

Abstract
Purpose
To systematically study the number of U.S. resident deaths from all causes, including suicide.
Method
The more than 9,900 programs accredited by the Accreditation Council for Graduate Medical Education (ACGME) annually report the status of residents. The authors aggregated ACGME data on 381,614 residents in training during years 2000 through 2014. Names of residents reported as deceased were submitted to the National Death Index to learn causes of death. Person-year calculations were used to establish resident death rates and compare them with those in the general population.
Results
Between 2000 and 2014, 324 individuals (220 men, 104 women) died while in residency. The leading cause of death was neoplastic disease, followed by suicide, accidents, and other diseases. For male residents the leading cause was suicide, and for female residents, malignancies. Resident death rates were lower than in the age- and gender-matched general population. Temporal patterns showed higher rates of death early in residency. Deaths by suicide were higher early in training, and during the first and third quarters of the academic year. There was no upward or downward trend in resident deaths over the 15 years of this study.
Conclusions
Neoplastic disease and suicide were the leading causes of death in residents. Data for death by suicide suggest added risk early in residency and during certain months of the academic year. Providing trainees with a supportive environment and with medical and mental health services is integral to reducing preventable deaths and fostering a healthy physician workforce.
In 2014, the suicide-related deaths of two internal medicine interns in New York1 shocked the public and the profession, and refocused attention on physician suicide, a concern for several decades. A study by Center et al2 found that an estimated 300 to 400 practicing physicians died by suicide each year, and another by Shanafelt et al3 showed that 1 in 16 surgeons reported suicidal ideation. Studies also show that medical residents are at higher risk for depressive disorders, depressed mood, burnout, and suicidal ideation than are their peers in the general population.4–6 However, the causes of death for physicians in training have not been systematically studied.
The Accreditation Council for Graduate Medical Education (ACGME) accredits more than 9,900 residency and fellowship programs across the United States7 and oversees the training of approximately 125,000 residents annually.7 Each preventable resident death, in addition to being a tragedy for colleagues, faculty, and patients, represents a real loss to patients and society, given the estimated 30,000-hour contribution of a physician over the course of a full career.
Our study sought to better understand the rates and causes of death for residents, and compare them with rates in the general population. In particular, we were interested in the number and leading causes of resident deaths; their patterns and trends in occurrence; and associations with gender, year in training, program accreditation status, and whether any patterns could offer information to reduce avoidable deaths.
Method
The ACGME maintains information about U.S. accredited graduate medical education programs, including the number of residents enrolled in a given program for each academic year.7 Programs annually update their information using the Accreditation Data System (ADS). Data about new residents are entered, residents continuing in the program are confirmed, and residents who have graduated or left the program are identified. For each resident no longer in the program, the reason is selected from a list that includes indicating the resident is deceased.
Our study used data aggregated by the National Death Index (NDI), a division of the National Center for Health Statistics. The American Institute for Research Review Board reviewed our study protocol and issued an exempt designation following an expedited review. We queried the NDI, in compliance with published guidelines,8 to provide the cause of death for residents reported as deceased. NDI staff matched resident information with cause of death data from their database, and provided ICD-10-coded causes of death.
We matched the cause of death information from the NDI with demographic data from the ADS database to determine cause-of-death differences by gender, specialty, level of training, and academic year. Cross-tab comparisons and odds ratio (OR) calculations were performed with SAS Enterprise Guide, Version 7.1 (SAS, Cary, North Carolina).
We calculated estimated person-years by summing the number of persons (in this case, residents) for each academic year whose data we studied. For example, in academic year 2007–2008, there were 107,851 residents in ACGME programs; thus, there were 107,851 person-years in 2007–2008. To create the study window of 15 years, 2000 through 2014, we used half the total number of person-years for academic years 1999–2000 and 2014–2015. Because ADS annual reporting was not fully operational during 1999–2000 and 2000–2001, we used data from the American Medical Association Graduate Medical Education Census published in the JAMA medical education theme issues of 20009 and 2001.10 We calculated person-years for men and for women for each individual year of training that we studied. This enabled comparisons of resident rates of death per 100,000 person-years to age- and gender-matched U.S. cohorts, reported for the overall cohort, and by gender and year of training for the 15-year period of analysis.
Lastly, we examined whether there were differences in accreditation status and/or other accreditation parameters for programs with one or more resident suicides, those with one or more resident deaths due to other causes, and programs overall, on the hypothesis that resident stress may be higher in programs that are not well managed.
Results
From 2000 through 2014, 381,614 individual physicians were enrolled in ACGME-accredited residency programs and participated in 1,622,939 collective person-years of training (918,654 years for men, 704,285 years for women). Over the same period, 324 residents were reported as having died while enrolled in ACGME-accredited programs.
