

Abstract
Our study aimed to investigate the changes of white matter microstructure of cortico-subcortical pathways using diffusion tensor imaging (DTI), and to explore the relationship between abnormal parameters of DTI and cognitive function underlying in patients with leukoaraiosis (LA).
A total of 42 patients with LA and 42 age- and sex-matched healthy controls were recruited from Beijing Chaoyang Hospital, Capital Medical University between January 2012 and December 2012. All the subjects underwent scans of conventional magnetic resonance imaging and DTI, and a comprehensive neuropsychological battery was utilized. The regions of interest (ROIs) were located at the white matter of centrum semiovale, anterior and posterior periventricular white matter, basal ganglia, corpus callosum. The averaged values of mean diffusivity (MD) and fractional anisotropy (FA) were quantified both within white matter lesions (WMLs) and normal appearing white matter (NAWM). A linear regression analysis was performed to assess the association between diffusion parameters and decline in cognitive domains.
Patients with LA were associated with comprehensive cognitive function deficits. We found that significantly decreased FA and increased MD in WMLs at the 5 ROIs than that of NAWM and controls (P < .05). The values of FA in NAWM were significantly lower and MD in NAWM were significantly higher at centrum semiovale and posterior periventricular white matter than that of controls (P < .05). The values of FA in WMLs at anterior periventricular white matter were positively related to the performances of cognition in patients with LA (P < .05). The values of FA in NAWM located at anterior periventricular white matter were positively related to the score of Digit-symbol test (r = 0.446, P = .002). The values of FA in NAWM located at anterior periventricular white matter correlated inversely with the Z scores of executive function (r = −0.418, P = .03).
In our study, patients with LA exhibited significant cognitive impairment especially in the domains of executive function. The technique of DTI revealed that the reduced FA and increased MD at the corresponding regions of cortico-subcortical pathways in patients with LA. DTI may be of great help for an early pathology of white matter microstructure underlying in patients with LA.
Keywords: cognitive impairment, diffusion tensor imaging, leukoaraiosis
1. Introduction
Leukoaraiosis (LA) is also known as white matter lesion (WML) or age-related white matter changes (ARWMC). It refers to specked or patchy change in the periventricular or subcortical white matter of multiple causes. Studies have shown that LA patients have evident cognitive impairment,[1,2] but the underlying neural mechanism remains still unclear and might be associated with the damage to the prefrontal-striatal pathway.[3,4] In recent years, diffusion tensor imaging (DTI), a new functional magnetic resonance imaging, is developed for the quantification of the diffusion of water in tissues, and then the fractional anisotropy (FA) of water in tissues is used to infer the ultrastructure characteristics and pathological changes. To date, DTI has been an effective measure used to investigate the white matter microstructure and integrity. DTI may be used to explore the neural mechanism underlying the cognitive impairment. DTI has advantages in the detection of abnormalities in the normal appearing white matter (NAWM)[5] and is helpful for the early identification of white matter microstructure change in LA patients.[6,7] The common parameters used in DTI include FA, apparent diffusion coefficient (ADC) and mean diffusivity (MD). This study aimed to investigate the early diagnosis of LA with DTI and its relationship with cognitive impairment in LA patients, which may provide theoretical evidence for the prevention and therapy of early dementia.
2. Methods
2.1. Subjects
LA patients: LA was defined as diffuse or confluent white matter hyperintensity in the periventricular or subcortical white matter observed on T2-weighted magnetic resonance imaging (MRI) or fluid attenuated inversion recovery (FLAIR). Forty-two patients with LA were consecutively recruited from Department of Neurology, Beijing Chaoyang Hospital between January 2012 and December 2012. The average age was 74.8 ± 6.1 years. The average education was 7.1 ± 3.8 years. The mean time of education was 7.1 ± 3.8 years. Inclusion criteria included: patients were ≥60 years; cranial MRI confirmed WML of different extents; evaluation with daily life scale showed no functional disability. Exclusion criteria included: there were severe internal diseases (such as heart diseases, liver diseases, renal failure, tumor or other systemic diseases; there were severe neurological disease (such as white matter lesions unrelated to vascular diseases [immune, demyelination, metabolism, toxicity, infection, and other factors], tumor, stroke, Parkinson disease, and brain trauma); there were severe neuropsychological disorders, mental disease, and no medication with drugs affecting cognition within prior 24 hours; there were contradictions to MRI and patients were unable to receive cranial MRI.
