
Figure 3.
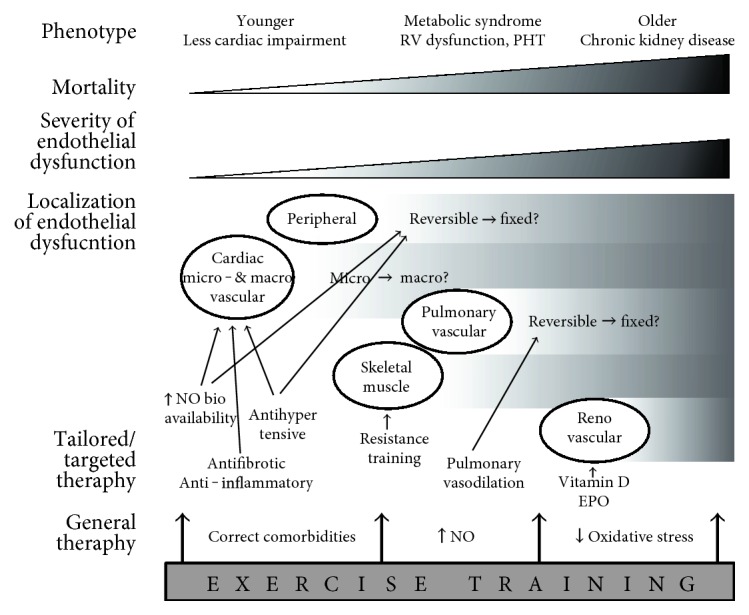
Possibilities for exercise training and targeted therapies depending on HFpEF phenotype. Cardiac ED is an early hallmark in all HFpEF patients. In older patients, pulmonary and renal vasculature are more frequently involved, and mortality is higher. HFpEF therapy could be tailored for each phenotype. Younger patients could still benefit from correction of comorbidities, preventing further systemic inflammation and ED. Increasing NO bioavailability, antifibrotic, or anti-inflammatory therapy could also be useful in early stages. Pulmonary vasodilation can only be effective when pulmonary vascular ED is manifested and still reversible. Exercise training has possible benefits at each stage, as it is able to correct comorbidities (weight loss, better glycemic control), increase NO bioavailability, and reduce systemic oxidative stress. EPO=erythropoietin, NO=nitric oxide, PHT=pulmonary hypertension, RV=right ventricle.