Through the NDI and other public sources, the cause of death was identified for 311 individuals (96%). Of the 324 deceased trainees, 305 (94%) were accurately matched to the cause of death using NDI data, and for another 6 trainees (2%), the cause of death was determined from obituaries or local news articles. The cause of death of the remaining 13 could not be precisely identified and was categorized as “ill-defined or of undetermined intent.”
For the study period, the general category representing the highest number of deaths among residents (80; 42 men, 38 women) was neoplastic diseases, with central nervous system (15; 7 men, 8 women) and breast cancer (12 women, no men) the most prevalent causes (see Table 1). The second-most-prevalent cause of resident death was suicide (66; 51 men, 15 women), with 16 residents dying using firearms, and 16 intentionally overdosing on drugs or other substances. Suicide by leaping from heights or by asphyxia by hanging, strangulation, or inhalation accounted for 18 deaths, and 16 residents died by suicide by other means or by unspecified means.
Table 1.
Causes of Death of Residents From 2000 Through 2014: Frequency and Rate per 100,000 Person-Years, by Resident Gender and Age Rangea,b
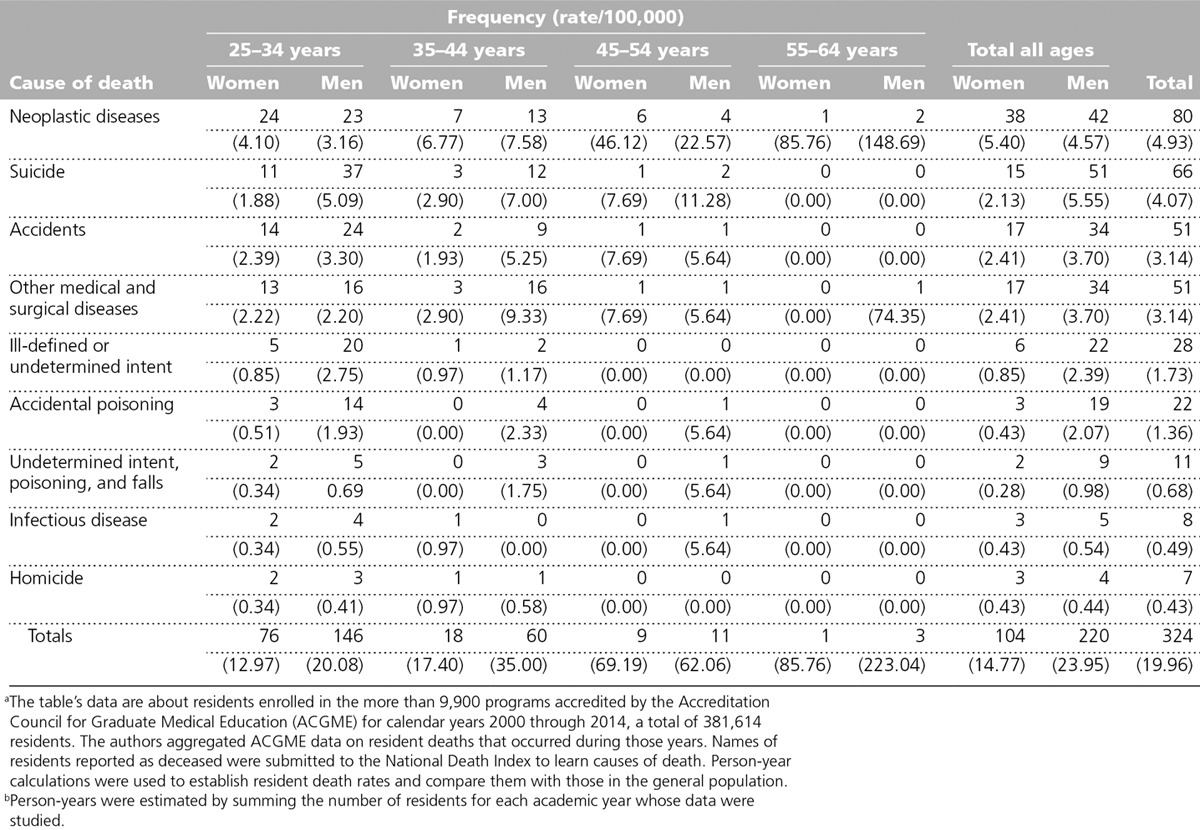
Fifty-one residents died from being involved in accidents (34 men, 17 women). Among these deaths, 33 (20 men, 13 women) were classified as motor vehicle accidents, and 5 (4 men, 1 woman) were classified as pedestrian or bicycle accidents. Another 51 residents succumbed to medical and surgical diseases. Among these deaths, 30 (22 men, 8 women) resulted from cardiovascular disease, and 8 (5 men, 3 women) were from infectious diseases.