Control group: 42 healthy community volunteer control subjects also were recruited. The average age was 70.2 ± 8.9 years. The average education was 8.7 ± 3.4 years. Healthy subjects who were ≥60 years and had no history of neurological and mental diseases were recruited in the same period from Beijing Chaoyang Hospital. Cranial MRI showed normal, and no abnormalities were identified by neurological examination. There were 7 males and 14 females. The mean age was 70.2 ± 8.9 years. The mean time of education was 8.7 ± 3.4. There were no significant differences in the age, gender, and education level between 2 groups (P < .05).
This study was approved by the Ethics Committee of Affiliated Beijing Chaoyang Hospital of Capital Medical University, and informed consent was obtained from each patient before study.
2.2. Methods
Our neuropsychological assessments mostly followed the protocol of LADIS study. The neuropsychological test battery included the mini-mental state examination (MMSE), Montreal cognitive assessment (MoCA), digit span test, trail making test (TMT), digit-symbol test, the Stroop test, and verbal fluency test. The verbal fluency test was instructed by asking the participants to generate as many names of animals that they could think of in 1 minute. The MMSE and MOCA were considered a global measure of cognitive function. The 24 stems of Hamilton depression scale (HAMD) were also performed to assess the severity of depressive disorders.
2.3. Data collection of MRI
2.3.1. MRI scanning
All data were acquired on a 3.0 Tesla Siemens MAGNETOM TIM Trio whole-body MR system (Siemens, Erlangen, Germany) with an 8-channel phased-array head coil. The head was fixed with a sponge mat. All the patients and controls received sagittal T1-weighted image (T1WI) scanning first, and then axial scanning. Scanning was performed at the central sagittal layer parallel to the AC-PC line. Routine cranial MRI was done with sagittal T1WI, axial T2W1, and axial FLAIR. The unknown lesions were excluded. Once normality was confirmed, following scanning was performed: T1WI: sagittal, 3-dimensional volume acquisition, pulse repetition interval = 1900 ms, echo time = 2.52 ms; TI = 900 ms; flip angle = 97°, scanning field = 250 mm × 250 mm; slice thickness = 5 mm; slice interval = 1.5 mm; T2WI: axial; FSE sequence; pulse repetition interval = 4500 ms; echo time = 93 ms; slice thickness = 5 mm; slice interval = 1.5 mm; scanning field = 220 mm × 220 mm; T2-FLAIR: axial; pulse repetition interval = 8000 ms; echo time = 86 ms; slice thickness = 5 mm; slice interval = 1.5 mm; scanning field = 220 mm × 220 mm; DTI: axial; single-shot SE EPI sequence; pulse repetition interval = 7700 ms; echo time = 104 ms; slice thickness = 3.5 mm, slice interval = 0 mm; consecutive scanning of 35 slices; number of excitation = 2; scanning field = 230 mm × 230 mm; diffusion gradient exerted at 20 directions with b = 0, 1000 s/mm2, bandwidth = 1396 and slice number = 35.
2.3.2. Processing of DTI data
Two radiologists with rich experience in neuroimaging observed the images and measured the parameters. The region of interest (ROI) was delineated in the Leonardo workstation (Siemens), and FA, ADC, and MD values were measured (Fig. 1). Slices used in this study include: frontal cortex localizes superior frontal gyrus and middle frontal gyrus at slices 3, 4, and 5 anterior to the top of lateral ventricle and above the genu of corpus callosum, and ROI localizes at 9, 10, and 46 regions of Brodmann region; putamen; gyri callosus; genu and body of corpus callosum; lenticular nucleus; caudate nucleus; pulvinar (Fig. 1); crus posterius capsulae internae; crus anterius capsulae internae.
Figure 1.
