

Abstract
Background
Spontaneous regression of metastatic melanoma and delayed responses more than one year after treatment with ipilimumab are rarely seen.
Case presentation
Here, we present the case of a patient with in transit metastases from cutaneous melanoma on his right lower extremity who achieved complete regression of all metastatic lesions 13 months after the first of two consecutive palliative resections of dominant masses and more than two years after treatment with ipilimumab.
Conclusion
The exact cause of our patient’s sudden onset of tumor regression remains speculative. We hypothesize that the operative trauma followed by the postoperative infections augmented an innate immune response.
Keywords: PD-1, Immune checkpoint blockade, Antibody therapy, Melanoma, Immunotherapy
Background
Immune checkpoint blockade using monoclonal antibodies have been approved by the US Food and Drug Administration (FDA) to treat patients with advanced melanoma. We describe a case involving a patient that received ipilimumab, a monoclonal antibody against cytotoxic T-lymphocyte associated protein 4 (CTLA-4). CTLA-4 is a cell surface receptor that negatively regulates the immune response and its blockade can influence anti-tumor T cell activity. Ipilimumab showed a survival benefit in Phase III trials involving patients with advanced melanoma [1, 2]. Durable tumor responses in patients with advanced melanoma treated with ipilimumab yielded a plateau in the survival curve at 21% starting at 3 years from study initiation [3]. Here, we present a patient with multifocal in-transit melanoma metastases who achieved spontaneous regression two years after completion of ipilimumab.
Case presentation
In October of 2012 an 84-year-old man with a history of coronary artery disease, COPD, hypertension, and venous insufficiency presented with multiple cutaneous nodules on his right leg. The lesions had been growing in size over the preceding 3 years (Fig. 1a). An excisional biopsy was performed and revealed a malignant melanoma with focal necrosis. The lesion was described as purple, tender, 2.7 × 2.5 × 1.5 cm in size. A PET/CT of the entire body demonstrated a dominant soft tissue mass lateral to the right fibular head with numerous additional soft tissue nodules extending from the right mid thigh anteriorly to the level of the ankle, compatible with multiple cutaneous and subcutaneous melanoma metastases (Fig. 1b). There was no evidence for distant metastatic disease. BRAFV600 status was found to be wild-type. The patient was not deemed a candidate for hyperthermic isolated limb perfusion due to peripheral vascular disease and the perceived very high risk for development of distant metastatic disease. Between December 2012 and February 2013 the patient received 4 cycles of the anti-CTLA-4 monoclonal antibody ipilimumab, at the standard dose of 3 mg/kg given once every 3 weeks, which he intially tolerated well except for intermittent low-grade diarrhea and fatigue. In April 2013, he developed anemia with a hemoglobin of 6.7 g/dl requiring transfusions. An extensive work up including bone marrow biopsy suggested pure red cell aplasia, which is rare however has been previously described after treatment with CTLA-4 blockade [4], as the most likely etiology. The patient was treated with a pulse of dexamethasone for 4 days at 1 mg/kg-day, with no change in his transfusion requirements and no rise of the reticulocyte count, then intravenous immunoglobulin (IVIg), with no reticulocytosis and no normalization of his hemoglobin. His cytogenetics showed 5/20 cells positive for del(5q), consistent with myelodysplastic syndrome and he therefore received a course of lenalidomide between April and June 2013, which was eventually stopped 2nd to renal toxicity and substantial improvement of the anemia. His anemia was ultimately attributed to pure red cell aplasia, which was caused by ipilimumab and resolved over a period of 6 months despite documentation of 5q- myelodysplastic syndrome.
Fig. 1.
