted in higher scores for the ‘fear’ (p < 0.00) and ‘arousal’ (p < 0.00) NRS scales.
Table 1.
Median and interquartile range for the ratings of each scene with respect to immersiveness and psychological properties.
| Statement (scale) | Neutral | Pleasant | Socially positive | Socially negative | Threatening |
|---|---|---|---|---|---|
| Immersiveness (−3 to 3) | 1.5 [0.5, 2] | 1 [−1, 2] | .5 [−1, 1.8] | 0.5 [−0.3, 1.5] | 1 [−1, 2] |
| Fear (0–10) | 0 [0, 0.75] | 0 [0, 0.75] | 0 [0, 0.5] | 3.5 [1, 5]* | 4.5 [2.5, 6.5]* |
| Arousal (0–10) | 0 [0, 1.5] | 0.5 [0, 2] | 1 [0.5, 2.3] | 4.5 [2.8, 5.8]* | 5.5 [3.5, 6.8]* |
| Control (0–10) | 0.5 [0, 1.5] | 0.5 [0, 1.3] | 1.5 [0, 3] | 6 [2.8, 7]* | 5.5 [2.8, 6.5]* |
| Valence (0–10) | 2 [1, 3] | 0.5 [0, 1.8] | 2 [1, 2.5] | 6.5 [5.3, 7]* | 7 [4.5, 7.8]* |
p ⩽ 0.05.
Effect of order during virtual immersion
There was no significant effect of order across the experiment (F(4, 120) = 0.503, p = 0.73, partial η2 = 0.016), indicating that PPTs did not significantly improve or worsen during VR, irrespective of context and supporting the randomisation process that was undertaken.
Primary outcome: effect of context on pain threshold
There was no significant main effect of context (F(3, 66) = 1.00, p = 0.40, partial η2 = 0.04) (Figure 2), indicating that PPTs were not modulated by the chosen VR contexts. There was no significant interaction effect of context × anxiety (F(3, 66) = 1.15, p = 0.36, partial η2 = 0.05), context × pain catastrophisation (F(3, 66) = 0.88, p = 0.46, partial η2 = 0.04) or context × gender (F(3, 66) = 0.98, p = 0.41, partial η2 = 0.04), indicating that gender and psychological variables did not significantly influence PPTs for various contexts. There was also no main effect of gender, anxiety or pain catastrophisation levels on average PPTs: gender (F(1, 22) = 1.37, p = 0.26, partial η2 = 0.059), anxiety (F(1, 22) = 0.30, p = 0.59, partial η2 = 0.013) or pain catastrophisation (F(1, 22) = 0.003, p = 0.96, partial η2 < 0.00).
Figure 2.
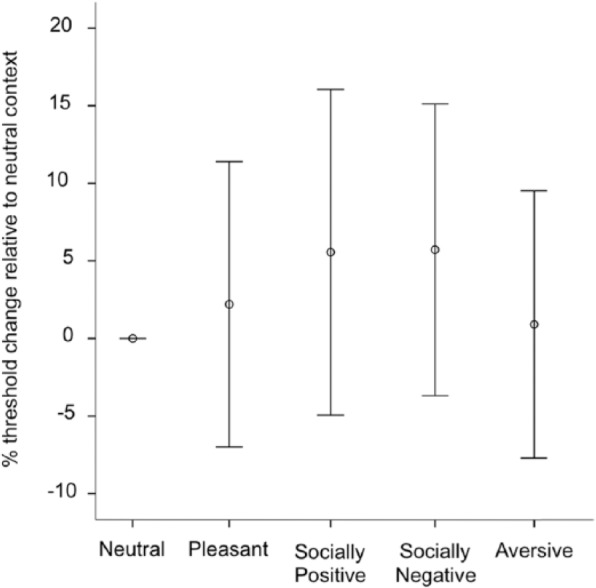
Effect of context on mechanical pain threshold relative to the neutral. Bars indicate 95% confidence intervals. Values above zero indicate relative hypoalgesia, while values below zero indicate relative hyperalgesia to pressure stimuli compared to the neutral scene.
