

Supplemental Digital Content is available in the text
Keywords: branched-chain amino acid, complication, liver cirrhosis, nutrition, prognosis
Abstract
Evidence of the potential benefits of long-term oral branched-chain amino acid (BCAA) supplementation in reducing the severity of liver disease is limited.
Patients who were diagnosed with liver cirrhosis with a Child–Pugh (CP) score of 8–10 were included. The BCAA group consumed BCAAs daily for at least 6 months, and the control group consumed a diet without BCAA. We analyzed the improvements based on the model for end-stage liver disease (MELD) score, CP score, incidence of cirrhosis-related complications, and event-free survival over 2 years. Among the 867 recruited patients, 307 (166 in the BCAA group and 141 in the control group) were analyzed. The BCAA group was divided into 3 subgroups, whose patients consumed 4.15 g, 8.3 g, or 12.45 g of BCAAs daily for the analysis. There were significant differences in the CP score, albumin, and hepatic encephalopathy between the 2 groups at baseline. After matching the propensity scores, we analyzed patients in the BCAA-12.45 g group (12.45 g of BCAAs daily, n = 41) and matched control group (n = 41). The MELD score significantly improved in the BCCA-12.45 g group compared to the matched control group (P = .004). The changes in the serum bilirubin level (P = .014) and CP score (P = .033) over time also differed significantly between the 2 groups. The incidence rates of cirrhosis-related complications (P = .973) and development of hepatocellular carcinoma (2 cases each) did not differ significantly between the 2 groups.
Long-term oral BCAA supplementation has beneficial effects in patients with advanced liver cirrhosis. A further large-scale prospective study is needed to delineate these beneficial effects.
1. Introduction
The progression of chronic liver disease results in diminished hepatic glycogen stores due to a catabolic state that requires a higher protein intake than usual.[1,2] The negative nitrogen balance is exaggerated, especially in advanced liver disease, due to disease-associated factors including low protein intake and anorexia.[3,4] As a result, protein-calorie malnutrition, which is a body wasting condition caused by a dietary shortage in calories and protein, in advanced liver disease increases the risks of complications and death.[3] Approximately two-thirds of patients with advanced liver disease and almost all patients waiting for liver transplantation are subject to this condition.[5] Regardless of any etiology, including alcoholic or nonalcoholic and cholestatic or noncholestatic liver disease, malnutrition can develop in patients with chronic liver disease.[6] Early screening of nutritional status and intervention in patients with chronic liver disease can reduce their risks of complications.[7] However, there are limited data related to patients with chronic liver disease requiring nutritional intervention.[8]
Branched-chain amino acids (BCAAs) are a preferential source of nitrogen for glutamate synthesis, which detoxify ammonia in the skeletal muscle as well as represent an essential substrate for the synthesis of body proteins.[9] The beneficial effects of BCAAs on protein metabolism and the nutritional state of patients with chronic liver disease are well known.[10,11] In the progression of liver cirrhosis, the depletion of BCCAs, such as leucine, isoleucine, and valine inhibits protein synthesis and protein turnover.[1,12] Moreover, the skeletal muscle catabolizes BCAAs more rapidly than most other amino acids,[13,14] and these increase the major complications of liver cirrhosis during disease progression: hepatic encephalopathy, edema, and ascites accompanied by hypoalbuminemia, insulin resistance, hepatocarcinogenesis, and infection caused by an impaired immune function.[9,15,16] Furthermore, a lower serum BCAA/aromatic-amino-acid ratio is associated with a worse prognosis in patients with advanced liver disease.[17] However, there is still little consensus on the optimal dose and duration of BCAA supplementation for chronic liver disease.
The present study investigated the long-term effectiveness of oral BCCA supplementation by analyzing the model for end-stage liver disease (MELD) score and the occurrence of complications in advanced liver disease.