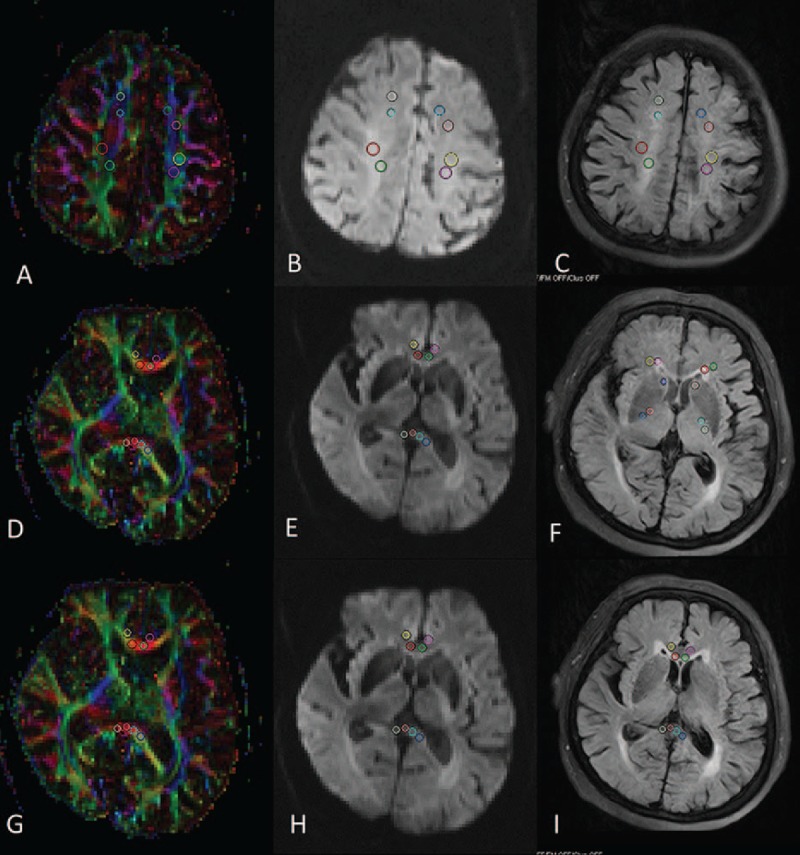
Measurement of ROIs in the same LA patient. A, D, G, FA. B, E, H, ADC. C, F, I, Axial FLAIR, measurement of NAWN in the frontal lobe, crus posterius capsulae internae, head of caudate nucleus, and corpus collosum as well as LA at white matter. Measurements were matched at the location in FLAIR, assuring the localization accuracy. FLAIR = fluid-attenuated inversion recovery, LA = leukoaraiosis, NAWM = normal appearing white matter, ROI = region of interest.
To reduce the diffusion gradient vortex-induced image distortion, the above ROIs were selected from high-resolution readily available sequence (FSE sequence). Then, image synchronization and positioning technique was used for analysis and measurement on the basis of FA and ADC. To avoid volume effect, the ROIs did not include gray matter, cerebrospinal fluid, scalp, and skull. At each brain region, values from different slices were averaged. For the bilateral ROIs, left and right means were used for statistical analysis. The DTI signal characteristics are related to the selection of ROIs. Thus, ROI of the same size was used in the same anatomic structure (especially the small anatomic structure). Measurement was done thrice in a blind manner, and average was calculated. The examinee was blinding to the grouping.
2.4. Statistical analysis
Statistical analysis was performed with SPSS version 16.0. All the data were subjected to tests for normal distribution and homogeneity of variance. Data with normal distribution and homogeneity of variance are expressed as mean ± standard deviation ( ± s) and compared with t test and 1-way analysis of variance (ANOVA). Data with normal distribution and heterogeneity of variance were compared with approximate analysis of variance, and data with abnormal distribution with nonparametric test. Paired comparisons of means were done with least significant difference procedure (L-S-D). Qualitative data are expressed as percentage and compared with χ2 test. Correlation between cognition function score and DTI parameters was evaluated with Pearson correlation analysis. A value of P < .05 was considered statistically significant.
± s) and compared with t test and 1-way analysis of variance (ANOVA). Data with normal distribution and heterogeneity of variance were compared with approximate analysis of variance, and data with abnormal distribution with nonparametric test. Paired comparisons of means were done with least significant difference procedure (L-S-D). Qualitative data are expressed as percentage and compared with χ2 test. Correlation between cognition function score and DTI parameters was evaluated with Pearson correlation analysis. A value of P < .05 was considered statistically significant.
3. Results
3.1. General characteristics and cognition function
There were no significant differences in the age, gender, and education level between LA patients and healthy controls (P > .05). In addition, the risk factors of cerebrovascular disease (such as hypertension, diabetes mellitus, coronary heart disease, and history of smoking) were also comparable between 2 groups (P > .05) (Table 1).