Twenty-two residents (19 men, 3 women), including 12 anesthesiology residents, died by accidental poisoning. The deaths of an additional 11 residents (9 men, 2 women) occurred under circumstances of unclear intent (5 of these deaths by falls and 6 by poisoning), and 7 residents (4 men, 3 women) were victims of homicide. For 28 residents (22 men, 6 women)—including 13 residents that could not be matched to NDI or public data, and 15 with NDI records—the cause of death was classified as ill-defined or undetermined intent.
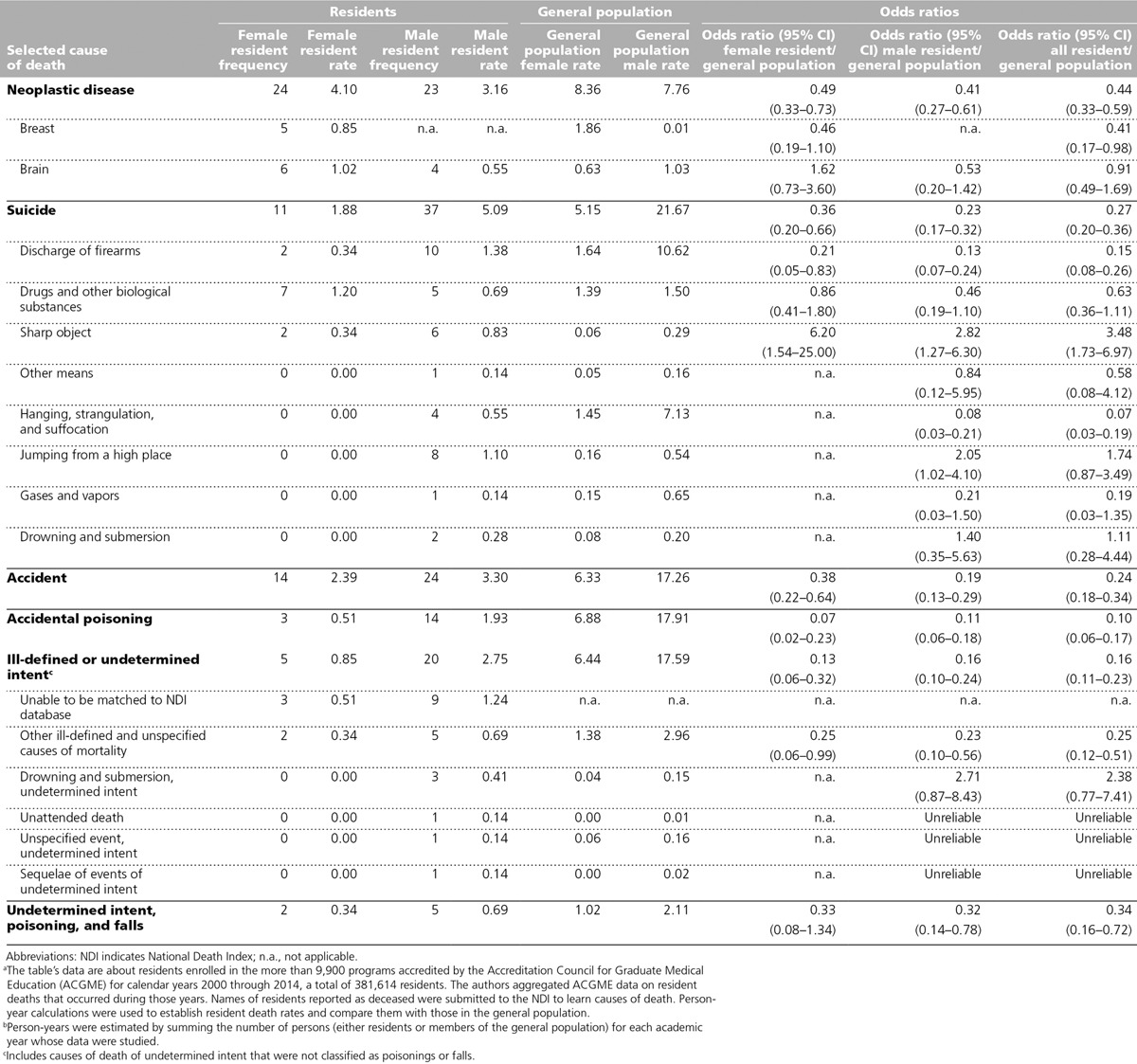
Between 2000 and 2014, the reported and published overall death rate for 25- to 34-year-olds in the U.S. general population was 105.4 per 100,000 population (145.3 men, 65.0 women).11 Over the 15 years of this study, the death rate of male residents ages 25–34 years was much lower at 20.08 per 100,000 (OR 0.14, confidence interval [CI] 0.11–0.16), and for female residents ages 25–34 it was 12.97 per 100,000 (OR 0.20, CI 0.15–0.24), for an aggregate death rate for residents ages 25–34 of 16.91 (OR 0.16, CI 0.14–0.18). The specific frequencies and rates of causes of death are shown in Table 1, and comparisons with the gender- and age-matched parameters of the U.S. population are provided in Table 2.
