
Figure 1.
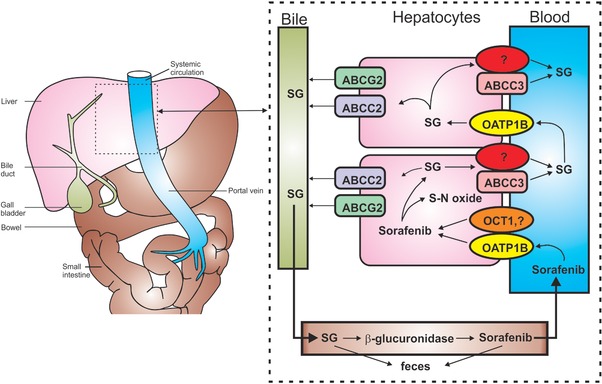
Hepatocyte hopping and recirculation of sorafenib‐β‐D‐glucuronide. After oral administration, sorafenib enters the hepatocytes by incompletely defined transporters mechanisms, including OATP1B‐type carriers and OCT1, and undergoes ABCG2‐mediated biliary secretion, CYP3A4‐mediated metabolism to sorafenib‐N‐oxide (S‐N‐oxide), or UGT1A9‐mediated glucuronidation to form sorafenib‐β‐D‐glucuronide (SG). After conjugation, SG is extensively secreted into the bile by a process that is mainly mediated by ABCC2. Under physiological conditions, a fraction of the intracellular SG is secreted by ABCC3 and at least one other transporter back to the blood, from where it can be taken up again into downstream hepatocytes via OATP1B‐type carriers. This secretion‐and‐reuptake loop may prevent the saturation of ABCC2‐mediated biliary excretion in the upstream hepatocytes, thereby ensuring efficient biliary elimination and hepatocyte detoxification. Once secreted into bile, SG enters the intestinal lumen, where it can either be excreted or serve as a substrate for an as‐yet unknown bacterial β‐glucuronidase that produces sorafenib, which is subsequently undergoing intestinal absorption and reenters the systemic circulation. This figure is a modified version of a figure from Vasilyeva et al.13 and is reprinted with permission.