Effect of VR
There was a significant main effect of VR (pre-, during, post-VR) on PPTs (F1.571, 37.696 = 14.8, p = 0.00, partial η2 = 0.38, Figure 3). Post hoc Bonferroni pairwise comparison demonstrated that post-VR PPTs (355 kPa (95% confidence interval (CI): 292, 419)) were lower than pre-VR PPTs (430 kPa (95% CI: 356, 503)); p = 0.005). There were no significant differences demonstrated between pre-VR (p = 0.054) or post-VR (p = 1.00) PPTs with those measured during VR (375 kPa (95% CI: 310, 440)).
Figure 3.

Effect of virtual reality (VR) immersion on median tibialis anterior pressure pain thresholds. Bars indicate interquartile range.
*p < 0.05.
Discussion
This study aimed to investigate the differential influences of pleasant, threatening, socially positive and socially negative contexts on PPTs using immersive VR. We hypothesised that there would be increased pain sensitivity in threatening and socially negative contexts and decreased pain sensitivity in pleasant and socially positive contexts, relative to neutral contexts. We also hypothesised that the influence of context on pain would be augmented by anxiety and pain catastrophising. Our results did not support our hypotheses. That is, PPTs were not differentially influenced by context, and anxiety and pain catastrophising did not interact with the relationship between context and PPT.
Given previous research findings suggesting that perceived threat enhances pain,13,14 the lack of significant finding in this study was surprising. The lack of effect does not appear to be as a result of failure to produce meaningful and varied contexts, since the scene rating data confirmed the successful manipulation effected by each context, evidenced both in the immersiveness ratings (participants largely agreed that each scene was immersive) and the scene ratings for each psychological construct measured, which approached the limits of each scale. There are a number of reasons that may explain our null result. First, in previous studies demonstrating an effect of context, the experimental manipulation directly altered the actual or perceived threat of the painful stimulus. For example, Antz and Claassens13 used visual cues to suggest a noxious thermal stimulus was either hot or cold, despite the fact it was always cold.13 When the cue indicated it was hot, it was perceived as (1) more threatening, (2) more painful and (3) hotter, compared to when the cue suggested it was cold. Similarly, Wiech et al.14 manipulated the context of a laser stimulus using verbal suggestion of danger, by falsely indicating that some stimuli were being delivered to areas where skin was more vulnerable to burn. Stimuli were more likely to be perceived as painful when delivered to the area believed to be more vulnerable. In contrast, although the contexts presented in our study were globally threatening, they were less likely to directly manipulate the threat of the mechanical stimulus (algometer) performed at an individual’s pain threshold level (i.e. was not painful). In fact, prior to the experiment, study participants were assured that the applied stimulus was unlikely to elicit harm. The functional and neurochemical mechanisms underlying the potential effect of context have been reviewed elsewhere,4 and include changes in cortical processing and descending inhibition. When comparing our results to other studies investigating the influence of images on pain, it is evident that our images focussed on emotional and social salience. As a result of recent functional magnetic resonance imaging (fMRI) studies, it is becoming apparent that visualisation of different images activates different brain regions.33–37 These brain regions are dissociable and separately modifiable.38 Thus, our social and emotionally valent images may not have resulted in activation of brain regions or modulate brain processes associated with somatic pain, as would be induced by the algometer.
Since pain catastrophising and anxiety have been shown to modulate a number of the dimensions of pain, including both the intensity and spread of pain (Niederstrasser 2014; Harvie et al unpublished), we also hypothesised that these psychological variables might interact with the effect of context on pain thresholds. These findings were not supported, with anxiety and pain catastrophising showing no interaction with the relationship between context and pain threshold. That is, anxiety or pain catastrophisation scores did not influence PPTs during the socially negative or threatening images. However, given the relatively low levels of pain catastrophisation24 and anxiety26 demonstrated by our participants, further research involving individuals with higher levels would be warranted.