2. Methods
2.1. Eligible patients
The eligibility criteria applied in this study were as follows: (1) diagnosis of liver cirrhosis documented by histology or imaging findings and confirmed by laboratory data, (2) Child–Pugh (CP) score between 8 and 10, and (3) age 18–80 years. The exclusion criteria were as follows: (1) diagnosis of malignancy (except hepatocellular carcinoma [HCC]) within the past 3 years or the presence of an untreated malignancy, (2) failure of a major organ, such as the heart, lung, or kidney, (3) being admitted or receiving medical therapy, or dialysis, (4) on a waiting list or under consideration for a major organ transplantation, (5) serum creatinine level higher than 1.5 mg/dL, (6) receiving treatment with albumin replacement regularly, (7) presence of a viable HCC tumor, advanced Barcelona Clinic Liver Cancer stage, or HCC with a life expectancy of less than 6 months, (8) persistence of alcohol consumption, (9) amyotrophic lateral sclerosis, (10) presence of another metabolic disorder presenting branched-chain ketoaciduria, (11) inability to calculate the MELD score at the time of enrollment, (12) transient impairment of liver function, or (13) treatment with a medication that affects the prothrombin time (e.g., warfarin).
2.2. Study design
This study had a multicenter, retrospective, observational, cohort design and involved 13 tertiary medical centers in South Korea. Each center was asked to recruit all patients with advanced liver cirrhosis of any etiology between January 1, 2008, and December 31, 2010. The study protocol is presented in Fig. 1. After enrollment, the patients were divided into 2 groups: treated or not treated with BCAAs. The BCAA group consumed any dose of BCAAs daily, and the control group consumed a diet without BCAA for at least 6 months. After 6 months, we analyzed the data in these 2 groups over 2 years, including the duration of BCAA medication.
Figure 1.
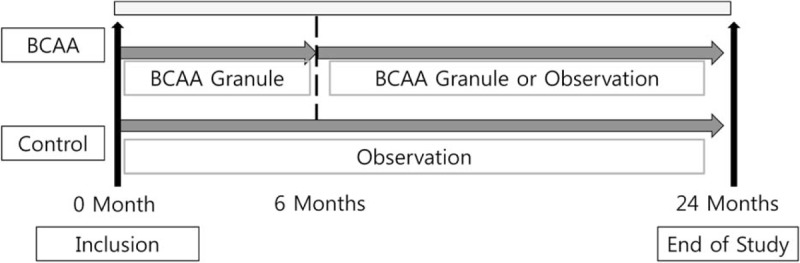
Scheme of the study design.
The primary end point of the study was the changes in the MELD score over time. The secondary end point was the changes in the CP score, incidence of HCC, survival, development of liver cirrhosis-related complications, including the development or aggravation of ascites, spontaneous bacterial peritonitis, hepatic encephalopathy, rupture of esophageal or gastric varices, hepatorenal syndrome, and development or recurrence of HCC. This study was exempt from the requirement in written informed consent because the data were analyzed anonymously. This study was approved by the institutional review board (KNUH 2012-10-024) of each center and was conducted in accordance with the principles of the Declaration of Helsinki.
2.3. Baseline assessments and follow-up
We initially performed a liver function test and evaluated the serum creatinine, viral markers of hepatitis B virus (HBV) and hepatitis C virus, prothrombin activity, CP score, MELD score, and history of cirrhotic complications, including HCC. The follow-up examinations included laboratory studies, including the serum total bilirubin, albumin, and creatinine; prothrombin activity; prognostic markers, including the CP score and MELD score; and any complications, including HCC and death.
2.4. BCAA content and compliance with BCAA treatment
Patients in the BCAA group were treated with a nutritional preparation (LIVACT, Samil Pharmaceutical Co., Ltd., Seoul, Korea; 4.15 g of BCAA granules per sachet containing 952 mg of L-iso-leucine, 1904 mg of L-leucine, and 1144 mg of L-valine). The BCAA group was divided into 3 subgroups, whose patients consumed 4.15 g, 8.3 g, or 12.45 g of BCAA granules daily. More than 80% of the patients complied with their prescribed intake of BCAA granules. Patients in the control group consumed a standard diet without BCAAs.
2.5. Statistical analysis
Data were analyzed using the IBM SPSS 20.0 (IBM Co., Armonk, NY). Baseline characteristics were compared between the 2 study groups using the chi-square test, Student's t-test, or linear-by-linear association test. Changes in the MELD score, CP score, and serum albumin between the 2 groups were analyzed using a mixed linear model. The incidence of cirrhotic complications was compared using the chi-square test. The cumulative survival and event-free survival (EFS) rates were estimated using the Kaplan–Meier method and compared using the log-rank test. Patients were counted at the loss of follow-up or death of any cause. Factors related to the incidence of HCC were analyzed using the Cox proportional-hazards model. A probability value of P < 0.05 was considered to indicate a statistical significance.
