

Abstract
Intake of sweet food, beverages and added sugars has been linked with depressive symptoms in several populations. Aim of this study was to investigate systematically cross-sectional and prospective associations between sweet food/beverage intake, common mental disorder (CMD) and depression and to examine the role of reverse causation (influence of mood on intake) as potential explanation for the observed linkage. We analysed repeated measures (23,245 person-observations) from the Whitehall II study using random effects regression. Diet was assessed using food frequency questionnaires, mood using validated questionnaires. Cross-sectional analyses showed positive associations. In prospective analyses, men in the highest tertile of sugar intake from sweet food/beverages had a 23% increased odds of incident CMD after 5 years (95% CI: 1.02, 1.48) independent of health behaviours, socio-demographic and diet-related factors, adiposity and other diseases. The odds of recurrent depression were increased in the highest tertile for both sexes, but not statistically significant when diet-related factors were included in the model (OR 1.47; 95% CI: 0.98, 2.22). Neither CMD nor depression predicted intake changes. Our research confirms an adverse effect of sugar intake from sweet food/beverage on long-term psychological health and suggests that lower intake of sugar may be associated with better psychological health.
Introduction
Sugar consumption is increasingly discussed as an intervention target to reduce prevalence of obesity, diabetes and other non-communicable diseases1, 2. In Britain, adults consume approximately double, and in the U.S. triple, the recommended level of added sugar for additional health benefits (5% of energy intake), with sweet foods and drinks contributing three-quarters of the intake1, 3, 4. Meanwhile, major depression is predicted to become the leading cause of disability in high income countries by 20305.
Higher sugar consumption was linked to higher depression prevalence in several ecological and cross-sectional studies6–8. To date, few studies have investigated the prospective association of sweet food and beverage intake with depression9–12. Although all studies found an increased risk of depression with higher baseline consumption of added sugars, soft drinks, juices and pastries; none examined the role of ‘reverse causation’ in producing the observed association. Reverse causation refers, in this context, to the possibility that a mood disorder may lead to higher sugar intake, so that the diet-mental health association is wholly or partly the result of poor mental health rather than of high sugar intake13–15. A prospective study with repeat measures of food intake and mental health provides the opportunity to examine the bidirectional nature of the association, and to contribute novel evidence on the effect of sugar dense diet on depression in the general population.
There are several plausible biological explanations for an association of habitual sugar intake and subsequent risk of depression, in the long-term. Firstly, low levels of the growth factor brain derived neurotrophic factor (BDNF) have been discussed as facilitating neurogenesis and hippocampal atrophy in depression16. Rodents fed high-fat high-sugar diets, but not high-fat diets only, show a decrease in BDNF level17–19, which could be a mechanistic link between diets high in sugar and depression. Secondly, carbohydrate consumption has been associated with increased circulating inflammatory markers, which may depress mood20, 21. Thirdly, high sugar diets could induce hypoglycaemia through an exaggerated insulin response and thereby influence hormone levels and potentially mood states22. Fourthly, addiction-like effects of sugar suggest dopaminergic neurotransmission mechanisms might connect frequent sugar intake with depression23–25. Lastly, obesity could be a mediating factor between a sugar-dense diet and depression26, 27 not only via inflammatory but also psychosocial factors like weight discrimination28.
The aim of this study is to investigate whether sugar intake from sweet food/beverages is positively associated with the risk of both incident and recurrent mood disorders, and to establish the role of the reverse effect in the Whitehall II cohort, using prospective, repeat measures data collected over a 22 year period.
Methods
Study cohort
The Whitehall Study II consists of non-industrial civil servants, who were recruited in London at age 35 to 55 years during 1985–1988 (phase 1). The initial sample size was 10,308 individuals (33.1% female and 66.9% male). The participants were followed up via questionnaire in 1989–1990 (phase 2), 1991–1993 (phase 3), 1995–1996 (phase 4), 1997–1999 (phase 5), 2001 (phase 6), 2003–2004 (phase 7), 2006 (phase 8), 2008–2009 (phase 9) and 2012–2013 (phase 11). In phases 1, 3, 5, 7, 9 and 11 they were additionally invited for screening in a research clinic29. Phase 10 (2011) consisted of a smaller sample of participants used for a pilot study. The study was approved by the Joint UCL/UCLH Committee on the Ethics of Human Research and carried out in accordance with the ethical principles set out in the Declaration of Helsinki. Further all participants have been asked for informed consent at every follow-up.