Table 1.
General characteristics and cognition function of LA patients and controls.
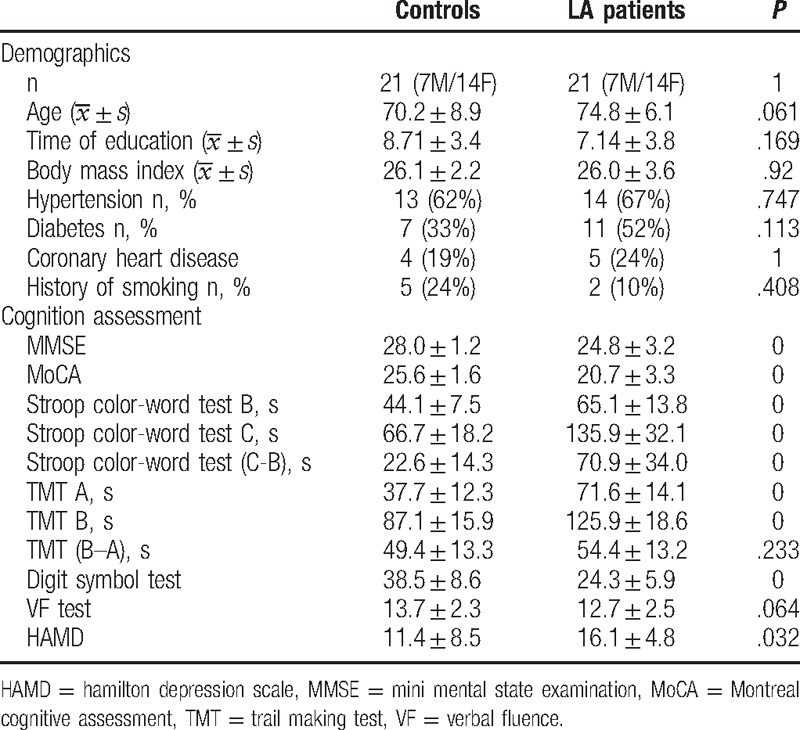
LA patients had evident cognitive impairment and manifested significant reductions in MMSE and MoCA (P < .05). Moreover, LA patients had evident executive function impairment and there were differences in the scores of Stroop B, Stroop C, Stroop (C-B), TMT-A, TMT-B, and digit symbol test between 2 groups (P < .05). In addition, significant difference in HAMD score was also observed between LA patients and controls (P < .05).
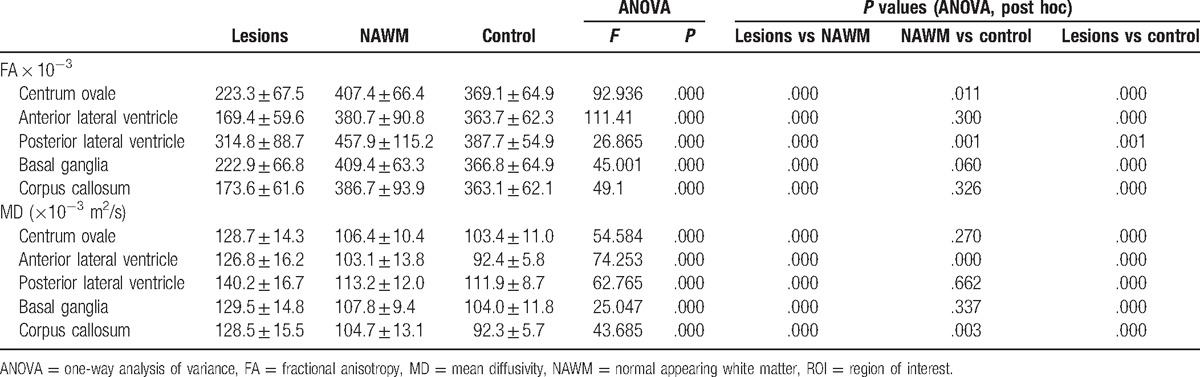
3.2. FA and MD of ROI in two groups
The FA of WML at centrum ovale and anterior and posterior lateral ventricle in LA patients was significantly lower than that of NAWM and controls (P < .05), but MD was markedly higher than that of NAWM and controls (P < .05). The FA of NAWM at centrum ovale and posterior lateral ventricle in LA patients was significantly lower than in controls, but MD of NAWM at anterior lateral ventricle in LA patients was significantly higher than in controls (P < .05) (Table 2).