3. Results
A retrospective analysis was applied to 867 patients who met the inclusion criteria, of which 552 were excluded. The main reasons for exclusion were the presence of a viable or advanced HCC, abnormal serum creatinine level, and inability to cease alcohol consumption. Among the 315 patients, 8 patients who received medication less frequently than once a day were excluded from the analysis. Finally, a total of 307 patients (166 in the BCAA group, 141 in the control group) were analyzed (Fig. 2).
Figure 2.
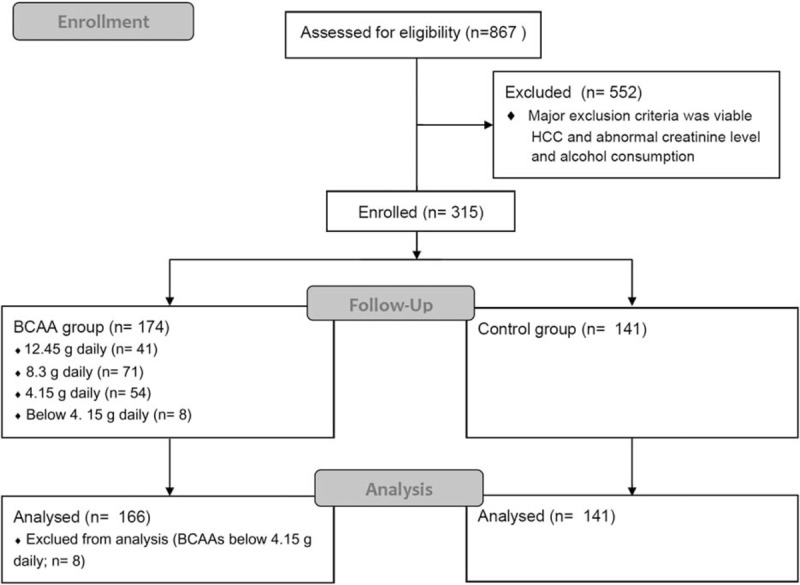
Flow diagram of the study.
There were significant differences between the BCAA and control groups in the distribution of the CP score, serum albumin level, and hepatic encephalopathy (Table 1). We attributed these differences to the physicians tending to prescribe BCAAs to patients with greater deterioration of the hepatic reservoir.
Table 1.
Baseline characteristics between control and any dose of BCAAs treated group.

3.1. Analysis of the propensity scores
In observational studies, and especially retrospective studies, the presence of a selection bias often confuses the treatment effects.[18,19] The propensity score relates to the probability of a patient receiving a specific treatment.[20] A quasi-randomized experiment can be conducted by matching the results with the propensity scores to yield an adjusted estimate of the treatment effect.[21] A logistic regression model with the covariates of sex, age, presence of varices, history of HCC, CP score, and MELD score was used to estimate the propensity scores for the BCAAs. Matching the patients who were treated with 12.45 g of BCAAs daily (n = 41) on a one-to-one basis with those in the control group resulted in the closest propensity scores. The baseline characteristics in the 2 groups are listed in Table 2. The mean follow-up duration did not differ significantly between the 2 groups (17.5 ± 6.5 months in the BCAA-12.45 g group and 17.5 ± 6.7 months in the matched control group, P = .854).
Table 2.
Baseline characteristic between 12.45 g of BCAAs treated group and unmatched control, or matched control using the propensity score.

3.2. Outcomes associated with the hepatic reservoir
Figure 3A shows the changes in the MELD scores over 2 years in the 2 study groups. The MELD scores improved significantly in the BCAA-12.45 g group over time (P = .004). Figure 3B–D shows the changes in the CP score, serum albumin level, and bilirubin level, respectively, over 2 years in the 2 groups. The serum bilirubin level (P = .014) and CP score (P = .033) also improved significantly between the 2 groups over time. However, there was no significant intergroup difference in the serum albumin level (P = .751). The subgroup analyses revealed improvements in the MELD score and serum bilirubin level in patients treated with 8.3 g of BCAAs, whereas only improvements in the serum bilirubin level were observed in the patients treated with 4.15 g of BCAAs (Table 3).