Ascertainment of sugar intake from sweet food/beverages
Diet was assessed at phases 3, 5, 7 and 9 using a 127-item machine-readable semi-quantitative food frequency questionnaire (FFQ) which originates from the tool used in the US Nurses’ Health Study, a self-administered questionnaire on habitual diet over the past 12 months30, 31. In order to reflect most diets in the UK it has been modified and anglicized32. This FFQ has been validated against a 7 day diet diary in a stratified random sample of 865 participants in the Whitehall Study II at collection phase 330. Sweet food and beverage intake was measured with 15 items such as cakes, biscuits, added sugar to coffee or tea, and fizzy soft drinks (see Supplementary Table S1). Sugar intake was calculated by multiplying sweet food/beverage consumption frequencies per day by their sugar content and portion size based on McCance and Widdowson’s The Composition of Foods, 5th edition 33.
Depressive symptom assessment
The 30-item General Health Questionnaire (GHQ) measures depressive and somatic symptoms over the past two weeks34. Caseness was defined as reporting ≥5 symptoms and is referred to as common mental disorder (CMD). This measure was included in follow-up questionnaires at all phases apart from phase 4. In addition, the 20-item Center of Epidemiologic Studies Depression Scale (CES-D), a self-report measure of depressive symptoms in the general population over the past week35, was administered at phases 7, 9 and 11. Individuals scoring ≥16 were considered cases of depression36. Lastly, a clinical interview using the Revised Clinical Interview Schedule (CIS-R) was administered at phase 11 with participants assessed according to International Classification of Diseases (ICD-10) F32 criteria. The computerized self-completion version of the CIS-R included questions on depressive symptoms that were present for at least 2 weeks37–39. The GHQ and CES-D have been validated against the CIS-R in this cohort and showed high sensitivity and specificity in measuring depressive episodes39.
Covariates
Potential confounders were chosen based on review of the literature and restricted to variables available at all phases used in the analyses. All estimates were initially adjusted for age, ethnicity (White/ South Asian/ Black) and sex, with an interaction of sex and age where both sexes included. Socio-demographic variables consisted of marital status (married/cohabiting, single or divorced/widowed) and last employment grade level within the civil service, (high, intermediate, low). Health behaviours included smoking (never, former, current), alcohol intake (none: ≤1 unit/weeks, moderate, heavy: ≥14 units/week) self-reported physical activity (vigorous, moderate and non/mild)40 and duration of sleep (5 categories from ≤5 hours to ≥9 hours/day). Diet-related factors comprised energy intake, diet quality, fish, coffee and tea intake based on FFQ data. Energy intake was used to ascertain dietary misreporting. Misreporting was considered where the log ratio of energy intake to estimated energy expenditure was outside of 3 SD of the log mean. This definition was adopted by Mosdol et al. 2007 and based on basal metabolic rate equations of the Department of Health41–43. Since sugar intake from sweet food/beverages was strongly correlated with energy intake (r = 0.61, P < 0.001), energy intake was adjusted for with the partition method by using energy intake from other foods44. Diet quality was assessed using the Dietary Approaches to Stop Hypertension (DASH) diet score modified by excluding a measure for sweet drinks45. DASH diet score, coffee and tea intake were analysed as continuous variables, fish intake per day as quintiles and all dichotomized for descriptive analyses. Body mass index (BMI) (kg/m2) and central obesity (in women waist circumference ≥88 cm and in men ≥102 cm) were both measured by trained staff46. Physical health was defined as diabetes and cardiovascular disease (coronary heart disease and stroke, CVD) based on self-reports which were validated using the study clinical examination, Hospital Episode Statistics data, and by contacting general practitioners for confirmation when no other external source existed. Cancer was based on cancer registration data29. Finally, doctor diagnosis of depression was based on self-report at phases 1 to 4 and on self-reported antidepressant intake at all phases after phase 4.
Statistical analysis
At each phase, participants were included if they had answered at least 8 of the FFQ sweet food and beverage items47 (less than 5% of eligible sample had one missing item and about 1% two or more), their ethnicity was known to be either White, Black or South Asian, and participants were not energy misreporters (see above). In addition, participants were also excluded from analyses if they had incomplete data on GHQ-, CES-D- or CIS-R caseness for outcome-specific analyses, respectively. Supplementary Fig. S1 shows how the included sample was reached (see Online).