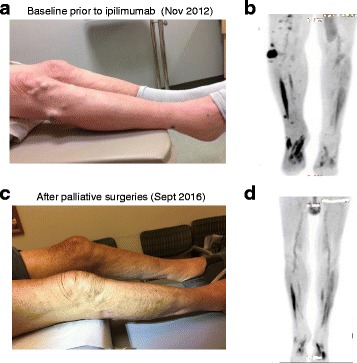
In transit metastases as evident clinically and on PET. a, b At baseline (October/November 2012). c, d Two years after the 2nd of 2 palliative surgical resections (September 2016)
Between December 2012 and December 2013 there was continued slow growth of the right lower extremity metastases. By January 2014 accelerated progression of disease with substantial increase in the size of pre-existent right lower extremity skin nodules as well as development of new nodules was noted. A nodule in the lateral right popliteal area enlarged to a size of ca. 4 cm over a few weeks and became ulcerated and chronically infected. The patient was not a candidate for a clinical trial using PD-1/PD-L1 blockade. Given the lack of distant metastatic disease and the absence of compelling systemic treatment options, in February 2014 a palliative resection of the fast growing dominant nodule was performed. The patient had a complicated postoperative course with wound dehiscence and recurring infections requiring intense wound care over a period of 3 months. During the protracted postoperative course there was further growth of multiple skin metastases with emergence of new lesions both clinically and on restaging scans while no distant metastases were evident. Another palliative resection of a fast growing nodule on the right medial knee was performed in August 2014. By November 2014, almost 2 years after the first treatment with ipilimumab and 9 months after the first of 2 palliative resections, the patient noted shrinkage of several skin nodules. A restaging PET/CT performed in December 2014 showed a mixed response. By March 2015 (2 years after completion of ipilimumab) all non-resected in transit metastases had completely disappeared clinically; radiographically, in May 2015 there was a continued mixed response with most lesions reduced in size. By August 2016, all in transit metastases had resolved both clinically and radiographically and the patient remains in a complete clinical and radiographic response (Fig. 1c, d). Dual immunohistochemical staining of CD3 and CD8 with the melanoma marker SOX10 demonstrated brisk infiltration with CD3+ and CD8+ T cells in both surgically resected in transit metastases, suggesting a T cell mediated immune response against the tumor in both samples (Fig. 2). The metastasis which was resected in February 2014 was highly necrotic with some areas of viable tumor as evident by SOX10 staining, whereas no necrosis was seen in the metastasis that was removed in August 2014.
Fig. 2.
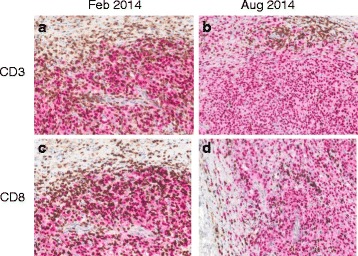
Melanoma surgical resection specimens were co-stained for CD3/SOX10 and CD8/SOX10, respectively. a CD3/SOX10, c, CD8/SOX10 staining of tumor resected in Feb of 2014. b CD3/SOX10, d, CD8/SOX10 staining of tumor resected in August of 2014
Conclusion
We describe the case of an 84 year old man who presented with multiple in transit melanoma metastases on his right lower extremity that did not respond to ipilimumab, but eventually completely regressed, almost 2 years after the initial dose of ipilimumab, following two serial palliative resections of dominant masses that had became ulcerated and painful. Delayed tumor responses have been reported in melanoma patients treated with ipilimumab. The observation of delayed response kinetics and unusual response patterns with immunotherapy have lead to the development of immune related response criteria [5, 6]. These response patterns can include transient increases in baseline tumor lesions or development of new metastases. Nevertheless, a delay of almost 2 years between the first ipilimumab dose and the regression of in transit metastases would be highly unusual. The fact that the tumor responses were observed shortly after the palliative resection that resulted in infectious wound healing complications suggests that a tumor specific immune response was triggered by these interventions. While spontaneous regression of primary melanomas is not an uncommon event, spontaneous regression of metastatic melanoma is exceedingly rare [7, 8]. A report by Kalialis et al. collected only 76 cases from the literature since 1866 [8]. Operative trauma has previously been associated with spontaneous regression of metastatic melanoma lesions. Furthermore, it is known that regression of cancers can occur in the context of infection, especially those caused by Streptococcus pyogenes, first reported by William Coley. Mimicking this situation deliberately by injecting patients with streptococcus lead to regression of sarcomas in a case series [9]. These early observations have been interpreted as the initial evidence for the potential of immunotherapy as a treatment for cancer. Notably in a review of 68 melanoma regression cases, 21 were led by a febrile episode, of which 9 were associated to erysipelas [10].