Figure 3.
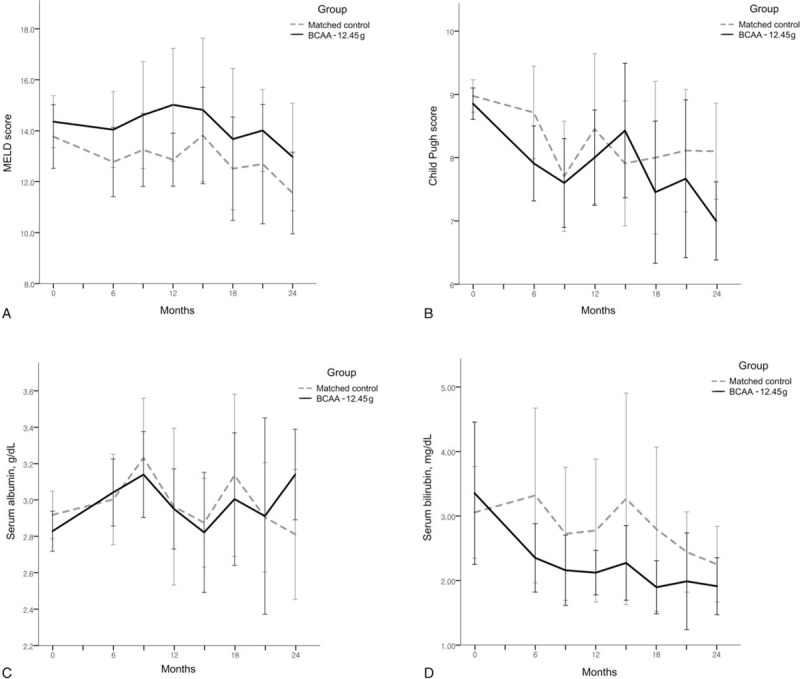
Changes in the MELD (A) and Child–Pugh (B) scores, serum albumin (C), and total bilirubin (D) in the 12.45 g branched-chain amino acid-treated group and matched control group over 2 years. MELD = model for end-stage liver disease.
Table 3.
Changes of serum albumin, total bilirubin, and prognostic marker dosages of BCAAs†.

3.3. Major cirrhotic complications and survival
The cumulative EFS curves for both study groups are shown in Fig. 4. There was no significant intergroup difference in the EFS (19.3 ± 1.2 months [mean ± SD] in the BCAA-12.45 g group and 19.2 ± 1.2 months in the matched control group, P = .973).
Figure 4.
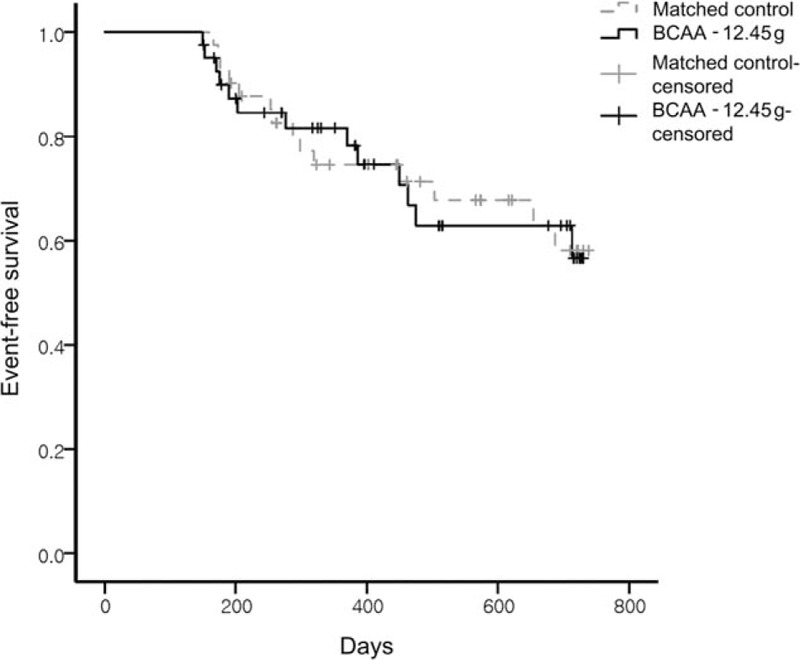
Cumulative event-free survival in the 12.45 g branched-chain amino acid-treated group and matched control group over 2 years.
