

Abstract
We report two patients with Robinow or fetal face syndrome. We present a thirteen year follow-up on three previously published cases and a review of 32 cases in the literature. The cardinal features of this condition include mesomelic shortening of the forearms, frontal bossing, hypertelorism, wide palpebral fissures, short upturned broad nose with anteverted nares, long philtrum, small chin, brachydactyly, hypoplastic genitalia and a normal karyotype. Development delay and mental retardation was noted in 18% of the reported cases. Early death was identified in about 10% of the cases. Genetic heterogeneity is suggested with autosomal dominant inheritance reported in 8 individuals from 3 families and autosomal recessive inheritance in 8 siblings from 4 families although no clinical differences were identified among those individuals with different inheritance patterns. Male to male transmission was reported in one family. Parental age does not appear to be a factor in the cause of this syndrome.
Keywords: Fetal face, hypoplastic genitalia, mesomelic brachymelia, Robinow syndrome, short stature, skeletal abnormalities
In 1969, Robinow et al. reported a mother and her three children with mesomelic brachymelia, hemivertebrae, peculiar facies and genital hypoplasia. Since that time at least 32 cases have been reported (Robinow et al. 1969, Pfeiffer & Muller 1971, Wadlington et al. 1973, Feingold & Bull 1973, Schinzel et al. 1974, Seel et al. 1974, Seemanova et al. 1974, Hanssler & Schwanitz 1975, Giedion et al. 1976, Wadia et al. 1978, Wadia 1979, Portnoy 1979, Petit et al. 1980, Marni et al. 1980, Ziska et al. 1981, Shprintzen et al. 1982, Vallee et al. 1982, Khayat et al. 1983, Menon et al. 1983, Rodriquez-Costa et al. 1984, Saal et al. 1985). Herein we report follow-up studies on Wadlington et al. (1973) original patients, description of two additional patients and review of literature.
Case Presentations
L.H. was the product of a full term normal pregnancy and weighed 3175 g (30th percentile), height was 43 cm (less than third percentile) and head circumference was 34 cm (70th percentile). She was the second born child of an unrelated 18-year-old mother and 20-year-old father. The family history was negative for birth defects or genetic disorders. The patient was noted at birth to have a prominent forehead, short neck, short upturned nose with anteverted nares, broad nasal bridge, wide triangular shaped mouth, long philtrum, hypertelorism, gingival hyperplasia, low set ears, mesomelic shortening of extremities, nail dysplasia, brachydactyly with absent third toe on left foot, sacral dimple, hypoplastic labia minora and clitoris, and a systolic murmur (Fig. 1). X-ray studies showed 11 sets of ribs with several that were bifid, two thoracic hemivertebrae and shortening of the radius and ulna bilaterally. A cardiac catherization at two months of age revealed a coarctation of the aorta and a bicuspid aortic valve. The patient underwent repair of the coarctation at 3 months of age. The infant died at 7 months of age from viral pneumonia. An autopsy was not done.
Fig. 1.
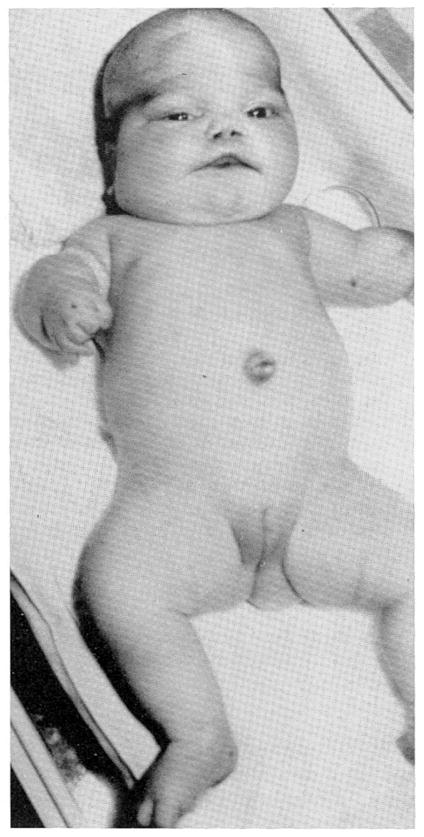
Frontal view of L.H. at two months of age.
