

Abstract
Background:
Condylar resorption as a cause of relapse after orthognathic surgery is well known. Several authors have presented evidence of the relation between orthognathic surgery and condylar remodeling and resorption. This study was done to appraise the condylar changes along with the form and function following orthognathic surgery, as well as to assess what factors may have contributed to the problems.
Methodology:
A diagnosis of progressive condylar resorption (PCR) was made by comparison of preoperative and postoperative radiographs (cephalometric radiograms), as well as clinical evaluations. The radiographs were taken for each patient preoperatively and postoperatively, which include immediately after osteotomy, at 6 months and 24 months. Additional radiographs were taken when required. Then, preoperative and postoperative tracings were compared at 24 months postoperatively.
Results and Conclusion:
It can be concluded from this study that females of relative low age (<18 years) appeared to be a high-risk factor for the occurrence of condylar alteration including PCR. A steep mandibular plane angle, the low facial height ratio (post/ant), and magnitude of surgery were also significantly related to the occurrence of condylar alteration, but the multivariance regression showed that these parameters had only limited value.
Keywords: Cephalogram, condylar changes, condylar resorption, orthognathic surgery
Introduction
Functional and esthetic considerations are the reasons for patients seeking treatment for dentofacial deformities, yet osteotomies can contribute some unwanted alterations in the temporomandibular joint (TMJ) giving rise to temporomandibular dysfunction. Skeletal stability following advancement of the mandible through bilateral sagittal split osteotomy (BSSO) has been a subject of numerous investigations such as postoperative occlusion, TMJ changes, and mandibular condylar changes. Several authors have presented evidence of the relation between orthognathic surgery and condylar remodeling and various changes.[1,2,3,4,5,6] Ellis and Hinton have shown remodeling changes occurring in the TMJ after mandibular advancement surgery in the adult Macaca mulatta monkey.[2] Condylar resorption was first reported by Burke in 1961.[3] Condylar resorption is an irreversible complication following orthognathic surgery.
The term progressive condylar resorption (PCR) was coined by Arnett and Tamborello.[4] The BSSO may cause alteration of the position of the condyle in the fossa. The mediolateral torquing or posterior positioning of the condyle after rigid fixation might be associated with condylar resorption and late relapse. PCR is a serious complication that gives rise to frustration for both the patient and the clinician. There is often a dilemma as to what to do when the occlusion is not stable or the esthetic result not acceptable. Condylar changes are seen in terms of progressive alteration of condylar shape and decrease in mass. As a result, most patients exhibit a decrease in posterior facial height (PFH) and retrognathism. Although the cause is unknown, condylar resorption has been associated with various systemic diseases, trauma, neoplasia, orthodontic treatment, and orthognathic surgery.[4] In this retrospective study, we have tried to evaluate the long-term treatment results of 25 patients with regards to condylar changes following orthognathic surgery. Condylar changes were diagnosed clinically and from a comparison of pre- and post-operative cephalometric and orthopantomographic (OPG) radiographs.
The aim of this retrospective study was to evaluate the long-term treatment results of 25 patients who developed condylar changes following orthognathic surgery and to identify possible predisposing factors for condylar resorption. The main objectives of the study were to evaluate the condylar changes following orthognathic surgery, to evaluate decrease in height of ramus and PFH, and to identify the factor influencing the condylar changes. In addition, the study shows the importance of evaluating preoperative and postoperative condylar changes and suggests the clinician to consider the role of orthognathic surgery.
Methodology
A total of 25 patients (15 females and 10 males) were operated and evaluated for dentofacial deformity by orthognathic surgery (BSSO). Among these 25 patients, 15 patients underwent mandibular advancement procedure, and 10 underwent mandibular setback procedure. The mean age at the time of operation was 19.6 years 13 patients had an open bite at the time of operation and 12 had a deep bite. The lateral cephalograms and OPG radiographs were taken at preoperative (T1), immediate postoperative (T2), 6 months (T3), and 2 years (T4) postoperatively. The internal fixation was made by means of monocortical plate osteosynthesis without intermaxillary fixation. Minor occlusal corrections were obtained by orthodontic procedures postoperatively.