Table 4 lists the major cirrhotic complications in both groups. The total events of cirrhotic complications did not differ significantly between the 2 groups (P = .814). There were also no significant intergroup differences in the following specific complications: development or aggravation of ascites, hepatic encephalopathy, hepatorenal syndrome, rupture of varices, spontaneous bacterial peritonitis, or death. HCC occurred in only 1 patient in the matched control group and 2 patients in the BCAA-12.45 g group. The cumulative HCC recurrence rate did not significantly differ between the 2 groups (P = .271, hazard ratio = 0.179; 95% confidence interval = 0.008–3.841).
Table 4.
The major cirrhotic complications in 12.45 g of BCAAs-treated group and matched control group.

4. Discussion
An exogenous protein supply was known to accelerate protein synthesis as well as inhibit proteolysis.[21,22] BCAAs, including valine, leucine, and isoleucine are indispensable amino acids and have been shown to be effective in proteolytic illnesses, such as sepsis, cancer, and trauma.[23,24] Early studies on the effectiveness of BCAA supplementation in patients with chronic liver disease focused on malnutrition and encephalopathy.[8,25] Many clinical trials have demonstrated the beneficial effects of BCAAs in patients with hepatic encephalopathy.[10,25–27] The progression of chronic liver disease is associated with the metabolism of amino acids resulting in a decreased circulating BCAA/aromatic-amino-acid ratio.[28,29] This alteration may induce hepatic encephalopathy due to elevated ammonia levels in the serum and brain.[30] There is evidence of the beneficial role of BCAAs in hepatic encephalopathy, although there are also conflicting data.[10,26,31] Two large-scale randomized controlled trials showed that long-term oral BCAA supplementation improves the clinical outcome of advanced liver cirrhosis.[3,32] These trials found that the EFS, including death due to any cause and deterioration of liver disease with or without the development of HCC, improved during oral BCAA supplementation.[3,32] The current guidelines of the European Society for Clinical Nutrition and Metabolism recommend taking a BCAA-enriched formula in case of hepatic encephalopathy during enteral nutrition.[33]
The MELD score is a well-known predictive indicator of the pretransplant waiting list death rate.[34,35] In the present study, the MELD score improved significantly over time in the patients who were treated with 12.45 g of BCAAs relative to the control group (Fig. 3A). The progression of liver cirrhosis can be slowed by other treatments, such as nucleos(t)ide analogs for treating chronic hepatitis B (CHB) or abstaining from alcohol. Therefore, nucleos(t)ide analogs might have influenced the improvements in the MELD scores in both of the present study groups. However, the number of CHB patients with a high viral load (HBV DNA > 2000 IU/mL)—and hence being treated with an antiviral agent—was only slightly higher in the matched control group than in the patients treated with 12.45 g of BCAAs (see Table, supplemental data which shows the number of CHB patients with a high viral load and their treatment). An Italian randomized, controlled, double-blind multicenter study found that long-term BCAA supplementation in patients with liver cirrhosis improved both the serum bilirubin level and CP score.[3] These results are very similar to those obtained in the present study. Decreased serum bilirubin levels may lead to improvements in the MELD score. However, in contrast to the findings in a Japanese study, we found no improvement in the serum albumin level.[32] The albumin level exhibits greater dynamic changes than the serum bilirubin level in various situations, including infection, hemorrhage, and poor nutrition. In the present study, despite the improvement in the MELD score, there were no significant intergroup differences in the EFS. This might indicate that improvements in the MELD scores have negligible effects in the presence of major cirrhotic complications.
There were no significant differences in hepatic encephalopathy between the 2 groups (Table 4). This might have been due to minimal hepatic encephalopathy being overlooked owing to the retrospective design of this study or to the duration of BCAA supplementation in the present study being shorter than those in previous studies. About 30% of the patients discontinued BCAA supplementation within 1 year; thus, the early withdrawal of BCAA supplementation seems to affect the improvement of hepatic encephalopathy.[10]
In the subgroup analysis of the entire BCAA group treated with BCAAs, the CP score did not improve in patients treated with < 12.45 g of BCAAs. In patients treated with 4.15 g of BCAAs, only marginal effects were found (Table 3). These observations imply that optimizing the dose of BCAA supplementation is important for maximizing the beneficial effects. A large-scale prospective study is needed for optimizing the dose of BCAA supplementation in patients with liver cirrhosis.