M.W. was the product of a full term normal pregnancy to a 29-year-old mother. He weighed 3700 g (75th percentile) and was 49 cm (15th percentile) in length. The family history was negative for short stature or birth defects and consanguinity was denied. The patient was noted at birth to have short arms and legs, abnormal facies and hypoplastic genitalia. Follow up at 9 months revealed an active child with mesomelic brachymelia, frontal bossing, hypertelorism, wide palpebral fissures, short upturned nose with a broad nasal bridge, anteverted nares, long philtrum, large triangular shaped mouth, enamel hypoplasia, gingival hyperplasia, small chin, brachydactyly, pectus excavatum, hypoplastic penis and cryptorchidism. He rolled over at 2 months, sat alone at 6 months, and crawled at 8 months. X-ray studies showed hemivertebrae at T-9 and T-5, several fused thoracic ribs, and shortened radius and ulna with hypoplasia of the first metacarpal bone. The child has been followed since birth with measurements on 16 separate occasions. His height has ranged from the 15th (at birth) to the third percentile (10 years of age) and weight has ranged from the 75th (at birth) to the third percentile (10 years of age). He is currently a healthy ten-year-old with normal intelligence (Fig. 2). No additional findings were identified except a mild bilateral sensorineural hearing loss. High resolution chromosome studies were normal.
Fig. 2.

Frontal and profile views of M.W. at 6 weeks (a), 2 years (b) and ten years of age (c).
J.G. (patient no. 3 from Wadlington et al. 1973) is now a 22-year-old white male with normal intelligence. He had penoplasty at 6 years of age and placement of a Herrington rod for scoliosis at 8 years of age. He graduated from college and is employed in a print shop. He is healthy and weighs 100 pounds (<3rd percentile), height is 57 inches (< 3rd percentile) and head circumference is 53.5 cm (10th percentile). He is unmarried and functions as a normal male. High resolution chromosome studies were normal.
D.B. (patient no. 2 from Wadlington et al. 1973) is a healthy 19-year-old white male with borderline short stature (5th to 10th percentile) and of normal intelligence (Fig. 3). He graduated from high school and functions as a normal male.
Fig. 3.
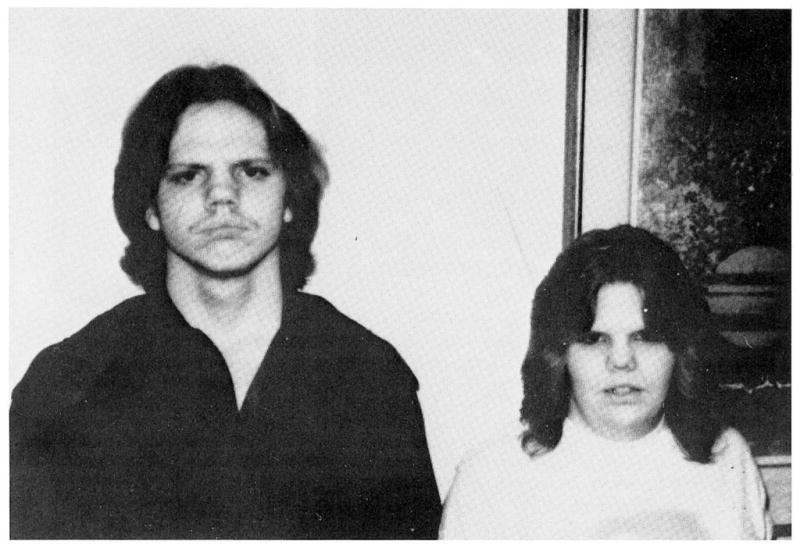
Frontal views of siblings D.B. and LB. at 19 and 21 years, respectively.
L.B. (patient no. 1 from Wadlington et al. 1973) is the sister of D.B. (Fig. 3). Both parents were unaffected. She is a healthy 21-year-old white female with short stature and normal intelligence. She has two normal children.
Longitudinal height and weight growth data were recorded for M.W., D.B., J.G., and L.B. Their height and weight growth curves are shown in Figures 4 through 7.
Fig. 4.