Table 2.
Selected Causes of Death of Residents 25–34 Years Old and of Members of the General Population in the Same Age Group, From 2000 Through 2014: Frequency (for Residents) and Rate (for Both Groups) per 100,000 Person-Years, by Gendera,b
Suicide is the leading cause of death in male residents, and the second-most-prevalent for female residents (see Table 1). An important finding is that the majority of suicides (49 of 66; 74%) occurred in years 1 and 2 of training (see Figure 1). In addition, the months of July–September and January–March (the first and third quarters of each academic year) contain 42 of the 66 (64%) resident suicides, with the first quarter containing 23 (almost 35%).
Figure 1.
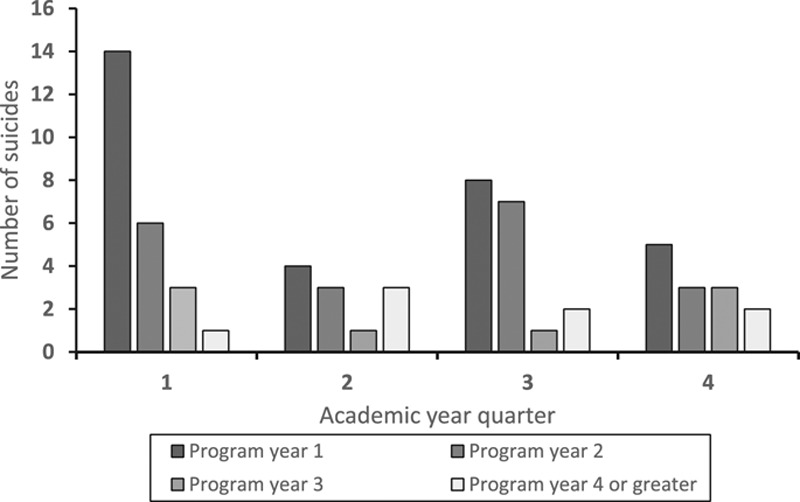
Number of resident suicides by academic year, quarter, and residency program year. The figure uses data about residents enrolled in the more than 9,900 programs accredited by the Accreditation Council for Graduate Medical Education (ACGME) during the years 2000 through 2014, a total of 381,614 residents. The authors aggregated ACGME data on resident deaths that occurred during those years.
Whereas residents as a group were less likely to die by suicide than the members of the general population as a group (see Table 2), residents in the age cohorts 35–44 and 45–54 had higher rates of suicide than did those in the 25–34 cohort, and the 95% CIs of the ORs for these groups exceed the rate of the general population. Gender-related trends are present as well. The suicide rate for male residents of 5.55 is 2.61 times higher than the rate for female residents of 2.13. However, the male resident OR for deaths by suicide in comparison with males in the general population aged 25–34 is 0.24, while the female resident to population aged 25–34 is 0.38, nearly 50% greater than that for males.11
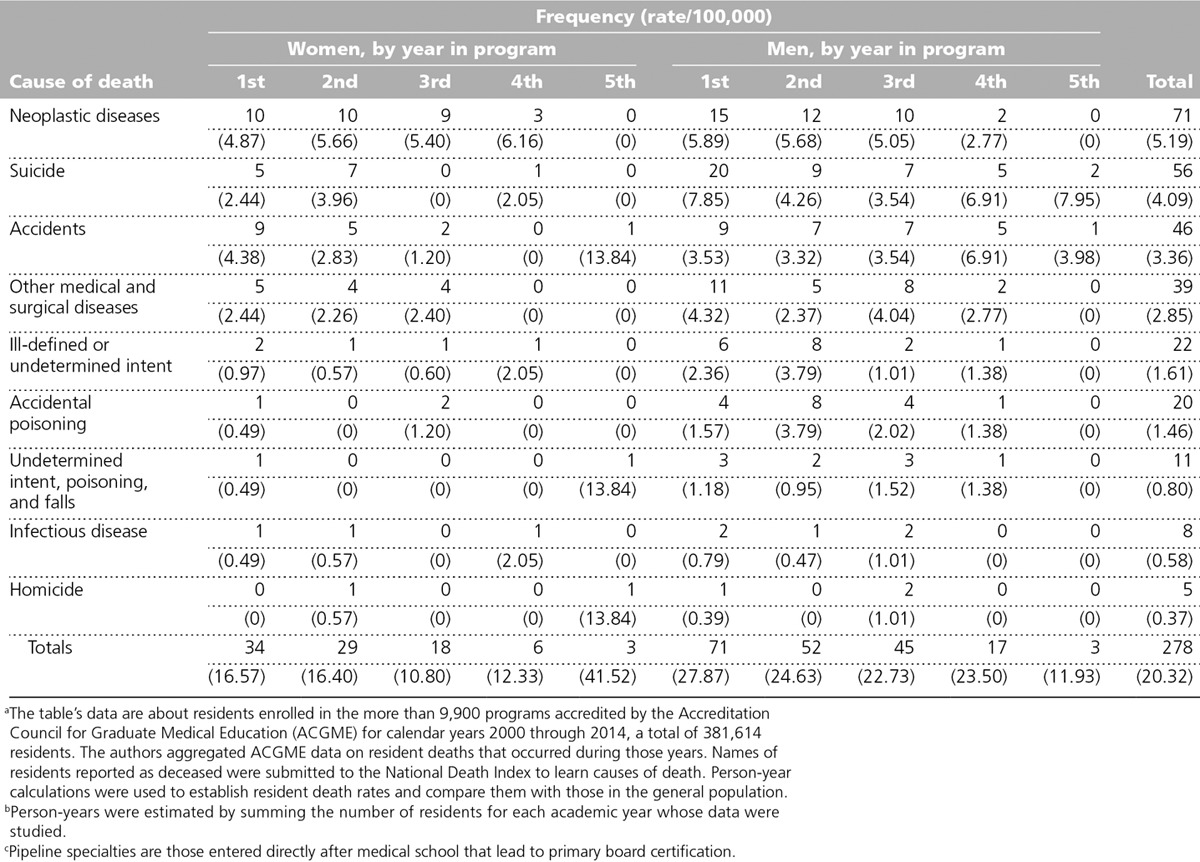
Table 3 shows patterns in death by year for training for pipeline specialties (i.e., specialties entered directly after medical school that lead to primary board certification; nonpipeline specialties are those in fellowship programs entered after completion of a pipeline specialty program). Other than the data for suicide, there are no patterns that provide actionable information to reduce preventable deaths. For neoplastic disease, which was the most common cause of death during the study period, a higher number of deaths occurred in the first year of training, yet the calculated rates do not suggest any significant differences across years of training. Information for the 46 physicians in nonpipeline specialties shows “other medical and surgical diseases” as the most common cause of death (12), followed by suicide (10) and neoplastic disease (9); these data are not shown in Table 3.