Table 2.
FA and MD of ROI in two groups.
3.3. Correlation of FA and MD of different brain regions with cognition function in LA patients
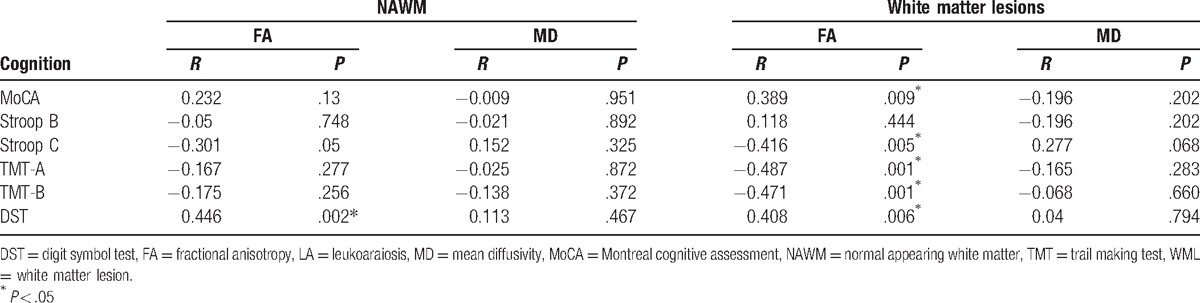
As shown in Table 3, the FA of WML at anterior lateral ventricle was positively related to the scores of MoCA, Stroop B, Stroop C, TMT-A, TMT-B, and digit symbol test (DST) in LA patients (P < .05). The FA of NAWM of anterior lateral ventricle was positively related to DST (P < .05). The MD of WML and NAWM had no relationship with cognition function (Table 3).
Table 3.
Correlation of FA and MD of WML and NAWM with cognition function in LA patients.
4. Discussion
DTI is a new, noninvasive MRI and can detect the diffusion of water in the brain tissues to provide information on the tissue structure. FA represents the fractional anisotropy and reflects the degree of water diffusion in anisotropy tissues (such as white matter). In the brain, FA is affected by the diameter, density, and extent of myelination of nerve fibers. It may reflect the integrity of nerve fibers in the white matter of the brain and has been used as a sensitive indicator reflecting the damage to white matter tracts: the higher the FA, the better the directivity of tissues and the better the degree of tract bonding are. The axonal missing may compromise the barrier to water, which then changes the DTI-related parameters. The neurological pathology of LA (such as axonal missing) is consistent with the gliosis, which might be related to the disordered neural network regulation.[8,9] DTI may also display the integrity of NAWM at the white matter that cannot be identified by traditional MRI.[6]
The left hemisphere is involved in the cognition activities such as language and language-related memory, and the right hemisphere is involved in visuospatial function and related memory and cognition. The division of the work between hemispheres has involvement of both cortex and subcortical structures. Studies have revealed that damage to the left hemisphere may cause cognitive impairment,[10] which may be ascribed to that the left hemisphere is dominant hemisphere in most people and dominant hemisphere is more susceptible to cognitive impairment as compared with nondominant hemisphere.[10] In this study, DTI was employed to detect LA patients. Results showed the FA of WML at the centrum ovale and anterior and posterior lateral ventricle of left hemisphere reduced significantly, but MD increased markedly as compared with NAWM and controls. In addition, FA of NAWM at centrum ovale and posterior lateral ventricle of left hemisphere in LA patients was significantly lower than that in controls, and the MD of NAWM at the left anterior lateral ventricle was markedly higher than in controls, which were consistent with the language dysfunction in LA patients.[11] Our results indicate the impairment of the white matter neural fibers in LA patient is not confined to the abnormal region shown by routine MRI-T2, but may be present in NAWM shown by routine MRI-T2.