Height of J.G. (★), D.B. (○) and M.W. (●) plotted against chronological age.
Fig. 7.

Weight of L.B. plotted against chronological age.
Discussion
Robinow or fetal face syndrome is characterized by short forearms and hands, short stature, flat facial profile with hypertelorism, a short upturned nose, vertebral abnormalities and hypoplastic genitalia. We present two additional patients with this rare syndrome, a thirteen year follow-up on three previously reported patients and review of 32 published cases.
In our review of the literature two affected siblings were not included due to inadequate individual information (Saal et al. 1985). Our findings from the review are presented in Table 1.
Table 1.
Summary of clinical features in Robinow syndrome
| Clinical features | M.W. | L.H. | Literature | Total | % |
|---|---|---|---|---|---|
| Gestation and family history | |||||
| Normal pregnancy | + | + | 31/31 | 33/33 | 100 |
| Normal birth weight | + | + | 22/25 | 24/27 | 89 |
| Family history | − | − | 14/32 | 14/34 | 41 |
| Cranio-facial | |||||
| Hypertelorism | + | + | 32/32 | 34/34 | 100 |
| Short upturned nose | + | + | 32/32 | 34/34 | 100 |
| Broad nasal bridge | + | + | 30/31 | 32/33 | 97 |
| Anteverted nares | + | + | 31/32 | 33/34 | 97 |
| Triangular mouth | + | + | 27/29 | 29/31 | 94 |
| Frontal bossing | + | + | 29/31 | 31/33 | 94 |
| Long philtrum | + | + | 27/31 | 29/33 | 88 |
| Micrognathia | + | + | 24/28 | 26/30 | 87 |
| Wide palpebral fissures | + | + | 23/27 | 25/29 | 86 |
| Downslanting palpebral fissures | + | − | 19/23 | 20/25 | 80 |
| Ear abnormality | + | + | 15/30 | 17/32 | 53 |
| Macrocephaly | + | − | 11/25 | 12/27 | 44 |
| Facial nevus | − | − | 7/28 | 7/30 | 23 |
| Oral | |||||
| Dental abnormalities | + | ? | 22/23 | 23/24 | 96 |
| Gingival hyperplasia | + | + | 19/30 | 21/32 | 66 |
| Abnormal uvula | − | − | 4/20 | 4/22 | 18 |
| Cleft lip/palate | − | − | 3/32 | 3/34 | 9 |
| Musculoskeletal | |||||
| Short stature | + | + | 22/31 | 24/33 | 73 |
| Vertebral anomalies | + | + | 19/30 | 21/32 | 66 |
| Scoliosis | + | − | 11/22 | 12/24 | 50 |
| Rib defects | + | + | 9/29 | 11/31 | 36 |
| Delayed bone age | + | ? | 4/14 | 5/15 | 33 |
| Inguinal or umbilical hernias | − | − | 6/28 | 6/30 | 20 |
| Pectus excavatum | + | − | 4/24 | 5/26 | 19 |
| Acrodysostosis | − | − | 4/30 | 4/32 | 12 |
| Extremities | |||||
| Mesomelic brachymelia | + | + | 32/32 | 34/34 | 100 |
| Small hands with clinodactyly | + | + | 27/31 | 29/33 | 88 |
| Nail dysplasia | + | + | 9/21 | 11/23 | 48 |
| Uro-genital | |||||
| Hypoplastic genitalia | + | + | 27/29 | 29/31 | 94 |
| Cryptorchidism | + | NA | 12/19 | 13/20 | 65 |
| Renal abnormalities | ? | ? | 4/14 | 4/14 | 29 |
| Other | |||||
| Normal karyotype | + | ? | 17/17 | 18/18 | 100 |
| Normal intelligence | + | ? | 21/26 | 22/27 | 82 |
| Early death | − | + | 3/32 | 4/34 | 12 |
| Hematological disorders | − | − | 3/32 | 3/34 | 9 |
| Hip dislocation | − | − | 2/26 | 2/28 | 7 |
| Heart defect | − | + | 1/30 | 2/32 | 6 |
| Malignancy | − | − | 1/32 | 1/34 | 3 |
Little information on adults with Robinow syndrome exists in the literature. Three adult cases have been previously reported (Robinow et al. 1969, Shprintzen et al. 1982, Vallee et al. 1982). Therefore follow-up information on our previously reported patients is useful in order to determine the intelligence, height and health problems that may be present in the adult individual. The present average age of the three patients previously reported by Wadlington et al. (1973) is 21 years. They have normal intelligence, attended school and participated in regular activities including athletics. They have few physical limitations or health problems and the female patient has delivered two normal children.