Although not a primary aim of this study, we also demonstrated that increased pain sensitivity was evident following VR, when compared to pre-VR immersion. This is a unique finding and does not appear to be demonstrated or reported in other studies. As a control group was not employed in this study without VR context presentation, the reasons for this are entirely speculative and may relate to progressive increased sensitisation as a result of repeat mechanical measures being performed, despite our efforts to ensure that PPTs were only partially overlapping prior areas of application. As there was no effect of order during VR immersion, and PPTs measured post-VR were not significantly lower than those measured during VR immersion, the ‘clinical’ significance of these findings is unclear. It must also be noted that the difference in pain thresholds measured prior to and following VR immersion (Figure 3: 75 kPa), although statistically significant, may not be detected by all participants, given that they are slightly less than the published minimal detectable change (86 kPa) for tibialis anterior.39 Thus, we can only speculate as to the mechanisms underlying this increased pain sensitivity. This requires replication in future studies, and possible further investigation.
Our study has several limitations that require noting. First, we investigated the role of context on pain sensitivity, and not pain intensity. Various studies have demonstrated that PPTs and clinical pain levels are not necessarily correlated,40,41 and thus, it remains to be seen whether contexts such as those in this study moderate pain intensity. Second, since only 30 s of a scene was presented before PPT measures were recorded, carry-over effects from the previous context to the next cannot be ruled out; however, the order of conditions were altered between participants to eliminate any systematic effects. Longer scene duration may also have resulted in greater immersiveness. Finally, our study investigated young healthy volunteers with low levels of anxiety and pain catastrophisation, and thus, we cannot rule out the possibility that certain trait variables, not present in the current population, relate to a propensity towards sensitisation in certain contexts. Recruiting populations who rate high on measures of somatisation and/or have clinical pain symptoms (e.g. chronic pain patients) would be of particular interest. Future research would also benefit from investigating a range of other contexts, such as those associated with pain which may be more relevant to somatic pain.37
In summary, socially and emotionally salient contexts did not influence pain thresholds. We suggest that pain outcomes might only be tenable to manipulation by contextual cues if they directly manipulate the meaning of the pain-eliciting stimulus, rather than where they manipulate psychological state generally – as per the current study. Future research might exploit immersive VR technology to better explore the link between noxious stimuli and contexts that directly alter its threat value.
Appendix 1
Virtual reality (VR) scenes
-
Threatening.

-
Pleasant.
-
Socially negative.

-
Socially positive.

-
Neutral.

Appendix 2
Scene characteristics questionnaire
-
How much do you agree with this statement?
I feel as if I am really there
−3……….−2……….−1……….0……….1……….2……….3
Strongly Disagree Strongly Agree
-
On a scale of 0–10 with zero ‘being not afraid’ and 10 ‘being the most afraid’, how afraid are you at this moment?
0 1 2 3 4 5 6 7 8 9 10
-
How calm do you feel on the following scale (0 = completely calm, 10 = hyper-alert)?
0 1 2 3 4 5 6 7 8 9 10
-
How in control, or dominated, do you feel right now (0 = completely in control, 10 = completely dominated)?
0 1 2 3 4 5 6 7 8 9 10
-
How pleasant or aversive do you find this scene (0 = highly pleasant, 10 = highly aversive)?
0 1 2 3 4 5 6 7 8 9 10
Footnotes
Conflict of interest: The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding: The author(s) received no financial support for the research, authorship and/or publication of this article.