Table 3.
Causes of Deaths of Residents Who Were Training in Pipeline Specialties, From 2000 Through 2014: Frequency and Rate per 100,000 Person-Years, by Resident Gender and Year in Programa,b,c
Residents who died during the time period we studied were training in 49 specialties or subspecialties. During the same time period, deaths of graduates from Canadian medical schools (3; 0.9%), international medical schools (88; 27%), U.S. MD-granting medical schools (201; 62%), and DO-granting medical schools (25; 7.7%) approximate the proportions of matriculated residents in ACGME-accredited programs.12
Analysis of the relationship between the accreditation status of programs and resident deaths showed that at the time of the resident deaths, there were no significant differences between the accreditation status of programs with resident deaths and those without them (chi-square = 3.3087, P = .3464). Review of the resident surveys from the programs with resident suicides compared with programs with resident deaths from other causes revealed no differences in duty hours compliance, institutional or faculty resources, or resident satisfaction with their program (data not shown in the table).
Resident deaths per year varied from a minimum of 13 in 2000–2001 to a maximum of 31 in 2007–2008 (mean 22.36, mode 18, SD 4.78; detailed data not shown in the table). There was no trend (increasing or decreasing) in total deaths, or deaths from any common causes for the 15 academic years in this analysis, which include the implementation of common work hours standards in 2003 and 2011.
Discussion
We are aware of only two prior national, multispecialty reports of resident mortality, with both using a more limited sample and finding low rates of death.13,14 Both studies used surveys of program directors, which may have resulted in underreporting. In this comprehensive study of nearly 400,000 resident physicians, covering over 1.6 million person-years over 15 years, we observed 324 deaths. This corresponds to an overall death rate of 19.96 per 100,000 person-years (23.95 men; 14.77 women), and a death rate from suicide for residents of 4.07 per 100,000 person-years (5.56 men; 2.13 women), compared with 13.07 suicides per 100,000 years for the general population aged 25–34.9 Both the overall rate of resident deaths and the rates for common causes of resident deaths are notably lower than the corresponding rates for the general population.