Early death in Robinow syndrome was noted in three cases. These individuals died from hemorrhage (Petit et al. 1980) or pneumonia (Wadlington et al. 1973, Seemanova et al. 1974). Therefore early death was a finding in about 10% of reported cases.
Congenital heart disease is also a rare finding in this syndrome. L.H. had coarctation of the aorta and pneumonia which led to her demise. Another case of Robinow syndrome with a heart disorder was reported by Kelly et al. (1975).
The inheritance patterns in Robinow syndrome is not clear. Autosomal dominant inheritance has been reported in 8 individuals from 3 families (Robinow et al. 1969, Shprintzen et al. 1982, Vallee et al. 1982). Autosomal recessive inheritance has been identified in 8 siblings from 4 separate families (Wadlington et al. 1973, Seemanova et al. 1974, Wadia et al. 1979, Saal et al. 1985). Male to male transmission has been reported in one family (Shprintzen et al. 1982). Genetic heterogeneity is suggested by the two inheritance patterns seen in Robinow syndrome, although no obvious physical differences between patients with the two inheritance patterns were identified by reviewing published cases. In some cases advanced paternal age has also been incriminated (Kelly et al. 1975). Another explanation for the apparent heterogeneity might be a subtle chromosomal abnormality [for example, chromosome 15 deletion in the Prader-Willi syndrome (Ledbetter et al. 1982, Butler et al. 1986)] segregating in certain families. Although routine chromosome studies have been normal, we have evaluated several of our patients with high resolution chromosome analysis but no abnormality was identified.
In the review of literature, sibling data were available in 20 families. Twenty-eight of 53 siblings were affected with Robinow syndrome. A segregation analysis (Weinberg proband method) of the family data produced a probability estimate of 0.3. Therefore, in families with one child affected and without a family history of Robinow syndrome, autosomal recessive inheritance or a 25% recurrence risk should be discussed.
Affected individuals with Robinow syndrome tend to have short stature but their weight and length may be within normal limits and remain within the normal range or fall below the third percentile as represented by the longitudinal growth curves of our patients (Figures 4 to 7). The average birth weight in 25 patients reported with the syndrome was 3135 g. Small for gestational age was noted in 4 of 30 cases while 24 of 33 individuals had short stature (less than third percentile) at the time of their evaluation (average age of evaluation was 5.8 years). Short stature may appear by three to four years of age although one of our patients (D.B.) was within the normal range for height as an adult (Figure 4).
Skeletal abnormalities were frequently identified in this syndrome. The most common bone changes were vertebral anomalies, rib defects, shortening of the ulna and radius, bifid phalanges and occasionally acrodysostosis. Approximately 70% of the patients had hemivertebrae in the thoracic region while 40% of the patients had rib abnormalities, generally fusion or absent ribs. The majority of individuals had a normal bone age although delayed bone age was noted in approximately one third of the cases. Scoliosis was also noted in one half of the patients, particularly those individuals with vertebral and/or rib defects. The scoliosis was progressive in several cases and surgery was required to stabilize the spine. Bifid terminal phalanges and toes have been observed in several patients with Robinow syndrome and is considered a highly diagnostic radiological sign (Giedion et al. 1976). These investigators also reported similarity in hand pattern profiles in two patients.
An investigation is underway at our Center to determine if the metacarpophalangeal pattern profile analysis can be used as a tool for diagnosis in this syndrome similar to the analysis employed with the Prader-Willi and Sotos syndromes (Butler & Meaney 1985a, Butler et al. 1985b, Butler et al. 1986). This technique was useful in ruling out the diagnosis of Robinow syndrome in one of our patients suspected to have this disorder.