Three binary outcomes were analysed, GHQ caseness, CES-D caseness and CIS-R caseness. Daily sweet food and beverage intake was modelled as sex-specific tertiles of sugar intake from sweet food/beverages based on the distribution at phase 3 (in men <39.5, ≥39.5 to <67.0 and ≥67.0 g/day; in women <30.0, ≥30.0 to <51.0 and ≥51.0 g/day). To describe the sample at phase 3, GHQ cases, non-cases and tertiles of sugar intake by covariate were compared. To examine the prospective association of sugar intake from sweet food and beverages, a random effects logistic regression model (REM) was performed using the STATA command xtlogit 48, with exposures at phases 3, 5, 7 and 9 for GHQ caseness, and at phases 7 and 9 for CES-D caseness. The applicability of the REM was tested by introducing study phase-interactions and likelihood ratio tests (LRT). The prospective effect of sugar intake from sweet food/beverages on incident and recurrent CMD and depression was examined using REMs in 2, 5 and 10-year cycles49. Figure 1 shows the included phases for analyses using GHQ caseness as the outcome. For example, the association between sugar intake and GHQ status 2 years later was conducted by combining the associations between sugar intake at Phase 5 and incident GHQ caseness at Phase 6, and between sugar intake at Phase 7 and incident GHQ caseness at Phase 8. For all depression outcomes, incidence was assumed if no CMD was apparent at each baseline, and recurrence if CMD was apparent at each baseline. For the analyses of depression, two 5-year cycles (to Phase 9 and 11) and three 10 year cycles (to Phases 7, 9 and 11) were used. For clinical depression, one 5-year cycle and one 10-year cycle were used.
Figure 1.
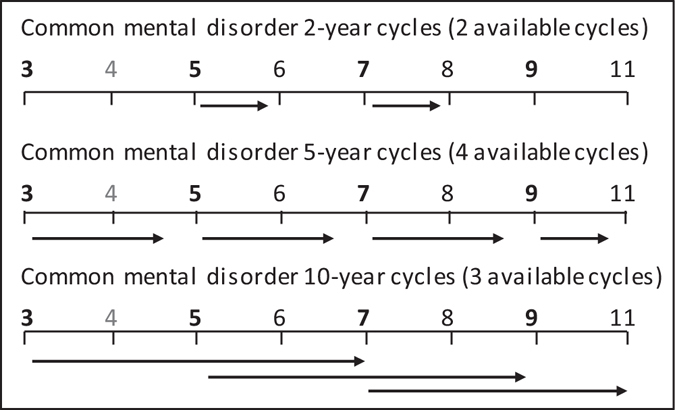
Modes of analysis using cycle approach for common mental disordera. Numbers indicate study phases. Phases with food frequency data in bold; no data on common mental disorder available at Phase 4. aCommon mental disorder measured using the 30-item General Health Questionnaire.
To check for reverse causation, that depressive symptoms may affect subsequent sugar intake from sweet food/beverages, linear regression models of 5-year change and multinomial logistic regression for change groups were fitted for each cycle, from phases 3 to 5, 5 to 7 and 7 to 9, with CMD at phases 3, 5, 7 respectively, and for change from phase 7 to 9 with depression at phase 7. Normal distribution of change in sugar intake from sweet food/beverages was verified using a histogram. Change groups were created by subtracting tertiles of sugar intake at baseline (t) from sugar intake from sweet food/beverages at follow-up (t + 5 y) and coding −2/−1 as decrease, 0 as no change and +1/+2 as increase in sugar intake from sweet food/beverages.
All analyses were performed using Stata 1450. Interactions of CMD and depression with sex in the initial model (Model 0 per sex-specific tertile trend: adjusted for age and ethnicity) were tested using LRT since sex-differences have been reported in a prior study on the association of diet and depression in the Whitehall II cohort51. Further adjustments were grouped into four hierarchical models: baseline socio-demographic factors and health behaviours (Model 1), diet-related factors (Model 2), BMI and central obesity (Model 3), and physical health (Model 4). In sensitivity analyses, main analyses were repeated by: (a) excluding participants with unknown or reported doctor diagnosis of depression at each baseline (at phases 3/5/7/9: 166/156/193/209 individuals) and: (b) excluding participants with extreme values of sugar intake (>7 SD) at phases 3/5/7/9: 5/3/4/4 individuals.