The epidemiological surveillance nature of the data limits our ability to make further evidence-based recommendations to reduce preventable deaths from many common causes. For example, data for resident deaths in motor vehicle accidents would be of interest, given concerns about resident fatigue and increased risk for accidents.15 The favorable comparisons with the age- and gender-matched population (2.39 vs. 6.33 per 100,000 person-years for female residents, and 3.33 vs. 17.26 per 100,000 person-years for male residents; see Table 2) offer reassurance that residents die in motor vehicle accidents at rates lower than the general population. At the same time, the data lack information on the timing and context of accidents, which makes it impossible to assess whether any of these deaths resulted from potentially preventable causes.
Our data indicate that neoplastic disease is the most prevalent cause of death of residents, and the leading cause of death in female residents. Although residents are less likely to die of malignancy than their age- and gender-matched cohorts, resident deaths from malignancy occur throughout training, suggesting that some residents matriculate into graduate training with potentially undiagnosed disease, and others develop the disease while in training. This suggests that supporting resident self-care, including opportunities for preventive health care, is essential, if programs and sponsoring institutions are to minimize preventable deaths from malignancy. As noted by Legha16 in a history of physician suicide—yet applicable to other causes of resident deaths—if a member of a health profession can become ill and not seek or receive care, “despite being surrounded by other caregivers, [that] begs for a thoughtful assessment to determine why it happens at all.” There are few studies of resident access and use of health care services. One study from 2000 found barriers to resident use of health services, due to residents’ long hours and multiple competing obligations.17
The finding of lower rates of resident death by suicide compared with the age- and gender-matched population was surprising, given the data on higher rates of depression in medical students than in the age-matched general population,18 and the higher rates of suicide deaths in practicing physicians compared with the rates in the general population. The exceptions to this are residents in age cohorts 35–44 and 45–54, for which the 95% CIs of the ORs exceeded the rate of the general population. Despite the lower rate, of all major causes of death during residency, only death by suicide showed potentially actionable patterns. The higher rates of suicide for residents early in their training are consistent with data from a prospective study of 740 interns at 13 institutions, finding that suicidal ideation increased 370% over the first three months of the first year of training.19 Higher rates early in training, and during the first and third quarters of the academic year, are consistent with the hypothesis that the stresses of the transition from medical school to residency, and from intern to resident, are significant and may contribute to risk in susceptible individuals. Similarly, postholiday midwinter, midyear academic, and seasonal factors may have particularly severe effects on some residents, possibly leading to depression, isolation, and even suicide. It is possible that some suicide deaths were attributed to other causes, due to pressure from, for example, decedents’ families, colleagues, or faculty. If some of the accidental deaths, some of the surprisingly high rate of poisonings, and some of the deaths with ill-defined causes or undetermined intent were misclassified suicides, the number would be higher than the 66 declared suicides.
Our findings present the education community with an opportunity to reduce unnecessary deaths by increasing preventive strategies, scheduling preemptive education, and fostering access to counseling and confidential mental health services for residents. In addition, all of those who are engaged in the clinical learning environment—both faculty and residents themselves—need to watch for signs of resident burnout, depression, social isolation, or significant changes in performance.
Practical interventions to enhance well-being are beginning to result from efforts by the ACGME and the graduate medical education community to aggregate relevant resources, including an enhanced focus on resident well-being through a range of ACGME activities.20 That such programs can be created and used by residents and faculty, and show positive impact, has been demonstrated for the past decade by the experience at Oregon Health and Science University,21 and a controlled trial that showed that cognitive behavior therapy significantly reduced suicidal ideation.22
At the same time, supporting trainee well-being and help-seeking behaviors will not eliminate resident deaths by suicide, as rates are already low, and, often, there is a lack of any advance warning.23 Future studies should explore institution- and program-level approaches to increase and support help-seeking behaviors by trainees in distress, through a supportive community, and engagement of faculty, peers, and family and social networks.