Few studies have evaluated the anticarcinogenic effects of BCAAs in patients with liver cirrhosis.[36–38] The anticarcinogenic effect of BCAA supplementation could be due to improvements in insulin resistance, whereas its antiangiogenic effect could be due to the inhibition of the vascular endothelial growth factor.[9,39,40] A Japanese study found that the incidence of HCC decreased in specific populations, such as in patients with chronic hepatitis C (CHC) or in those with a body mass index (BMI) of ≥ 25 kg/m2. However, the etiology of liver cirrhosis in Korea differs from that in Japan. In the present study, CHB and alcoholic liver cirrhosis were more common than CHC. Further, a subgroup analysis of the effects of a BMI of ≥ 25 kg/m2 could not be performed owing to the small number of patients.
Our study was subject to several limitations. First, the guideline for using BCAA supplementation varied among the included centers. However, after adjustments based on the propensity scores, differences in the baseline characteristics disappeared between the 2 study groups. Second, the number of patients treated with 12.45 g of BCAAs was smaller in this study than in previous studies owing to the high cost or poor palatability of the particular BCAA granules used. Third, although significant improvements in the MELD scores were demonstrated in patients treated with BCAAs, there were no improvements in the clinical outcomes in this study. To improve the clinical outcomes, further evaluation of the optimal duration and indication of BCAA supplementation would be needed considering the disease stage and degree of malnutrition. Fourth, the retrospective design of this study meant that the follow-up interval varied among the patients and their dietary habits were not tracked. A further large-scale prospective study would be needed to delineate the efficacy of oral BCAAs and overcome these limitations.
This study has demonstrated that the MELD score improves during treatment with long-term oral BCAA supplementation in advanced liver disease. The efficacy of BCAA supplementation varies with the dosing regimen; thus, it is important to determine how to maximize the effectiveness of BCAAs in chronic liver disease.
5. Conclusion
Long-term oral BCAA supplementation has beneficial effects on prognostic markers in patients with advanced liver cirrhosis. A sufficient dosage of oral BCAA supplementation would be needed to increase its beneficial effects.
Supplementary Material
Footnotes
Abbreviations: BCAAs = branched-chain amino acids, BMI = body mass index, CHB = chronic hepatitis B, CHC = chronic hepatitis C, CP = Child–Pugh, EFS = event-free survival, HBV = hepatitis B virus, HCC = hepatocellular carcinoma, MELD = model for end-stage liver disease.
Authorship: WYT and JGP is guarantor of integrity of the entire study. SYP, WYT, and YOK designed the study. JGP, SHB, JYJ, DYK, JSL, KTS, IHK, HJL, WJC, BKJ, JIS, and JH collected data, which was analyzed by GJP and WKL based on the statistical analysis plan. GJP drafted the manuscript, which was critically revised by WYT, SYP, SYJ, and YRL. This manuscript does not contain any previously published material and will not be submitted for publication elsewhere.
Funding: This work was supported by Samil Pharmaceutical Co., Ltd.
The authors have no conflicts of interest to disclose.
Supplemental Digital Content is available for this article.