Results
Table 1 shows the prevalence of CMD and tertiles of reported sugar consumption from sweet food/beverages according to covariates at phase 3. CMD was more prevalent in women: under 50-years old, divorced/widowed, physically inactive, current smokers and those with fewer hours of sleep. Women with CMD were more likely to be in a lower grade level in civil service (P < 0.001; not depicted). Sugar consumption was associated with socio-demographic factors, health behaviours, physical health and diet-related factors (Table 1). Unexpectedly, participants in the highest tertile of sweet food/beverage intake had the highest prevalence of normal weight and lowest prevalence of overweight and obesity as well as the lowest prevalence of abdominal obesity in men (both P = 0.002; not depicted).
Table 1.
Crude association of common mental disorder and sugar intake from sweet food/beverages with covariates at phase 3.
| Covariates at phase 3 | n | Common mental disorder casesa | Sugar intake from sweet food/beverages | ||||
|---|---|---|---|---|---|---|---|
| % | P | Tertile 1 | Tertile 2 | Tertile3 | P | ||
| % | % | % | |||||
| Sex | <0.001 | 0.84 | |||||
| Men | 5,603 | 20.7 | 69.0 | 69.7 | 69.1 | ||
| Women | 2,484 | 25.7 | 31.0 | 30.3 | 30.9 | ||
| Age | <0.001 | 0.87 | |||||
| <50 years | 4,264 | 25.3 | 53.1 | 52.5 | 52.6 | ||
| ≥50 years | 3,823 | 18.9 | 46.9 | 47.5 | 47.4 | ||
| Ethnic Group | 0.03 | ||||||
| White | 7,423 | 22.4 | 89.3 | 91.5 | 94.6 | <0.001 | |
| South Asian | 410 | 23.7 | 7.07 | 5.20 | 2.95 | ||
| Black | 254 | 15.7 | 3.63 | 3.33 | 2.47 | ||
| Marital Status | <0.001 | <0.001 | |||||
| Married/cohabiting | 6,197 | 20.7 | 75.9 | 78.8 | 75.5 | ||
| Single | 1,145 | 25.8 | 14.1 | 12.9 | 16.7 | ||
| Divorced/widowed | 705 | 29.9 | 10.0 | 8.36 | 7.82 | ||
| Last grade level in Civil service | 0.19 | 0.03 | |||||
| Highest | 3,119 | 21.8 | 36.3 | 39.7 | 39.7 | ||
| Intermediate | 3,639 | 23.1 | 46.0 | 44.2 | 44.8 | ||
| Lowest | 1,329 | 20.8 | 17.7 | 16.1 | 15.5 | ||
| Smoking | 0.006 | <0.001 | |||||
| Never Smoker | 3,540 | 21.0 | 42.7 | 47.6 | 49.4 | ||
| Ex-Smoker | 2,957 | 22.4 | 41.9 | 38.3 | 36.5 | ||
| Current Smoker | 1,108 | 25.5 | 15.4 | 14.2 | 14.2 | ||
| Physical activity | <0.001 | 0.002 | |||||
| Non/mild | 3,027 | 25.4 | 40.3 | 36.6 | 35.4 | ||
| Vigorous | 1,475 | 19.1 | 17.9 | 17.8 | 19.0 | ||
| Alcohol consumption | 0.94 | <0.001 | |||||
| None | 1,916 | 22.4 | 20.8 | 22.3 | 28.0 | ||
| Moderate | 4,208 | 22.1 | 48.3 | 53.8 | 54.1 | ||
| Heavy | 1,955 | 22.4 | 30.9 | 23.9 | 17.9 | ||
| Sleep duration | <0.001 | 0.33 | |||||
| less than 7 h/day | 2,055 | 27.3 | 26.4 | 24.6 | 25.4 | ||
| ≥7 h/day | 6,022 | 20.5 | 73.6 | 75.4 | 74.6 | ||
| Energy intake from other diet | 0.03 | <0.001 | |||||
| <median (1339 kcal) | 4,042 | 21.2 | 61.8 | 52.6 | 35.7 | ||
| >median (2107 kcal) | 4,045 | 23.3 | 38.2 | 47.4 | 64.3 | ||