According to age, these 25 patients again subdivided into three subgroups. Group 1 contains patients <18 years of age (n = 11), Group 2 has the patients from 19 to 21 years (n = 9), and Group 3 contains more than 21 years (n = 5)
According to the mandibular plane angle (MPA): The patients were divided into two groups. Group 1 with MPA <28° and Group 2 with MPA ≥28°
According to the type of surgery, these patients were again subdivided into two groups. Group 1 with mandibular advancement procedure (n = 15) and Group 2 with setback procedure (n = 10)
According to the magnitude, these subgroups are again subcategorized into Group A advancement (Aadv) and A setback (Asb) and B advancement (Badv) and B setback (Bsb) with <6 mm and more than 6, respectively.
All the divided groups and subgroups compared with the different values of condylar changes. Because the condylion is hard to define, the articulare (Ar) was chosen for measurement. The distance from Ar to gonion (Go) and PFH was measured on lateral cephalograms at immediate and 2 years postoperatively so that the shortening could be calculated in relation to the total length of ramus. The distance between Ar to mini-plate was also measured to evaluate condylar changes following in all the cases at T1, T2, T3, and T4. All the patients were evaluated for changes in condyle based on the radiographic findings as mentioned earlier. During the statistical analysis, the level of significance was adjusted to 5% and confidence interval at 95%. P <0.05 was considered as significant, while a P < 0.001 suggested highly significant value and P > 0.05 was considered statistically insignificant.
Results
This is a retrospective study based on an evaluation of 25 patients who were operated for dentofacial deformity by orthognathic surgery (bilateral sagittal split osteotomy, both advancement, and setback).
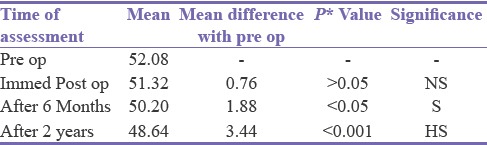
The measured mean values from Ar to Go of 25 patients are at T1-52.72, at T2-51.24, at T3-50.20, and T4-48.64.
Among these 25 patients, 15 were females (60%) and 10 were males (40%). In group of males, the mean value at T1 is 56.40 mm, at T2-55.20 mm, at T3-55.20 mm, and T4-54.40 mm were measured, and repeated measure ANOVA test and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P > 0.005. This was statistically not significant and showed no condylar changes between T1 and T3 and T1 and T4. Whereas, in group of females, the mean value at T1 is 49.20 mm, at T2-48.73 mm, at T3-46.87 mm, and T4-44.80 mm were measured, and repeated measure ANOVA test and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.001. This is statistically highly significant and shows condylar changes between T1 and T3 and T1 and T4 in males and females [Table 1].
Table 1.
Comparison between males and females

According to age, in group 1, the mean value at T1 is 52.18 mm, at T2-50.91 mm, at T3-49.82 mm, and T4-47.18 mm were measured, and repeated measure ANOVA and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.001. This is statistically highly significant and shows the condylar changes between T1 and T3 and T1 and T4. In Group 2, the mean value at T1 is 55.22 mm, at T2-53.22 mm, at T3-52.11 mm, and T4-51.67 mm were measured, and repeated measure ANOVA and Tukey's tests were applied to compare condylar changes between these different radiographic values and found the P < 0.005. This is statistically significant and shows the condylar changes between T1 and T3 and T1 and T4. In Group 3, the mean value at T1 is 49.40 mm, at T2-48.40 mm, at T3-47.60 mm, and T4-46.40 mm were measured, and repeated measure ANOVA and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.005. This is statistically significant and shows the condylar changes between T1 and T4 [Table 2]. Descriptive statistical data of condylar changes have been mentioned in Table 3. According to the type of surgery for Group 1 (advancement), the mean values at T2-1.13 mm, at T3-2.53 mm, at T4-4.47 mm were measured. And for Group 2 (setback), these values are at T2-2.00 mm, at T3-2.50 mm, and at T4-3.50 mm.