References
- [1].Swart GR, van den Berg JW, Wattimena JL, et al. Elevated protein requirements in cirrhosis of the liver investigated by whole body protein turnover studies. Clin Sci (Lond) 1988;75:101–7. [DOI] [PubMed] [Google Scholar]
- [2].Mullen KD, Denne SC, McCullough AJ, et al. Leucine metabolism in stable cirrhosis. Hepatology 1986;6:622–30. [DOI] [PubMed] [Google Scholar]
- [3].Marchesini G, Bianchi G, Merli M, et al. Nutritional supplementation with branched-chain amino acids in advanced cirrhosis: a double-blind, randomized trial. Gastroenterology 2003;124:1792–801. [DOI] [PubMed] [Google Scholar]
- [4].Laviano A, Cangiano C, Preziosa I, et al. Plasma tryptophan levels and anorexia in liver cirrhosis. Int J Eat Disord 1997;21:181–6. [DOI] [PubMed] [Google Scholar]
- [5].Henkel AS, Buchman AL. Nutritional support in patients with chronic liver disease. Nat Clin Pract Gastroenterol Hepatol 2006;3:202–9. [DOI] [PubMed] [Google Scholar]
- [6].McCullough AJ, Bugianesi E. Protein-calorie malnutrition and the etiology of cirrhosis. Am J Gastroenterol 1997;92:734–8. [PubMed] [Google Scholar]
- [7].Kondrup J, Allison SP, Elia M, et al. ESPEN guidelines for nutrition screening 2002. Clin Nutr 2003;22:415–21. [DOI] [PubMed] [Google Scholar]
- [8].Alberino F, Gatta A, Amodio P, et al. Nutrition and survival in patients with liver cirrhosis. Nutrition 2001;17:445–50. [DOI] [PubMed] [Google Scholar]
- [9].Kawaguchi T, Izumi N, Charlton MR, et al. Branched-chain amino acids as pharmacological nutrients in chronic liver disease. Hepatology 2011;54:1063–70. [DOI] [PubMed] [Google Scholar]
- [10].Khanna S, Gopalan S. Role of branched-chain amino acids in liver disease: the evidence for and against. Curr Opin Clin Nutr Metab Care 2007;10:297–303. [DOI] [PubMed] [Google Scholar]
- [11].Bianchi G, Marzocchi R, Agostini F, et al. Update on branched-chain amino acid supplementation in liver diseases. Curr Opin Gastroenterol 2005;21:197–200. [DOI] [PubMed] [Google Scholar]
- [12].Yoshizawa F. Regulation of protein synthesis by branched-chain amino acids in vivo. Biochem Biophys Res Commun 2004;313:417–22. [DOI] [PubMed] [Google Scholar]
- [13].Kimball SR, Jefferson LS. Regulation of protein synthesis by branched-chain amino acids. Curr Opin Clin Nutr Metab Care 2001;4:39–43. [DOI] [PubMed] [Google Scholar]
- [14].Tischler ME, Desautels M, Goldberg AL, et al. leucyl-tRNA, or some metabolite of leucine regulate protein synthesis and degradation in skeletal and cardiac muscle? J Biol Chem 1982;257:1613–21. [PubMed] [Google Scholar]
- [15].Freund HR, Hanani M. The metabolic role of branched-chain amino acids. Nutrition 2002;18:287–8. [DOI] [PubMed] [Google Scholar]
- [16].Nakamura I, Ochiai K, Imai Y, et al. Restoration of innate host defense responses by oral supplementation of branched-chain amino acids in decompensated cirrhotic patients. Hepatol Res 2007;37:1062–7. [DOI] [PubMed] [Google Scholar]
- [17].Morgan MY, Milsom JP, Sherlock S. Plasma ratio of valine, leucine and isoleucine to phenylalanine and tyrosine in liver disease. Gut 1978;19:1068–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [18].Austin PC. An introduction to propensity score methods for reducing the effects of confounding in observational studies. Multivariate Behav Res 2011;46:399–424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Austin PC. A critical appraisal of propensity-score matching in the medical literature between 1996 and 2003. Stat Med 2008;27:2037–49. [DOI] [PubMed] [Google Scholar]
- [20].D’Agostino RB., Jr Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med 1998;17:2265–81. [DOI] [PubMed] [Google Scholar]
- [21].Leweling H, Breitkreutz R, Behne F, et al. Hyperammonemia-induced depletion of glutamate and branched-chain amino acids in muscle and plasma. J Hepatol 1996;25:756–62. [DOI] [PubMed] [Google Scholar]
- [22].Harris RA, Joshi M, Jeoung NH. Mechanisms responsible for regulation of branched-chain amino acid catabolism. Biochem Biophys Res Commun 2004;313:391–6. [DOI] [PubMed] [Google Scholar]
