
Figure 1.
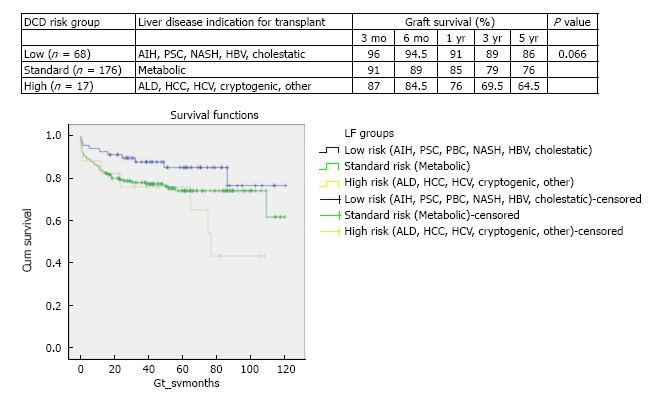
Stratified Kaplan-Meier curves for the cumulative donor after cardiac death graft survival in relation to primary indication for transplant and respective 3 mo, 6 mo, 1 year, 3 years and 5 years survival (χ2 5.1 log-rank, P = 0.066). This stratification of indication for transplant defining the three risk groups of low, standard and high. Low DCD risk indications for transplant included autoimmune hepatitis (AIH), primary sclerosing cholangitis (PSC), primary biliary cirrhosis (PBC), non-alcoholic steatohepatitis (NASH), hepatitis B virus (HBV) and cholestatic liver disease (primary familial intrahepatic cholestasis, extrahepatic biliary atresia and Crigler Najjar). Standard risk indications were metabolic diseases that included Wilson’s, Hemochromatosis and Familial Amyloid Polyneuropathy. High risk indications for DCD transplant were alcohol related liver disease (ALD), hepatocellular carcinoma (HCC), hepatitis C virus (HCV), cryptogenic and Budd Chiari.