In contrast to physicians in training, practicing physicians die by suicide at rates greater than those for age- and gender-matched professional and general populations,24–26 and the prevalence of physician burnout and depression appears to be increasing in practicing physicians27 and in residents.16 A systematic review4 found a rate of 29% of depression and/or depressive symptoms across studies, ranging from 21% to 43%, with higher rates in more recent studies. The link between burnout and suicidal ideation is complex, yet there is a link. A study showed that 27% of medical students who met criteria for burnout during their undergraduate medical education recovered, and that individuals who recovered reported markedly less suicidal ideation, suggesting lower risk for burnout.28
The well-being of physicians is important to patients, the profession, the public, and the physicians themselves.29,30 Disturbances in their well-being can have serious consequences for their patients and loved ones, while disturbances in the well-being of a sizable portion of the physician workforce may have a detrimental effect on the profession’s commitment to serving society.24 Efforts to enhance physician well-being must begin during the medical education years, and strategic interventions to initiate habits of self-care and improve use of mental and physical health care should target residents and faculty.21,31 Inclusion of the latter group is important for their well-being, and to promote these behaviors on the part of those who serve as role models for residents. Improved physician well-being will benefit patients, as a meta-analysis has found positive associations of occupational well-being and patient satisfaction, patient adherence to treatment, and interpersonal aspects of care.28
Limitations and strengths
There are limitations to this study. First, despite the magnitude of the cohort, it does not represent all residents in the United States. The American Osteopathic Association accredits osteopathic programs, and a number of surgical fellowship programs are accredited by specialty societies or other entities. Also, our study did not assess the prevalence of suicide after dismissal from, or completion of, residency. Finally, the limited number of deaths from specific causes, including suicide deaths, and absence of individual resident data beyond demographic information, precluded the use of regression analysis to provide a more sophisticated assessment of risk factors. Strengths of this study include that it is the most complete study of causes of resident death to date, covering 15 academic years of ACGME-accredited programs and involving nearly 400,000 physicians in training, with the causes of death obtained through the NDI database or other public sources of information.
Conclusions
Resident death occurs significantly less frequently than in the age- and gender-matched general population. Malignancy is the most common cause, with suicide the second-most prevalent etiology and the most preventable cause of death of trainees. The data suggest a higher risk for individuals early in their training and during vulnerable periods in the first quarter of the academic year and after the winter holiday season. Strategies to reduce preventable deaths should include preventive and treatment services, emergency support for trainees in distress, and ongoing monitoring and provision of wellness services that take into account the level of training, age of the trainee, and the time of year. Future research should explore institution- and program-level approaches to increase and support help-seeking behaviors by trainees in distress.
Acknowledgments: The authors would like to thank the staff at the National Death Index for their timely handling of the submission and matching data. The authors would also like to thank Laura Emory, John Anders Voss, and Peyman Adeli Sardo, MD, for their aid in reviewing the literature.
Footnotes
Funding/Support: This project was fully funded by the Accreditation Council for Graduate Medical Education (ACGME).
Other disclosures: All of the authors are paid employees of the ACGME.
Ethical approval: This study was deemed exempt from human subjects review by the American Institute for Research on August 22, 2015, following an expedited review.
References
- 1.Sinha P. Why do doctors commit suicide? N Y Times. September 4 2014. http://www.nytimes.com/2014/09/05/opinion/why-do-doctors-commit-suicide.html?_r=0. Accessed March 5, 2017. [Google Scholar]
- 2.Center C, Davis M, Detre T, et al. Confronting depression and suicide in physicians: A consensus statement. JAMA. 2003;289:3161–3166.. [DOI] [PubMed] [Google Scholar]
- 3.Shanafelt TD, Balch CM, Dyrbye L, et al. Special report: Suicidal ideation among American surgeons. Arch Surg. 2011;146:54–62.. [DOI] [PubMed] [Google Scholar]
- 4.Mata DA, Ramos MA, Bansal N, et al. Prevalence of depression and depressive symptoms among resident physicians: A systematic review and meta-analysis. JAMA. 2015;314:2373–2383.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Bellini LM, Baime M, Shea JA. Variation of mood and empathy during internship. JAMA. 2002;287:3143–3146.. [DOI] [PubMed] [Google Scholar]
- 6.Dyrbye LN, West CP, Satele D, et al. Burnout among U.S. medical students, residents, and early career physicians relative to the general U.S. population. Acad Med. 2014;89:443–451.. [DOI] [PubMed] [Google Scholar]
- 7.ACGME Data Resource Book, 2014–2015. http://www.acgme.org/About-Us/Publications-and-Resources/Graduate-Medical-Education-Data-Resource-Book. Accessed March 5, 2017.
- 8.U.S. Department of Health and Human Services, Centers for Disease Control and Prevention. National Death Index Users Guide. http://www.cdc.gov/nchs/data/ndi/ndi_users_guide.pdf. Accessed March 5, 2017.
- 9.Brotherton SE, Simon FA, Tomany SC. U.S. graduate medical education, 1999–2000. Graduate medical education. Appendix II, Table 1. JAMA. 2000;284:1159–1160.. [DOI] [PubMed] [Google Scholar]
- 10.Brotherton SE, Simon FA, Etzel SI. U.S. graduate medical education, 2000–2001. Graduate medical education. Appendix II, Table 1. JAMA. 2001;286:1095–1096.. [DOI] [PubMed] [Google Scholar]
- 11.Centers for Disease Control and Prevention, National Center for Health Statistics. About underlying cause of death 1999–2015. http://wonder.cdc.gov/ucd-icd10.html. Accessed March 5, 2017.