Table 2.
Comparison of condylar changes in age group
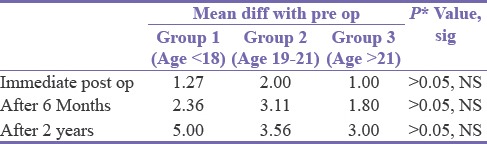
Table 3.
Descriptive statistics of condylar changes
According to the magnitude of surgery, in group Aadv, the mean value at T1 is 49.86 mm, at T2-48.71 mm, at T3-47.86 mm, and T4-46.14 mm were measured, and repeated measure ANOVA and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.005. This is statistically significant and shows the condylar changes between T1 and T3 and T1 and T4. In group Badv, the mean value at T1 is 51.88 mm, at T2-50.75 mm, at T3-48.88 mm, and T4-46.75 mm were measured, and repeated measure ANOVA and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.001. This is statistically highly significant and shows the condylar changes between T1 and T3 and T1 and T4. In group Asb, the mean value at T1 is 55.40 mm, at T2-53.20 mm, at T3-53.80 mm, and T4-53.20 mm were measured, and repeated measure ANOVA and Tukey's test were applied to compare condylar changes between these different radiographic values and found the P > 0.005. This is statistically not significant and shows no condylar changes between T1 and T3 and T1 and T4.
In group Bsb, the mean value at T1 is 55.40 mm, at T2-53.60 mm, at T3-52.00 mm, and T4-50.60 mm were measured, and repeated measure ANOVA test with Tukey's test were applied to compare condylar changes between these different radiographic values and found the P < 0.001. This is statistically highly significant and shows condylar changes between T1 and T3 and T1 and T4 [Table 4].
Table 4.
Comparison between advancement and set back

According to correlation with PFH/anterior face height ratio (AFH) ratio, the correlation coefficient shows the values in negative, and P > 0.05 at T3 and T4 which is statistically insignificant [Table 5].
Table 5.
Correlation with PFH/AFH ratio

According to the MPA, the mean value of condylar changes in Group A is 6.75 mm, whereas in Group B, it is 4.50 mm. It shows P < 0.05, which is statistically significant [Table 6].
Table 6.
Comparison of resorption with respect to MPA

Discussion
PCR is defined as an extreme change in the structure of the condyle leading to a decrease in the height of the ramus and thus, PFH. The condylar changes seen following orthognathic surgery is termed as secondary condylar resorption wherein the causes in most of the cases are not definitive and hence the term “idiopathic condylar resorption is coined.”[3] With unclear etiopathogenesis patients who are prone to develop condylar resorption have certain well-defined characteristics such as presence of high MPA, presence of preexisting TMJ dysfunction, large surgical mandibular advancements, and counterclockwise rotation of proximal segment in BSSO, as well as women of younger age.