Although the exact cause of our patient’s sudden onset of tumor regression, eventually leading to disappearance of all clinically and radiographically evident tumors, remains speculative, an immune related mechanism seems most plausible. We hypothesize that the operative trauma followed by the postoperative infections triggered an innate immune response similiar to a microbial immune adjuvant such as a Toll Like Receptor or a STING agonist [11, 12]. Notably, these and other strategies that are aimed at de novo induction of inflammation in the tumor such as radiotherapy or the recently approved oncolytic virus Talimogene Laherparepvec (T-VEC), which have provided evidence for systemic anti-tumor activity and are in clinical investigation either as monotherapy or with immune checkpoint inhibition [13, 14]. For our patient, it is intriguing to speculate that his exposure to ipilimumab almost 2 years prior to the onset of tumor regression also contributed to the tumor response.
Methods
Dual immunohistochemical staining of CD3 (DAKO, A0452, 1:250) and CD8 (Dako, M7103, 1:200) with the melanoma marker SOX10 (EP 268, Cell Marque, 1:1500) was performed using an automated staining system (Bond III, Leica Biosystems, Buffalo Grove, IL) according to the manufacturer’s protocol, as previously described [15].
Acknowledgments
Funding
Not applicable.
Availability of data and materials
The datasets generated and analyzed during the current study are not publicly available due to individual privacy but are available from the corresponding author on reasonable request.
Abbreviations
- COPD
Chronic Obstructive Pulmonary Disease
- CT
Computerized tomography
- CTLA-4
Cytotoxic lymphocyte antigen-4
- FDA
Food and Drug Administration
- MRI
Magnetic Resonance Imaging
- PD-1
Programmed death-1
- PD-L1
Programmed death ligand 1
- PET/CT
Positron emission tomography computerized tomography
- T-VEC
Talimogene Laherparepvec
Authors’ contributions
PAO, RB, and LH drafted the manuscript. CY helped to draft the manuscript and participated in the care of the patient. KMK provided and analyzed data and helped to draft the manuscript. PAO conceived of the report, helped to draft the manuscript, and coordinated the care for the patient. All authors read and approved the manuscript.
Ethics approval and consent to participate
Clinical data for this case report were collected under institutional review board approval.
Consent for publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
Competing interests
PAO reports grants and personal fees from Bristol-Myers Squibb, CytomX, Celldex, and Merck, personal fees from Amgen, Novartis, Pfizer, and Roche/Genentech, and grants from AztraZeneca/MedImmune, outside of the submitted work. All other authors have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Raphael B. Moreira, Email: RaphaelB_Moreira@DFCI.HARVARD.EDU
Lana Hamieh, Email: LHAMIEH@PARTNERS.ORG.
Evisa Gjini, Email: Evisa_Gjini@dfci.harvard.edu.
Ana Lako, Email: Ana_Lako@dfci.harvard.edu.