| Modified DASH diet score | 0.71 | <0.001 | |||||
| <median (17.7) | 4,522 | 22.1 | 50.6 | 55.6 | 61.7 | ||
| >median (24.8) | 3,559 | 22.4 | 49.4 | 44.4 | 38.3 | ||
| Fish intake ( | 0.38 | 0.02 | |||||
| <median (1 portion/week) | 4,597 | 21.9 | 56.6 | 58.9 | 55.1 | ||
| >median (4 portions/week) | 3,489 | 22.7 | 43.4 | 41.1 | 44.9 | ||
| Coffee and tea | 0.91 | <0.001 | |||||
| ≤1 cup of either/day | 714 | 22.4 | 11.0 | 8.54 | 6.96 | ||
| >1 cup of either/day | 7,373 | 22.2 | 89.0 | 91.5 | 93.0 | ||
| Body mass (BMI) | 0.02 | <0.001 | |||||
| Normal weight (<25 kg/m2) | 4,052 | 22.7 | 48.2 | 52.0 | 57.7 | ||
| Overweight (25–29.9 kg/m2) | 2,905 | 20.4 | 40.4 | 38.9 | 34.0 | ||
| Obese (≥30 kg/m2) | 737 | 24.3 | 11.4 | 9.04 | 8.33 | ||
| Central obesity | 0.59 | 0.21 | |||||
| No | 6,938 | 21.9 | 90.4 | 91.1 | 91.8 | ||
| Yes (Waist ≥88 (F)/102 (M)) | 679 | 22.8 | 9.61 | 8.94 | 8.20 | ||
| Diabetes | 0.90 | <0001 | |||||
| No | 7,861 | 22.2 | 96.1 | 97.4 | 98.1 | ||
| Yes | 226 | 22.6 | 3.92 | 2.58 | 1.88 | ||
| CVD | 0.03 | 0.007 | |||||
| No | 7,817 | 22.1 | 95.8 | 96.7 | 97.3 | ||
| Yes | 273 | 27.5 | 4.18 | 3.29 | 2.65 | ||
| Cancer | 0.58 | 0.32 | |||||
| No | 7.973 | 22.3 | 98.7 | 99.0 | 98.5 | ||
| Yes | 105 | 20.0 | 1.33 | 1.05 | 1.51 | ||
Abbreviations: SD = Standard Deviation, CVD = cardiovascular disease, DASH = Dietary Approaches to Stop Hypertension. P for difference or heterogeneity, derived from t-test, chi-square test, ANOVA or Kruskal-Wallis test. aCommon mental disorder measured using the 30-item General Health Questionnaire.
Incidence of CMD was around 9 to 15%, highest in the first cycle but did not differ greatly by cycle length. Depression and clinical depression incidence were approximately 8% and 2%, respectively. About 44% of participants who were CMD cases at baseline of each cycle remained recurrent CMD cases, 47% became recurrent depression cases and 58% recurrent clinical depression cases.
Cross-sectional results
Cross-sectional analyses showed strong positive associations between sugar intake from sweet food/beverages and common mental disorder from the GHQ, as well as CES-D caseness, when adjusted for age, sex and ethnicity (Table 2). There was no evidence for any interaction with sex (P = 0.8 for GHQ and P = 0.7 for CES-D). The association with CMD was robust whereas for depression it was removed on adjustment for socio-demographic factors, health behaviours and diet-related factors (Table 2). Further adjustments for central obesity and physical health (not shown), exclusion of 709 person-observations (377 in CES-D analysis) with reported doctor diagnosis of depression and person-observations with extreme values of sugar intake at baseline did not change the results.
Table 2.
Cross-sectional association of sugar intake from sweet food/beverages and prevalent common mental disorder and depression in men and womena.