The incidence of condylar resorption after orthognathic surgery is reported to range from 1% to 31% depending on various nonsurgical and surgical factors.[5,6]
Incidence of condylar alteration, relation with gender and age group
To know the influence of gender on condylar changes, we divided the patients into two groups of males (40%) and females (60%) and results showed that incidence of condylar changes following orthognathic surgery is higher in females as compared to males. Idiopathic and secondary condylar resorption affect men, but they are more frequently seen in women, with a 9:1 ratio. The female preponderance may be attributed to the modulation of the bone response by estrogen and prolactin. Estrogen receptors have been found in the temporomandibular disk of women and in the condyle and disc of female animals. In a study of the human TMJ, it was reported that estrogen and progesterone receptors were found five times more often in women with symptoms of TMJ internal derangement than in asymptomatic women.[7,8] Puberty is a unique stage of growth and development as at this stage adolescent growth spurts take place and very considerable changes in growth rate occur. The beginning of increase of growth velocity is about 12–14 years, which on an average lasts for 2–3 years. It is noteworthy that in young patients condylar alterations were more often seen but with unknown etiology. In our study, the statistic results show that there are higher incidences of changes in condyle in younger age group. Information gained from a larger series of patients treated at a young age would be necessary to substantiate the suspicion that young patients are more prone to develop PCR.[5]
Incidence of condylar alteration, relation with type of surgery and magnitude
In the present study, condylar alterations were found more in mandibular advancement procedure than in setback and in a higher magnitude of surgery, i.e., advancement or setback >6 mm. In general mandibular advancement, procedure appears to be less stable than a mandibular setback. Skeletal relapse after surgery appears to be multifactorial. The stretching of perimandibular musculature, connective tissues, and periosteum results in tension that tends to pull the distal segment posteriorly. Larger advancements high MPA and low PFH/AFH can increase perimandibular tissue stretch. The musculature acting on mandible specially suprahyoid muscles receives most of the attention. After movement of mandible following surgery, the associated musculature is thought to provide a reverse force that eventually results in some degree of relapse. In recent years, most of the authors have indicated elongation and tension of the suprahyoid musculature as the primary cause of skeletal relapse. The hyoid bone is displaced in a forward direction after surgery, and it creates a muscular imbalance resulting in relapse.[9,10] With regard to the magnitude of mandibular advancement, analysis of 18 orthognathic surgery patients showed that relapse occurred in patients having surgery with mandibular advancements more than 5 mm. It was noted that large advancement would tend to generate greater muscular forces. The result suggested that these mandibles are subjected to strong sustained forces, causing the condyle to retruded position, more forcefully into the fossa and generating more tension within the joint, leading to joint remodeling or resorption.[1]
Incidence of condylar alteration, relation with occlusion and posterior-to-anterior facial height ratio
Our study showed that preoperative open bite had a higher influence on postoperative condylar changes. Of the 25 patients, 11 patients with open bite were seen to have noticeable condylar changes. In contrast to the patients having preoperative deep bite, only five patients showed the noticeable condylar changes.
Condyles in patients with anterior open bite appear to be very sensitive to functional loading, and their adaptive capacity is probably less than in patients with deep bites. The difference in morphology of mandibular condyles between the two groups was seen. Trabeculae in high angle condyles (open bite) were less dense and not discretely oriented as compared to the low angle variant (deep bite). From the present study, it appears that the risk of condylar resorption increases with the severity of open bite. There is a clear distinction between “deep bite” and “open bite” condylar resorption. Deep bite condylar resorption corresponds to resorption on the superior site of the condyle. Open bite condylar resorption develops with resorption on the superior and anterior sites of the condyle.[9,11]