Katherine M. Krajewski, Email: KMKRAJEWSKI@PARTNERS.ORG
Charles H. Yoon, Email: CHYOON@PARTNERS.ORG
Patrick A. Ott, Phone: 617-582-9030, Email: Patrick_Ott@dfci.harvard.edu
References
- 1.Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. 2010;363(8):711–723. doi: 10.1056/NEJMoa1003466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Robert C, Thomas L, Bondarenko I, O'Day S, Weber J, Garbe C, et al. Ipilimumab plus dacarbazine for previously untreated metastatic melanoma. N Engl J Med. 2011;364(26):2517–26. doi: 10.1056/NEJMoa1104621. [DOI] [PubMed] [Google Scholar]
- 3.Schadendorf D, Hodi FS, Robert C, Weber JS, Margolin K, Hamid O, et al. Pooled Analysis of Long-Term Survival Data From Phase II and Phase III Trials of Ipilimumab in Unresectable or Metastatic Melanoma. J Clin Oncol. 2015;33(17):1889–1894. doi: 10.1200/JCO.2014.56.2736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Gordon IO, Wade T, Chin K, Dickstein J, Gajewski TF. Immune-mediated red cell aplasia after anti-CTLA-4 immunotherapy for metastatic melanoma. Cancer Immunol Immunother. 2009;58(8):1351–1353. doi: 10.1007/s00262-008-0627-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebbe C, et al. Guidelines for the evaluation of immune therapy activity in solid tumors: immune-related response criteria. Clin Cancer Res. 2009;15(23):7412–7420. doi: 10.1158/1078-0432.CCR-09-1624. [DOI] [PubMed] [Google Scholar]
- 6.Di Giacomo AM, Danielli R, Guidoboni M, Calabro L, Carlucci D, Miracco C, et al. Therapeutic efficacy of ipilimumab, an anti-CTLA-4 monoclonal antibody, in patients with metastatic melanoma unresponsive to prior systemic treatments: clinical and immunological evidence from three patient cases. Cancer Immunol Immunother. 2009;58(8):1297–1306. doi: 10.1007/s00262-008-0642-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Requena C, Botella-Estrada R, Traves V, Nagore E, Almenar S, Guillen C. Problems in defining melanoma regression and prognostic implication. Actas Dermosifiliogr. 2009;100(9):759–766. doi: 10.1016/S0001-7310(09)72549-9. [DOI] [PubMed] [Google Scholar]
- 8.Kalialis LV, Drzewiecki KT, Klyver H. Spontaneous regression of metastases from melanoma: review of the literature. Melanoma Res. 2009;19(5):275–282. doi: 10.1097/CMR.0b013e32832eabd5. [DOI] [PubMed] [Google Scholar]
- 9.Coley WB. The Treatment of Inoperable Sarcoma by Bacterial Toxins (the Mixed Toxins of the Streptococcus erysipelas and the Bacillus prodigiosus) Proc R Soc Med. 1910;3(Surg Sect):1–48. [PMC free article] [PubMed] [Google Scholar]
- 10.Maurer SKK. Spontaneous regression of advanced melanoma. Onkologie. 1998;21:14–18. [Google Scholar]
- 11.Adams S. Toll-like receptor agonists in cancer therapy. Immunotherapy. 2009;1(6):949–964. doi: 10.2217/imt.09.70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Corrales L, McWhirter SM, Dubensky TW, Jr, Gajewski TF. The host STING pathway at the interface of cancer and immunity. J Clin Invest. 2016;126(7):2404–2411. doi: 10.1172/JCI86892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Postow MA, Callahan MK, Barker CA, Yamada Y, Yuan J, Kitano S, et al. Immunologic correlates of the abscopal effect in a patient with melanoma. N Engl J Med. 2012;366(10):925–931. doi: 10.1056/NEJMoa1112824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ott PA, Hodi FS. Talimogene Laherparepvec for the Treatment of Advanced Melanoma. Clin Cancer Res. 2016;22(13):3127–3131. doi: 10.1158/1078-0432.CCR-15-2709. [DOI] [PubMed] [Google Scholar]
- 15.Roemer MG, Advani RH, Redd RA, Pinkus GS, Natkunam Y, Ligon AH, et al. Classical Hodgkin Lymphoma with Reduced beta2M/MHC Class I Expression Is Associated with Inferior Outcome Independent of 9p24.1 Status. Cancer Immunol Res. 2016;4(11):910–916. doi: 10.1158/2326-6066.CIR-16-0201. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available due to individual privacy but are available from the corresponding author on reasonable request.