
Figure 3. Lesioning the motor cortex reverses behavioral recovery.
(A) Photomicrograph of exemplar electrolytic lesion in the hindlimb motor cortex (inset: cortical map showing lesion location centered at 1.0 mm caudal to bregma and 2.0 mm lateral). (B) Locomotor recovery measured by %WSS during treadmill locomotion evaluated before and after (pre-, post-) lesioning the motor cortex. (C) Proportion of BBB scores that correspond to weight support in the hindlimbs during unassisted open field locomotion (≥9) before and after (pre-, post-) cortical lesions. ***p<0.001. Error bars indicate 95% confidence intervals.

Figure 3—figure supplement 1. Quality of steps assessed from the videos based on individual paw placements.
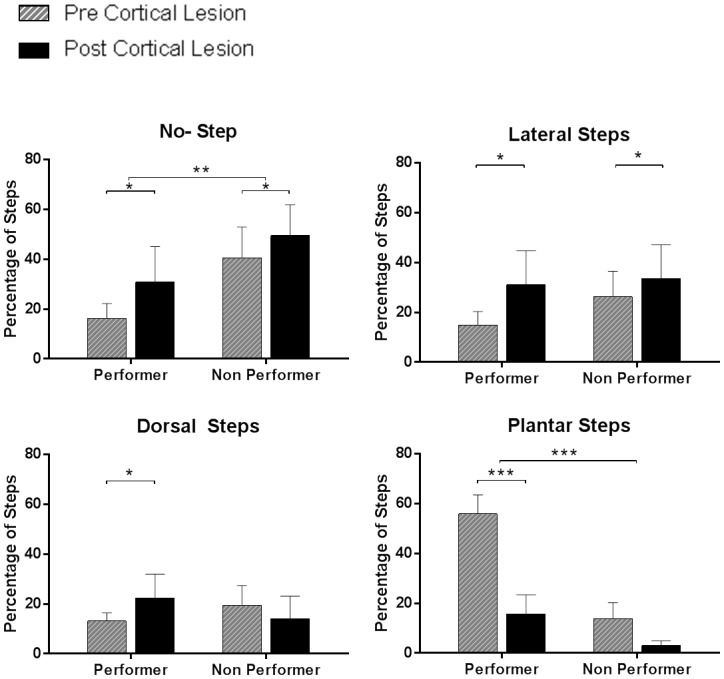
We performed video analyses from the treadmill testing data in animals that subsequently received cortical lesion (complete therapy, n = 12; partial therapy, n = 10), during testing at week-12 (pre-cortical lesion) and at week-14 (post-cortical lesion). Each of the 100 step cycles used for the %WSS was categorized – separately for each hindpaw – as no step (i.e. dragging), dorsal step (when the dorsal surface of the paw makes contact with the treadmill during paw placement), lateral step (when the animal performs a lateral sweep like motion without plantar contact) or plantar step (when the plantar surface of the paw comes in contact with the treadmill entirely during paw placement). Animals were categorized in two groups based on an arbitrary recovery threshold of 10 %WSS at week-12: animals with good recovery (performer, %WSS > 10, average 28.4 ± 11.1%, n = 11) and animals with poor recovery (non-performer, %WSS ≤ 10, average 2.8 ± 3.8%, n = 11). Left and right hindpaw steps were separated as an independent factor. As expected, the percentage of no steps was lower in performers than in non-performers (3-way ANOVA, group: F(1,40)=10.1, p=0.0028) and increased after cortical lesion in both groups (lesion: F(1,40)=6.8, p=0.0129). The percentage of dorsal steps was similar in the two groups (group: F(1,40)=0.05, p=0.82), with a tendency to increase after cortical lesion in performers but not in non-performers (group x lesion: F(1,40)=5.3, p=0.0261). The percentage of lateral steps was again similar in the two groups (group: F(1,40)=1.2, p=0.28) and increased after cortical lesion in both groups (lesion: F(1,40)=6.8, p=0.0127). Finally, the percentage of plantar steps was markedly higher in performers (group: F(1,40)=95.7, p<0.0001) and significantly decreased after the lesion in performers (lesion x group: F(1,40)=19.9, p<0.0001; Tukey: p=0.0002) but not in non-performers (Tukey: p=0.11). These results clarify that the ability to make plantar contact with the treadmill during stepping is key to achieve good recovery and that the reorganized motor cortex plays a critical role in this recovery. *p<0.05, **p<0.01, ***p<0.001.