
Figure 1.
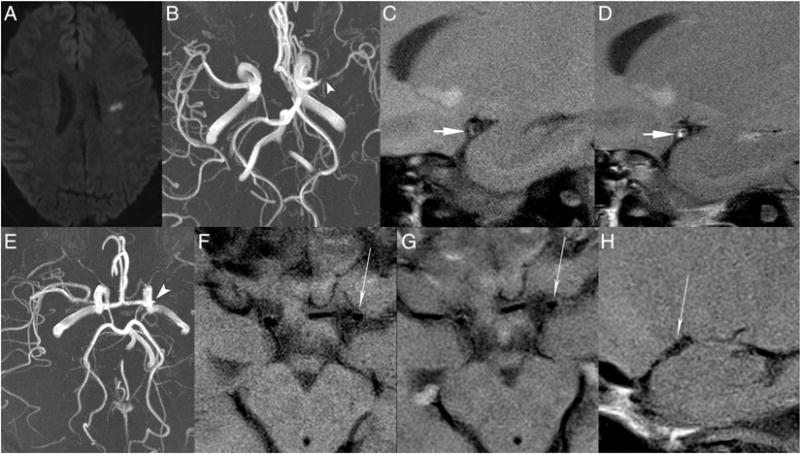
Atherosclerosis (A–D) and moyamoya disease (E–H). (A–D) A middle-aged homeless patient with 30 pack-year smoking history and IV drug abuse presented with a 4-day history of left middle cerebral artery (MCA) territory stroke. Axial diffusion-weighted imaging (A) shows multiple left MCA territory infarcts. Axial MR angiography (MRA) maximum intensity projection (MIP) (B) shows high-grade left MCA narrowing (arrowhead). Sagittal oblique T1 pre-contrast (C) and post-contrast (D) vessel wall sequences of the left MCA show an eccentric enhancing lesion with wall thickening and outward remodeling (short arrow), compatible with intracranial atherosclerotic disease. (E–H) A middle-aged patient without vascular risk factors, history of genetic syndromes, prior radiation, or evidence of central nervous system vasculitis presented with intermittent headaches and otherwise unremarkable clinical results. On axial MRA MIP (E) there is occlusion of the left carotid terminus (arrowhead) with attenuation of the right carotid terminus and proximal MCA. On axial T1 pre-contrast (F) and post-contrast (G) MRI of the carotid terminus and sagittal T1 post-contrast (H) MRI of the proximal MCA vessel wall there is no evidence of vessel wall enhancement, wall thickening, or outward remodeling (long arrows), most compatible with moyamoya disease.