The intelligence is considered normal in the majority of patients with Robinow syndrome. Five of 27 patients were noted to have delayed development or mental retardation.
The male to female ratio of Robinow syndrome patients was 1.6 to 1 (21 males and 13 females). The sex ratio may be related to bias of ascertainment rather than a true sex difference but additional case reports are needed for clarification of this issue and to identify the incidence of this syndrome in the general population. The average age of the reported patients was 5.8 years and a relatively normal life expectancy is anticipated, although one male patient (7.8 years of age) was found to have Hodgkins disease (Giedion et al. 1976). Malignancy was not identified in any of the other reported patients, therefore, it is unlikely that Robinow syndrome patients are at an increased risk for malignancy.
The average paternal age was 26.8 years while the average maternal age was 25.2 years in 20 families with the Robinow syndrome. Therefore the paternal age appears not to be increased when compared with paternal ages in the general population [average maternal age = 25.0 years and average paternal age = 28.1 years (Van Dyke et al. 1983)].
Mesomelic shortening of the forearms, frontal bossing, hypertelorism, wide palpebral fissures, short upturned broad nose with anteverted nares, long philtrum, triangular shaped mouth, dental abnormalities, small chin, brachydactyly, hypoplastic genitalia, short stature and a normal karyotype occurred in nearly all cases and may be considered cardinal characteristics of this rare syndrome. Other clinical findings that were noted in only a few patients included: facial nevus, renal and ear abnormalities, cleft lip/palate, inguinal or umbilical hernias, congenital hip dislocation, pectus excavatum, abnormal uvula and gingival hyperplasia. If the above features are present, the diagnosis of Robinow syndrome should certainly be considered. The practical importance of the correct diagnosis for counseling and prognosis is emphasized.
Fig. 5.

Weight of J.G. (★), D.B. (○) and M.W. (●) plotted against chronological age.
Fig. 6.

Height of L.B. plotted against chronological age.
Acknowledgments
We thank Cheryl Edens and Laurie Gilbert for their assistance in the preparation of this manuscript.
References
- Butler MG, Meaney FJ. Metacarpophalangeal pattern profile analysis in Prader-Willi syndrome. A follow-up report on 38 cases. Clin Genet. 1985a;28:27–30. doi: 10.1111/j.1399-0004.1985.tb01213.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Meaney FJ, Kittur S, Hersh JH, Hornstein L. Metacarpophalangeal pattern profile analysis in Sotos syndrome. Am J Med Genet. 1985b;20:625–629. doi: 10.1002/ajmg.1320200408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Butler MG, Meaney FJ, Palmer CG. Clinical and cytogenetic survey of 39 individuals with the Prader-Labhart-Willi syndrome. Am J Med Genet. 1986;23:793–809. doi: 10.1002/ajmg.1320230307. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feingold M, Bull M. In: Syndrome Identification. Bergsma D, editor. White Plains, NY: National Foundation – March of Dimes; 1973. pp. 14–16. [Google Scholar]
- Giedion A, Battaglia GF, Bellini F, Fanconi G. The radiological diagnosis of the fetal face (Robinow) syndrome. Report of 3 cases. Helv Pediatr Acta. 1976;30:409–423. [PubMed] [Google Scholar]
- Hanssler H, Schwanitz G. Report on a variant of the fetal face syndrome with acral dysostosis. Klin Pediatr. 1975;187:2774–2777. [PubMed] [Google Scholar]