References
- 1. Goldstein EB. The Blackwell handbook of sensation and perception. New York: John Wiley & Sons, 2008. [Google Scholar]
- 2. Weiten W. Psychology: themes and variations – themes and variations. Boston, MA: Cengage Learning, 2007. [Google Scholar]
- 3. Hochstein S, Ahissar M. View from the top: hierarchies and reverse hierarchies in the visual system. Neuron 2002; 36(5): 791–804. [DOI] [PubMed] [Google Scholar]
- 4. Carlino E, Frisaldi E, Benedetti F. Pain and the context. Nat Rev Rheumatol 2014; 10(6): 348–355. [DOI] [PubMed] [Google Scholar]
- 5. Brooks J, Tracey I. From nociception to pain perception: imaging the spinal and supraspinal pathways. J Anat 2005; 207(1): 19–33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tracey I. Getting the pain you expect: mechanisms of placebo, nocebo and reappraisal effects in humans. Nat Med 2010; 16(11): 1277–1283. [DOI] [PubMed] [Google Scholar]
- 7. Wiech K, Ploner M, Tracey I. Neurocognitive aspects of pain perception. Trends Cogn Sci 2008; 12(8): 306–313. [DOI] [PubMed] [Google Scholar]
- 8. Wiech K, Tracey I. The influence of negative emotions on pain: behavioral effects and neural mechanisms. NeuroImage 2009; 47(3): 987–994. [DOI] [PubMed] [Google Scholar]
- 9. Malloy KM, Milling LS. The effectiveness of virtual reality distraction for pain reduction: a systematic review. Clin Psychol Rev 2010; 30(8): 1011–1018. [DOI] [PubMed] [Google Scholar]
- 10. Crombez G, Eccleston C, Baeyens F, et al. Attention to chronic pain is dependent upon pain-related fear. J Psychosom Res 1999; 47(5): 403–410. [DOI] [PubMed] [Google Scholar]
- 11. Moseley GL. Reconceptualising pain according to modern pain science. Phys Ther Rev 2007; 12(3): 169–178. [Google Scholar]
- 12. Moseley GL, Arntz A. The context of a noxious stimulus affects the pain it evokes. Pain 2007; 133(1–3): 64–71. [DOI] [PubMed] [Google Scholar]
- 13. Arntz A, Claassens L. The meaning of pain influences its experienced intensity. Pain 2004; 109(1–2): 20–25. [DOI] [PubMed] [Google Scholar]
- 14. Wiech K, Lin CS, Brodersen KH, et al. Anterior insula integrates information about salience into perceptual decisions about pain. J Neurosci 2010; 30(48): 16324–16331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Butler RK, Finn DP. Stress-induced analgesia. Prog Neurobiol 2009; 88(3): 184–202. [DOI] [PubMed] [Google Scholar]
- 16. Madden VJ, Harvie DS, Parker R, et al. Can pain or hyperalgesia be a classically conditioned response in humans? A systematic review and meta-analysis. Pain Med 2016; 17(6): 1094–1111. [DOI] [PubMed] [Google Scholar]
- 17. Lamm C, Decety J, Singer T. Meta-analytic evidence for common and distinct neural networks associated with directly experienced pain and empathy for pain. Neuroimage 2011; 54(3): 2492–2502. [DOI] [PubMed] [Google Scholar]
- 18. Morrison I, Downing PE. Organization of felt and seen pain responses in anterior cingulate cortex. Neuroimage 2007; 37(2): 642–651. [DOI] [PubMed] [Google Scholar]
- 19. Morrison I, Peelen MV, Downing PE. The sight of others’ pain modulates motor processing in human cingulate cortex. Cereb Cortex 2007; 17(9): 2214–2222. [DOI] [PubMed] [Google Scholar]
- 20. Cheng Y, Lin CP, Liu HL, et al. Expertise modulates the perception of pain in others. Curr Biol 2007; 17(19): 1708–1713. [DOI] [PubMed] [Google Scholar]
- 21. Triberti S, Repetto C, Riva G. Psychological factors influencing the effectiveness of virtual reality-based analgesia: a systematic review. Cyberpsychol Behav Soc Netw 2014; 17(6): 335–345. [DOI] [PubMed] [Google Scholar]
- 22. Loomis JM, Blascovich JJ, Beall AC. Immersive virtual environment technology as a basic research tool in psychology. Behav Res Methods Instrum Comput 1999; 31(4): 557–564. [DOI] [PubMed] [Google Scholar]
- 23. Sullivan M, Bishop S, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assessment 1995; 7: 524–532. [Google Scholar]