Several studies have confirmed that the change in DTI parameters of NAWM is clinically important. O'Sullivan et al[12] found FA reduced in a linear manner and MD increased over age, which were more obvious at the anterior white matter of lateral ventricle. In addition, MD of anterior lateral ventricle is closely related to executive function (TMT), supporting the cortical disconnection hypothesis (white matter damage causes cognitive impairment).[12] This group conducted another DTI study in 36 patients with ischemia-related LA and 19 controls, and their results showed MD of WML and NAWM increased, which was closely associated with total IQ (Wechsler Intelligence Scale) and executive function, suggesting that DTI has advantages in the detection of white matter integrity and microvascular disease-induced cognitive impairment.[6] Our findings were basically consistent with the above results, and indicated that there were characteristic changes in the white matter of LA patients including the white matter of WML and that of NAWM not shown in routine MRI. Thus, DTI is superior to routine MRI in the detection of cognitive impairment of ischemic cerebrovascular disease patients.[13,14] These changes might be related to the neuropathology of LA (such as axonal loss and gliosis). The axons serve as a barrier to water diffusion. The axonal loss may compromise the barrier function and then the water will increase in tissues, leading to the changes in DTI-related parameters.[15] These characteristic changes in DTI are helpful for the early identification of brain lesions, disease monitoring, and evaluation of therapeutic efficacy.
Currently, it is accepted that executive dysfunction is associated with the prefrontal-striatal pathway impairment.[13] The prefrontal-striatal pathway impairment may cause damage to the top-down control in the prefrontal lobe, resulting in executive dysfunction syndrome[16] which is characterized by abnormalities in the executive control, working memory, and dominant response inhibition as well as psychomotor retardation. Some studies propose that WML mainly affect the structure and function of prefrontal-striatal pathway[17] and disrupt the signal transduction between neurons and between prefrontal cortex and subcortical center, finally leading to the executive dysfunction.[18] Raji et al[19] also found that the cortical thickness at the prefrontal lobe reduced, implying that subcortical pathway is also abnormal.[9] In 2012, our group also found that the concentration of NAA/Cho metabolites in the prefrontal lobe changed as shown by magnetic resonance spectroscopy in LA patients.[20] This study confirmed the change in the white matter microstructure diffusion of prefrontal-striatal pathway, which was consistent with the findings from the study of Yang et al.[21]
Taken together, we speculate that brain lesions in LA patient may affect the regulation and information processing of neural pathway in the brain,[22] and DTI is more sensitive and objective to reflect the early damage to the white matter microstructure, cognitive impairment, executive dysfunction, and change in the brain network system. Thus, it is an effective technique to investigate the pathogenesis of diseases and aging as well as the relationship between function and structure, and may provide evidence for the clinical monitoring of diseases and the evaluation of therapeutic efficacy. In future studies, the sample size should be increased, more specific method should be used for neuropsychological assessment, and combined use of other MRI techniques is necessary to explore the neural mechanism underlying the cognitive impairment in LA patients.
Footnotes
Abbreviations: ADC = apparent diffusion coefficient, ANOVA = one-way analysis of variance, ARWMC = age-related white matter changes, DTI = diffusion tensor imaging, FA = fractional anisotropy, HAMD = Hamilton depression scale, LA = leukoaraiosis, L-S-D = least significant difference procedure, MD = mean diffusivity, MMSE = mini mental state examination, MoCA = Montreal Cognitive Assessment, NAWM = normal appearing white matter, ROI = region of interest, T1WI = T1-weighted image, TMT = trail making test, VF = verbal fluence, WML = white matter lesion.
This study was supported by the National Natural Science Foundation of China (81301016 and 81541129).
The authors have no conflicts of interest to disclose.