- 12.Accreditation Council for Graduate Medical Education. Academic year 2014–2105. Figure c.14. Number of active residents, by medical school type and academic year, 2006–2007 to 2015–2016. In: ACGME Data Resource Book. 2015. Chicago, IL: Accreditation Council for Graduate Medical Education; http://www.acgme.org/About-Us/Publications-and-Resources/Graduate-Medical-Education-Data-Resource-Book. Accessed March 7, 2017. [Google Scholar]
- 13.Baldwin DC, Jr, Daugherty SR, Eckenfels EJ. Casualties of residency training: A national study of loss and attrition. In: Research in Medical Education 1988, Proceedings of the Twenty-Seventh Annual Conference. 1988:Washington, DC: Association of American Medical Colleges; 112–117.. [PubMed] [Google Scholar]
- 14.Baldwin DC, Jr, Rowley BD, Daugherty SR, Bay RC. Withdrawal and extended leave during residency training: Results of a national survey. Acad Med. 1995;70:1117–1124.. [PubMed] [Google Scholar]
- 15.Barger LK, Cade BE, Ayas NT, et al. ; Harvard Work Hours, Health, and Safety Group. Extended work shifts and the risk of motor vehicle crashes among interns. N Engl J Med. 2005;352:125–134.. [DOI] [PubMed] [Google Scholar]
- 16.Legha RK. A history of physician suicide in America. J Med Humanit. 2012;33:219–244.. [DOI] [PubMed] [Google Scholar]
- 17.Rosen IM, Christie JD, Bellini LM, Asch DA. Health and health care among housestaff in four U.S. internal medicine residency programs. J Gen Intern Med. 2000;15:116–121.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rotenstein LS, Ramos MA, Torre M, et al. Prevalence of depression, depressive symptoms, and suicidal ideation among medical students: A systematic review and meta-analysis. JAMA. 2016;316:2214–2236.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Sen S, Kranzler HR, Krystal JH, et al. A prospective cohort study investigating factors associated with depression during medical internship. Arch Gen Psychiatry. 2010;67:557–565.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.2015 ACGME Symposium on Physician Well-Being, November 29–December 1, 2016. http://www.acgme.org/What-We-Do/Initiatives/Physician-Well-Being/2016-ACGME-Symposium-on-Physician-Well-Being. Accessed March 8, 2017.
- 21.Ey S, Moffit M, Kinzie JM, Brunett PH. Feasibility of a comprehensive wellness and suicide prevention program: A decade of caring for physicians in training and practice. J Grad Med Educ. 2016;8:747–753.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Guille C, Zhao Z, Krystal J, et al. Suicidal ideation in medical interns: A randomized clinical trial. JAMA Psychiatry. 2015;72:1192–1198.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Christensen H, Cuijpers P, Reynolds CF., 3rd Changing the direction of suicide prevention research: A necessity for true population impact. JAMA Psychiatry. 2016;73:435–436.. [DOI] [PubMed] [Google Scholar]
- 24.Schernhammer ES, Colditz GA. Suicide rates among physicians: A quantitative and gender assessment (meta-analysis). Am J Psychiatry. 2004;161:2295–2302.. [DOI] [PubMed] [Google Scholar]
- 25.Emerson H, Hughes HE. Death rates of male white physicians in the United States, by age and cause. Am J Public Health (N Y). 1926;16:1088–1093.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Council on Scientific Affairs. Results and implications of the AMA-APA Physician Mortality Project: Stage II. JAMA. 1987;257:2949–2953.. [DOI] [PubMed] [Google Scholar]
- 27.Shanafelt TD, Hasan O, Dyrbye LN, Sinsky C, Sloan J, West CP. Changes in burnout and satisfaction with work–life balance in physicians and the general U.S. working population between 2011 and 2014. Mayo Clin Proc. 2015;90:1600–1613.. [DOI] [PubMed] [Google Scholar]
- 28.Dyrbye LN, Thomas MR, Massie FS, et al. Burnout and suicidal ideation among U.S. medical students. Ann Intern Med. 2008;149:334–341.. [DOI] [PubMed] [Google Scholar]
- 29.Scheepers RA, Boerebach BC, Arah OA, Heineman MJ, Lombarts KM. A systematic review of the impact of physicians’ occupational well-being on the quality of patient care. Int J Behav Med. 2015;22:683–698.. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wallace JE, Lemaire JB, Ghali WA. Physician wellness: A missing quality indicator. Lancet. 2009;374:1714–1721.. [DOI] [PubMed] [Google Scholar]
- 31.Nasca TJ. Open letter to the GME community. November 4 2016. Chicago, IL: Accreditation Council for Graduate Medical Education; http://www.acgme.org/Portals/0/PDFs/Nasca-Community/NascaLetterToTheCommunity_11-4-16.pdf. Accessed March 8, 2017. [Google Scholar]