| Prevalent common mental disorderb, OR (95% CI) | ||||
|---|---|---|---|---|
| events/person observations | Model 0c | Model 1d | Model 2e | |
| Sugar intake from sweet food/beverages | ||||
| Lowest Tertile | 1540/8402 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Middle Tertile | 1417/7439 | 1.08 (0.97, 1.20) | 1.10 (0.99, 1.22) | 1.07 (0.96, 1.19) |
| Highest Tertile | 1435/6872 | 1.22 (1.09, 1.36) | 1.25 (1.11, 1.41) | 1.17 (1.04, 1.32) |
| Total | 4392/22713 | |||
| P for trend | 0.001 | <0.001 | 0.011 | |
| Prevalent depression f , OR (95% CI) | ||||
| events/person observations | Model 0 g | Model 1 d | Model 2 e | |
| Lowest Tertile | 498/4025 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Middle Tertile | 360/3186 | 1.04 (0.83, 1.30) | 0.97 (0.77, 1.21) | 0.90 (0.72, 1.14) |
| Highest Tertile | 371/2684 | 1.36 (1.07, 1.73) | 1.25 (0.98, 1.59) | 1.08 (0.84, 1.39) |
| Total | 1229/9895 | |||
| P for trend | 0.016 | 0.098 | 0.643 | |
Abbreviations: OR = Odds ratio, CI = Confidence interval, DASH = Dietary Approaches to Stop Hypertension. aCross-sectional association across phases 3, 5, 7, 9 for common mental disorder and 7, 9 for depression. bCommon mental disorder measured using the 30-item General Health Questionnaire.; cCMD model 0 (4675 events/23954 person observations): adjusted for age*sex, ethnicity. dModel 1: additionally adjusted for marital status, last grade level in civil service, smoking, alcohol intake, physical activity, sleep duration. eModel 2: additionally adjusted for energy intake from other foods, modified DASH diet score, fish, coffee and tea intake. fDepression measured using 20-item the Centre of Epidemiologic Studies Depression Scale. gDepression model 0 (1313 events/10269 person observations): adjusted for age*sex, ethnicity.
Prospective results
Prospective analyses regarding incident CMD were stratified by sex, since interactions with sex were observed in the 5 years later model (LR test for sex interaction: GHQ 2 years later, P = 0.26: GHQ 5 years later, P = 0.05). In women, no associations were found for incident CMD with tertiles of sugar intake from sweet food/beverages (after 2 years, highest vs. lowest tertile OR: 0.98; 95% CI 0.72, 1.34; P for tertile trend = 0.90; after 5 years, highest vs. lowest tertile OR: 0.94; 95% CI 0.74, 1.19; P for tertile trend = 0.59). In men, after adjustment for age and ethnicity, sugar intake was associated with incident CMD 2 and 5 years later (Table 3). In further models, the association with 2-year incidence attenuated but the association with 5-year incidence remained (Table 3) and further adjustments for BMI, central obesity and physical health (not shown) resulted in an OR for highest vs. lowest tertile of: 1.23, 95% CI: 1.02, 1.48, P for trend = 0.03. Excluding participants who reported a doctor diagnosis of depression at each baseline strengthened the association (Model 4 for CMD after 5 years, Person observations = 10944; highest vs. lowest tertile OR; 1.25; 95% CI 1.03, 1.50; P for trend = 0.02, Supplementary Table S2) and exclusion of person observations with extremely high sugar intakes did not affect the results. In men and women, no association between sugar intake from sweet food/beverages and incident depression or clinical depression 5 years later was observed (Model 0, highest vs. lowest tertile OR, depression 0.92; 95% CI: 0.71, 1.18; P for tertile trend = 0.44; clinical depression: 0.95; 95% CI: 0.51, 1.75; P for trend = 0.84). The same exposure contrast was not associated with incident CMD or depression caseness after 10 years (Model 0, highest vs. lowest tertile OR: 1.10; 95% CI: 0.92, 1.31; P for tertile trend = 0.31; and 1.17; 95% CI: 0.91, 1.50, P for tertile trend = 0.25, respectively). However, sugar intake was positively associated with incident clinical depression after 10 years in men (Model 2 Person observations = 2572, cases = 35; P for tertile trend = 0.67), but negatively in women (Person observations = 848, cases = 28; P for tertile trend = 0.02).
Table 3.
Prospective association of sugar intake from sweet food/beverages and incident common mental disorder after 2 and 5 years in mena.