We also evaluated the influence of PFH and anterior height ratio with the condylar changes. The result shows that the lower is the ratio between PFH/AFH higher are the chances of condylar changes. Lower PFH/AFH ratio tends to increase perimandibular tissue stretch, which would be a contributing factor leading to condylar changes following a surgical procedure.[9,12]
Incidence of condylar alteration, relation with mandibular plane angle
We found that the patients in Group A with high MPA showed more changes in condyle as compared to Group B. The lack of association between the preoperative MPA and mandibular relapse was of considerable interest. It has been noticed by various authors that high MPA is an indication for skeletal relapse. This is based on an apparent shorter geniohyoid distance preoperatively, with a greater stretching effect when the mandible is advanced.[13,14]
Conclusion
The girls and women of relative low age (<18 years) with anterior open bites, high MPA, short ramus height, low ratio of posterior-to-anterior facial height should be considered as a high-risk group for PCR in particular when a BSSO specially advancement is performed more than 6 mm. Considering all these predisposing factors, surgeons are advised to take precautions in planning orthognathic procedure for such group, and in patients with above-combined factors, preoperative counseling is highly recommended to inform the patient about possible risk in regard to condylar changes. Further studies are required to elucidate the influence of the different factors that may play a role in the etiology of PCR.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Kohn MW. Analysis of relapse after mandibular advancement surgery. J Oral Surg. 1978;36:676–84. [PubMed] [Google Scholar]
- 2.Ellis E, 3rd, Hinton RJ. Histologic examination of the temporomandibular joint after mandibular advancement with and without rigid fixation: An experimental investigation in adult Macaca mulatta. J Oral Maxillofac Surg. 1991;49:1316–27. doi: 10.1016/0278-2391(91)90311-9. [DOI] [PubMed] [Google Scholar]
- 3.Burke PH. A case of acquired unilateral mandibular condylar hypoplasia. Proc R Soc Med. 1961;54:507–10. [PMC free article] [PubMed] [Google Scholar]
- 4.Arnett GW, Tamborello JA. Progressive class II development: Female idiopathic condylar resorption. Oral Maxillofac Surg Clin N Am. 1990;2:699–716. [Google Scholar]
- 5.Arnett GW, Milam SB, Gottesman L. Progressive mandibular retrusion – Idiopathic condylar resorption. Part I. Am J Orthod Dentofacial Orthop. 1996;110:8–15. doi: 10.1016/s0889-5406(96)70081-1. [DOI] [PubMed] [Google Scholar]
- 6.De Clercq CA, Neyt LF, Mommaerts MY, Abeloos JV, De Mot BM. Condylar resorption in orthognathic surgery: A retrospective study. Int J Adult Orthodon Orthognath Surg. 1994;9:233–40. [PubMed] [Google Scholar]
- 7.Hwang SJ, Haers PE, Sailer HF. The role of a posteriorly inclined condylar neck in condylar resorption after orthognathic surgery. J Craniomaxillofac Surg. 2000;28:85–90. doi: 10.1054/jcms.2000.0129. [DOI] [PubMed] [Google Scholar]
- 8.Abubaker AO, Raslan WF, Sotereanos GC. Estrogen and progesterone receptors in temporomandibular joint discs of symptomatic and asymptomatic persons: A preliminary study. J Oral Maxillofac Surg. 1993;51:1096–100. doi: 10.1016/s0278-2391(10)80448-3. [DOI] [PubMed] [Google Scholar]
- 9.Aufdemorte TB, Van Sickels JE, Dolwick MF, Sheridan PJ, Holt GR, Aragon SB, et al. Estrogen receptors in the temporomandibular joint of the baboon (Papio cynocephalus): An autoradiographic study. Oral Surg Oral Med Oral Pathol. 1986;61:307–14. doi: 10.1016/0030-4220(86)90407-x. [DOI] [PubMed] [Google Scholar]
- 10.Will LA. Risks and benefits of orthognathic surgery. Oral Maxillofac Surg Clin N Am. 1997;9:179–93. [Google Scholar]
- 11.Fonseca RJ, Davis WH. Text Book of Oral and Maxillofacial Surgery, Orthognathic Surgery. Philadelphia: W.B Saunders Company; 1986. [Google Scholar]
- 12.Hoppenreijs TJ, Freihofer HP, Stoelinga PJ, Tuinzing DB, van’t Hof MA. Condylar remodelling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite: A clinical and radiological study aesthetic and reconstructive surgery. Int J Oral Maxillofac Surg. 1998;27:81–91. doi: 10.1016/s0901-5027(98)80301-9. [DOI] [PubMed] [Google Scholar]
- 13.Arnett GW. A redefinition of bilateral sagittal split osteotomy (BSSO) advancement relapse. Am J Orthod Dentofacial Orthop. 1993;104:306–10. doi: 10.1016/0889-5406(93)70076-Z. [DOI] [PubMed] [Google Scholar]
- 14.Arnett GW, Milam SB, Gottesman L. Progressive mandibular retrusion-idiopathic condylar resorption. Part II. Am J Orthod Dentofacial Orthop. 1996;110:117–27. doi: 10.1016/s0889-5406(96)70099-9. [DOI] [PubMed] [Google Scholar]