References
- [1].Te M, Zhao E, Zheng X, et al. Leukoaraiosis with mild cognitive impairment. Neurol Res 2015;37:410–4. [DOI] [PubMed] [Google Scholar]
- [2].Frederiksen KS, Verdelho A, Madureira S, et al. Physical activity in the elderly is associated with improved executive function and processing speed: the LADIS Study. Int J Geriatr Psychiatry 2015;30:744–50. [DOI] [PubMed] [Google Scholar]
- [3].Macfarlane MD, Looi JC, Walterfang M, et al. Executive dysfunction correlates with caudate nucleus atrophy in patients with white matter changes on MRI: a subset of LADIS. Psychiatry Res 2013;214:16–23. [DOI] [PubMed] [Google Scholar]
- [4].Kim TW, Kim YH, Kim KH, et al. White matter hyperintensities and cognitive dysfunction in patients with infratentorial stroke. Ann Rehabil Med 2014;38:620–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [5].Jeantroux J, Kremer S, Lin XZ, et al. Diffusion tensor imaging of normal-appearing white matter in neuromyelitis optica. J Neuroradiol 2012;39:295–300. [DOI] [PubMed] [Google Scholar]
- [6].O'Sullivan M, Morris RG, Huckstep B, et al. Diffusion tensor MRI correlates with executive dysfunction in patients with ischaemic leukoaraiosis. J Neurol Neurosurg Psychiatry 2004;75:441–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].O'Sullivan M, Summers PE, Jones DK, et al. Normal-appearing white matter in ischemic leukoaraiosis: a diffusion tensor MRI study. Neurology 2001;57:2307–10. [DOI] [PubMed] [Google Scholar]
- [8].Nitkunan A, Charlton RA, McIntyre DJ, et al. Diffusion tensor imaging and MR spectroscopy in hypertension and presumed cerebral small vessel disease. Magn Reson Med 2008;59:528–34. [DOI] [PubMed] [Google Scholar]
- [9].Lambert C, Sam Narean J, Benjamin P, et al. Characterising the grey matter correlates of leukoaraiosis in cerebral small vessel disease. Neuroimage Clin 2015;9:194–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Li CM, Gui L, Du HJ, et al. A magnetic resonance imaging study of the gray matter configuration in amnestic mild cognitive impairment patients. Chin J Neurol 2010;43:853–7. [Google Scholar]
- [11].Welker KM, De Jesus RO, Watson RE, et al. Altered functional MR imaging language activation in elderly individuals with cerebral leukoaraiosis. Radiology 2012;265:222–32. [DOI] [PubMed] [Google Scholar]
- [12].O'Sullivan M, Jones DK, Summers PE, et al. Evidence for cortical “disconnection” as a mechanism of age-related cognitive decline. Neurology 2001;57:632–8. [DOI] [PubMed] [Google Scholar]
- [13].Xu Q, Zhou Y, Li YS, et al. Diffusion tensor imaging changes correlate with cognition better than conventional MRI findings in patients with subcortical ischemic vascular disease. Dement Geriatr Cogn Disord 2010;30:317–26. [DOI] [PubMed] [Google Scholar]
- [14].Yuan J, Wang S, Guo X, et al. [Association of diffusion tensor imaging abnormalities with executive dysfunction in patients with leukoaraiosis]. Zhonghua Yi Xue Za Zhi 2015;95:3650–4. [PubMed] [Google Scholar]
- [15].Lin Q, Huang WQ, Tzeng CM. Genetic associations of leukoaraiosis indicate pathophysiological mechanisms in white matter lesions etiology. Rev Neurosci 2015;26:343–58. [DOI] [PubMed] [Google Scholar]
- [16].Alves GS, Alves C, Lanna ME, et al. Subcortical ischemic vascular disease and cognition: a systematic review. Dement Neuropsychol 2008;2:82–90. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [17].Lamar M, Price CC, Libon DJ, et al. Alterations in working memory as a function of leukoaraiosis in dementia. Neuropsychologia 2007;45:245–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Mascalchi M, Ginestroni A, Toschi N, et al. The burden of microstructural damage modulates cortical activation in elderly subjects with MCI and leuko-araiosis. A DTI and fMRI study. Hum Brain Mapp 2014;35:819–30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Raji CA, Lopez OL, Kuller LH, et al. White matter lesions and brain gray matter volume in cognitively normal elders. Neurobiol Aging 2012;33: 834.e7–16. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Yuan JL, Wang SK, Guo XJ, et al. [Correlates of cognitive impairment in patients with leukoaraiosis by magnetic resonance spectroscopy]. Zhonghua Yi Xue Za Zhi 2012;92:303–6. [PubMed] [Google Scholar]
- [21].Yang YH, Liang PP, Qin W, et al. DTI study of the white matter of Dorsalaterai Prefrontal Cortex in patients with mild cognitive impairment. J Clin Radiol 2010;29:432–5. [Google Scholar]
- [22].Pantoni L, Fierini F, Poggesi A. Impact of cerebral white matter changes on functionality in older adults: an overview of the LADIS study results and future directions. Geriatr Gerontol Int 2015;15suppl 1:10–6. [DOI] [PubMed] [Google Scholar]