- Kelly TE, Benson R, Temtamy S, Plotnick L, Levin S. The Robinow syndrome. Am J Dis Child. 1975;129:383–386. doi: 10.1001/archpedi.1975.02120400081022. [DOI] [PubMed] [Google Scholar]
- Khayat D, Schiason G, Frija J, Szpirglas H. Robinow’s syndrome. Arch Fr Pediatr. 1983;40:327–330. [PubMed] [Google Scholar]
- Ledbetter DH, Mascarello JT, Riccardi VM, Harper VD, Airhart SD, Strobel RJ. Chromosome 15 abnormalities and the Prader-Willi syndrome: A follow-up report of 40 cases. Am J Hum Genet. 1982;34:278–285. [PMC free article] [PubMed] [Google Scholar]
- Marni E, Monafo V, Zanol MG, Pedroni E. The fetal face syndrome or Robinow syndrome. Description of a case. Minerva Pediatr. 1980;32:47–52. [PubMed] [Google Scholar]
- Menon PS, Thomas S, Matthews AR, Verma IC, Gupta A. Robinow syndrome. Indian Pediatr. 1983;20:783–787. [PubMed] [Google Scholar]
- Petit P, Fryns JP, Goddeeris P, Perlmutter-Cremer N. The Robinow syndrome. Ann Genet. 1980;23:221–223. [PubMed] [Google Scholar]
- Pfeiffer RA, Muller H. Ein Komplex multipler Missbildungen bei zwei nicht verwandten Kindern. Padiatr Padol. 1971;6:262–267. [PubMed] [Google Scholar]
- Portnoy Y. Robinow syndrome. Clin Pediatr. 1979;18:707–708. doi: 10.1177/000992287901801111. [DOI] [PubMed] [Google Scholar]
- Robinow M, Silverman FN, Smith HO. A newly recognized dwarfing syndrome. Am J Dis Child. 1969;117:645–651. doi: 10.1001/archpedi.1969.02100030647005. [DOI] [PubMed] [Google Scholar]
- Rodriquez-Costa T, Garcia-De-Leon R, Cases-Fernandez C, Puchemira A, Perez-Bryan J. Robinow syndrome: Presentation of a case and review of literature. An Esp Pediatr. 1984;20:55–61. [PubMed] [Google Scholar]
- Saal HM, Poole AE, Lodeiro JG, Weinbaum PJ, Greenstein RM. Autosomal recessive Robinow syndrome: Evidence for genetic heterogeneity. Am J Hum Genet. 1985;37:74A. [Google Scholar]
- Schinzel A, Zellweger H, Grella A, Prader A. Fetal face syndrome with acrodysostosis. Helv Pediatr Acta. 1974;29:55–60. [PubMed] [Google Scholar]
- Seel RE, Warner I, Passarge E. Robinow’s fetal face-dwarfism syndrome. Monatsschr Kinderheilkd. 1974;122:663–664. [PubMed] [Google Scholar]
- Seemanova E, Jirasek JE, Sevcikova M, Jodl J, Kreisinger J. Fetal face syndrome with mental retardation. Humangenetik. 1974;23:78–81. doi: 10.1007/BF00295686. [DOI] [PubMed] [Google Scholar]
- Shprintzen RJ, Goldberg RB, Saenger P, Sidoti E. Male to male transmission of Robinow’s syndrome. Am J Dis Child. 1982;136:594–597. doi: 10.1001/archpedi.1982.03970430026007. [DOI] [PubMed] [Google Scholar]
- Vallee L, Van Nerom PY, Ferraz FG, Delecour M, Maroteaux P, Farriaux JP, Fontaine G. Robinow’s syndrome with dominant transmission. Arch Fr Pediatr. 1982;39:447–448. [PubMed] [Google Scholar]
- Van Dyke DL, Miller MJ, Weiss L. The origin of inverted tandem duplications and phenotype effects of tandem duplication of the X chromosome long arm. Am J Med Genet. 1983;15:441–450. doi: 10.1002/ajmg.1320150309. [DOI] [PubMed] [Google Scholar]
- Wadia RS. Covesdem syndrome. J Med Genet. 1979;16:162. doi: 10.1136/jmg.16.2.162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wadia RS, Shirole DB, Dikshit MS. Recessively inherited costovertebral segmentation defect with mesomelia and peculiar facies (Covesdem syndrome) J Med Genet. 1978;15:123–127. doi: 10.1136/jmg.15.2.123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wadlington WB, Tucker VL, Schimke RN. Mesomelic dwarfism with hemivertebrae and small genitalia (the Robinow syndrome) Am J Dis Child. 1973;126:202–205. doi: 10.1001/archpedi.1973.02110190176013. [DOI] [PubMed] [Google Scholar]
- Ziska J, Gayer J, Juttnerova V, Balicek P, Tesarova B. Fetal face syndrome. Cesk Pediatr. 1981;36:328–330. [PubMed] [Google Scholar]