- 24. Scott W, Wideman TH, Sullivan MJ. Clinically meaningful scores on pain catastrophizing before and after multidisciplinary rehabilitation: a prospective study of individuals with subacute pain after whiplash injury. Clin J Pain 2013; 1–8. [DOI] [PubMed] [Google Scholar]
- 25. Picavet HS, Vlaeyen JW, Schouten JS. Pain catastrophizing and kinesiophobia: predictors of chronic low back pain. Am J Epidemiol 2002; 156(11): 1028–1034. [DOI] [PubMed] [Google Scholar]
- 26. Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med 2006; 166(10): 1092–1097. [DOI] [PubMed] [Google Scholar]
- 27. Lowe B, Decker O, Muller S, et al. Validation and standardization of the Generalized Anxiety Disorder Screener (GAD-7) in the general population. Medical Care 2008; 46(3): 266–274. [DOI] [PubMed] [Google Scholar]
- 28. Osman A, Barrios FX, Gutierrez PM, et al. The Pain Catastrophizing Scale: further psychometric evaluation with adult samples. J Behav Med 2000; 23(4): 351–365. [DOI] [PubMed] [Google Scholar]
- 29. Lee JE, Watson D, Frey-Law LA. Psychological factors predict local and referred experimental muscle pain: a cluster analysis in healthy adults. Eur J Pain 2013; 17(6): 903–915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Magerl W, Krumova EK, Baron R, et al. Reference data for quantitative sensory testing (QST): refined stratification for age and a novel method for statistical comparison of group data. Pain 2010; 151(3): 598–605. [DOI] [PubMed] [Google Scholar]
- 31. Munoz-Garcia D, Lopez-Uralde-Villanueva I, Beltran-Alacreu H, et al. Patients with concomitant chronic neck pain and myofascial pain in masticatory muscles have more widespread pain and distal hyperalgesia than patients with only chronic neck pain. Pain Med 2016. [DOI] [PubMed] [Google Scholar]
- 32. Kroenke K, Spitzer RL, Williams JB, et al. Anxiety disorders in primary care: prevalence, impairment, comorbidity, and detection. Ann Intern Med 2007; 146(5): 317–325. [DOI] [PubMed] [Google Scholar]
- 33. Wager TD, Atlas LY, Lindquist MA, et al. An fMRI-based neurologic signature of physical pain. N Engl J Med 2013; 368(15): 1388–1397. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Woo CW, Koban L, Kross E, et al. Separate neural representations for physical pain and social rejection. Nature Commun 2014; 5: 5380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35. Chang LJ, Gianaros PJ, Manuck SB, et al. A sensitive and specific neural signature for picture-induced negative affect. PLoS Biol 2015; 13(6): e1002180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36. Krishnan A, Woo CW, Chang LJ, et al. Somatic and vicarious pain are represented by dissociable multivariate brain patterns. eLife 2016; 5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Corradi-Dell’Acqua C, Hofstetter C, Vuilleumier P. Felt and seen pain evoke the same local patterns of cortical activity in insular and cingulate cortex. J Neurosci 2011; 31(49): 17996–18006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Woo CW, Roy M, Buhle JT, et al. Distinct brain systems mediate the effects of nociceptive input and self-regulation on pain. PLoS Biol 2015; 13(1): e1002036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39. Walton DM, Macdermid JC, Nielson W, et al. Reliability, standard error, and minimum detectable change of clinical pressure pain threshold testing in people with and without acute neck pain. J Orthop Sport Phys 2011; 41(9): 644–650. [DOI] [PubMed] [Google Scholar]
- 40. Kamper SJ, Maher CG, Hush JM, et al. Relationship between pressure pain thresholds and pain ratings in patients with whiplash-associated disorders. Clin J Pain 2010. [DOI] [PubMed] [Google Scholar]
- 41. Siegenthaler A, Eichenberger U, Schmidlin K, et al. What does local tenderness say about the origin of pain? An investigation of cervical zygapophysial joint pain. Anesth Analg 2010; 110(3): 923–927. [DOI] [PubMed] [Google Scholar]