
Figure 2. Therapeutic vaccine immunotherapy for PDAC requires multiple steps to overcome immunosuppression.
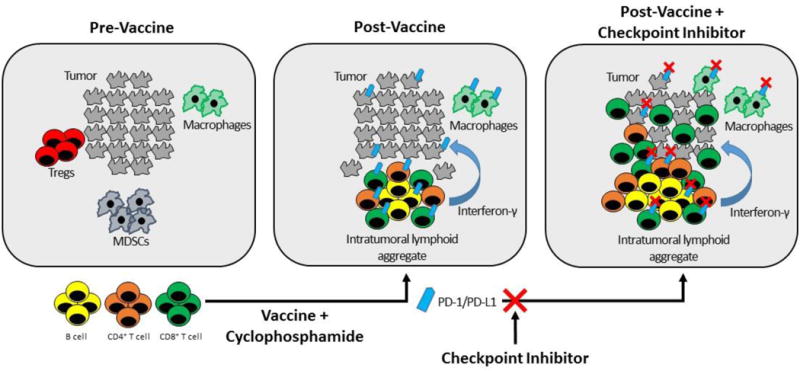
PDAC and other poorly immune responsive cancers are characterized by low numbers of tumor infiltrating lymphocytes (TILs), low levels of PD-L1 expression, and high numbers of immunosuppressive cells such as Tregs and MDSCs at baseline (left panel) (13). Using a vaccine approach will require at least two immunotherapeutics to achieve an immune response. In Step 1 (center panel), a therapeutic vaccine is used to induce accumulation of lymphoid aggregates (35). These lymphocytes secrete interferon gamma and other soluble factors that induce high levels of PD-L1/PD-1 expression on epithelial tumor cells and on immune cells (186). Vaccines can also be combined with other therapies such as cyclophosphamide, to deplete immunosuppressive cells in the TME (29). In Step 2 (right panel), the addition of a PD-pathway inhibitor to a vaccine-primed tumor inhibits PD-L1/PD-1 signaling to increase lymphocyte proliferation and activation and promote tumor eradication (36). The hypothesis that vaccine therapy can synergize with immune checkpoint inhibition is currently under clinical investigation in multiple trials in PDAC.