- [23].De Bandt JP, Cynober L. Therapeutic use of branched-chain amino acids in burn, trauma, and sepsis. J Nutr 2006;136:308S–13S. [DOI] [PubMed] [Google Scholar]
- [24].Choudry HA, Pan M, Karinch AM, et al. Branched-chain amino acid-enriched nutritional support in surgical and cancer patients. J Nutr 2006;136:314S–8S. [DOI] [PubMed] [Google Scholar]
- [25].Rossi Fanelli F, Cangiano C, Capocaccia L, et al. Use of branched chain amino acids for treating hepatic encephalopathy: clinical experiences. Gut 1986;27Suppl 1:111–5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Les I, Doval E, Garcia-Martinez R, et al. Effects of branched-chain amino acids supplementation in patients with cirrhosis and a previous episode of hepatic encephalopathy: a randomized study. Am J Gastroenterol 2011;106:1081–8. [DOI] [PubMed] [Google Scholar]
- [27].Gluud LL, Dam G, Borre M, et al. Oral branched-chain amino acids have a beneficial effect on manifestations of hepatic encephalopathy in a systematic review with meta-analyses of randomized controlled trials. J Nutr 2013;143:1263–8. [DOI] [PubMed] [Google Scholar]
- [28].Blonde-Cynober F, Aussel C, Cynober L. Abnormalities in branched-chain amino acid metabolism in cirrhosis: influence of hormonal and nutritional factors and directions for future research. Clin Nutr 1999;18:5–13. [DOI] [PubMed] [Google Scholar]
- [29].Charlton M. Branched-chain amino acid enriched supplements as therapy for liver disease. J Nutr 2006;136:295S–8S. [DOI] [PubMed] [Google Scholar]
- [30].Holecek M. Three targets of branched-chain amino acid supplementation in the treatment of liver disease. Nutrition 2010;26:482–90. [DOI] [PubMed] [Google Scholar]
- [31].James JH. Branched chain amino acids in heptatic encephalopathy. Am J Surg 2002;183:424–9. [DOI] [PubMed] [Google Scholar]
- [32].Muto Y, Sato S, Watanabe A, et al. Effects of oral branched-chain amino acid granules on event-free survival in patients with liver cirrhosis. Clin Gastroenterol Hepatol 2005;3:705–13. [DOI] [PubMed] [Google Scholar]
- [33].Plauth M, Cabre E, Riggio O, et al. ESPEN guidelines on enteral nutrition: liver disease. Clin Nutr 2006;25:285–94. [DOI] [PubMed] [Google Scholar]
- [34].Kamath PS, Wiesner RH, Malinchoc M, et al. A model to predict survival in patients with end-stage liver disease. Hepatology 2001;33:464–70. [DOI] [PubMed] [Google Scholar]
- [35].Kamath PS, Kim WR. Advanced Liver Disease Study Group. The model for end-stage liver disease (MELD). Hepatology 2007;45:797–805. [DOI] [PubMed] [Google Scholar]
- [36].Muto Y, Sato S, Watanabe A, et al. Overweight and obesity increase the risk for liver cancer in patients with liver cirrhosis and long-term oral supplementation with branched-chain amino acid granules inhibits liver carcinogenesis in heavier patients with liver cirrhosis. Hepatol Res 2006;35:204–14. [DOI] [PubMed] [Google Scholar]
- [37].Kobayashi M, Ikeda K, Arase Y, et al. Inhibitory effect of branched-chain amino acid granules on progression of compensated liver cirrhosis due to hepatitis C virus. J Gastroenterol 2008;43:63–70. [DOI] [PubMed] [Google Scholar]
- [38].Hayaishi S, Chung H, Kudo M, et al. Oral branched-chain amino acid granules reduce the incidence of hepatocellular carcinoma and improve event-free survival in patients with liver cirrhosis. Dig Dis 2011;29:326–32. [DOI] [PubMed] [Google Scholar]
- [39].Iwasa J, Shimizu M, Shiraki M, et al. Dietary supplementation with branched-chain amino acids suppresses diethylnitrosamine-induced liver tumorigenesis in obese and diabetic C57BL/KsJ-db/db mice. Cancer Sci 2010;101:460–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [40].Yoshiji H, Noguchi R, Kaji K, et al. Attenuation of insulin-resistance-based hepatocarcinogenesis and angiogenesis by combined treatment with branched-chain amino acids and angiotensin-converting enzyme inhibitor in obese diabetic rats. J Gastroenterol 2010;45:443–50. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.