| Incident common mental disorderb after 2 years, OR (95% CI) | ||||
|---|---|---|---|---|
| events/person observations | Model 0c | Model 1d | Model 2e | |
| Sugar intake from sweet food/beverages | ||||
| Lowest Tertile | 220/2090 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Middle Tertile | 205/1836 | 1.08 (0.85, 1.38) | 1.08 (0.85, 1.38) | 1.04 (0.81, 1.33) |
| Highest Tertile | 202/1615 | 1.31 (1.02, 1.68) | 1.30 (1.01, 1.67) | 1.18 (0.90, 1.55) |
| Total | 627/5541 | |||
| P for trend | 0.039 | 0.047 | 0.233 | |
| Incident common mental disorder b after 5 years, OR (95% CI) | ||||
| events/person observations | Model 0 f | Model 1 d | Model 2 e | |
| Lowest Tertile | 477/4451 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Middle Tertile | 446/3958 | 1.05 (0.90, 1.23) | 1.07 (0.91, 1.25) | 1.04 (0.88, 1.22) |
| Highest Tertile | 463/3532 | 1.26 (1.07, 1.48) | 1.28 (1.08, 1.51) | 1.20 (1.01, 1.43) |
| Total | 1386/11941 | |||
| P for trend | 0.006 | 0.005 | 0.047 | |
Abbreviations: OR = Odds ratio, CI = Confidence interval, DASH = Dietary Approaches to Stop Hypertension.
aProspective association across phases 3, 5 for 2-year and 3, 5, 7, 9 for 5-year incident common mental disorder. bCommon mental disorder measured using the 30-item General Health Questionnaire.
c2-year model 0 (655 events/5767 person observations): adjusted for age and ethnicity. dModel 1: additionally adjusted for marital status, last grade level in civil service, smoking, alcohol intake, physical activity, sleep duration. eModel 2: additionally adjusted for energy intake from other foods, modified DASH diet score, fish, coffee and tea intake. f5-year model 0 (1448 events/12445 person observations): adjusted for age and ethnicity.
Prospective analyses regarding the associations of sugar intake from sweet food/beverages and recurrent mood disorders showed no evidence for sex interaction for CMD, CES-D depression or clinical depression 5 years later. Sugar intake from sweet food/beverages was positively associated with recurrent depression after 5 years (Model 0, highest vs. lowest tertile OR: 1.81; 95% CI: 1.23, 2.66; P for tertile trend = 0.003, Table 4). The association was attenuated when adjusted for other diet-related factors. Moreover, there was some evidence that sugar intake from sweet food/beverages was associated with recurrent clinical depression in both sexes combined (highest vs. lowest tertile OR: 1.66; 95% CI: 0.96, 2.87 and P for tertile trend = 0.07) when adjusted for age, sex and ethnicity (Supplementary Table S3). This association attenuated when further factors were introduced to the model. No statistically significant association was found for sugar intake from sweet food/beverages and recurrent GHQ caseness after 2 and 5 years (Model 0 for CMD after 2 years, highest vs. lowest tertile OR: 1.05; 95% CI 0.76, 1.45; P for tertile trend = 0.83; for CMD after 5 years: 1.16; 95% CI 0.93, 1.46; P for tertile trend = 0.20).
Table 4.
Prospective association of sugar intake from sweet food/beverages and recurrent depression after 5 yearsa.
| Recurrent depression after 5 years, OR (95% CI)b | ||||
|---|---|---|---|---|
| events/person observations | Model 0c | Model 1d | Model 2e | |
| Sugar intake from sweet food/beverages | ||||
| Lowest Tertile | 258/848 | 1.0 (reference) | 1.0 (reference) | 1.0 (reference) |
| Middle Tertile | 220/737 | 1.19 (0.83, 1.73) | 1.10 (0.76, 1.60) | 1.05 (0.72, 1.53) |
| Highest Tertile | 263/719 | 1.81 (1.23, 2.66) | 1.60 (1.08, 2.37) | 1.47 (0.98, 2.22) |
| Total | 741/2304 | |||
| P for trend | 0.003 | 0.017 | 0.071 | |
Abbreviations: OR = Odds ratio, CI = Confidence interval, DASH = Dietary Approaches to Stop Hypertension, CVD = cardiovascular disease. aProspective association across phases 7, 9 for recurrent depression. bDepression measured using 20-item the Centre of Epidemiologic Studies Depression Scale.
cModel 0 (792 events/2435 person observations): adjusted for age*sex, ethnicity. dModel 1: additionally adjusted for marital status, last grade level in civil service, smoking, alcohol intake, physical activity, sleep duration. eModel 2: additionally adjusted for energy intake from other foods, modified DASH diet score, fish, coffee and tea intake.
Analyses of recurrent CMD, depression and recurrent clinical depression after 10 years showed no associations with sugar intake from sweet food/beverages.
Sensitivity analyses excluding extreme values of sugar intake and excluding person-observations with self-reported doctor diagnosis at baseline attenuated the association of sugar intake from sweet food/beverages and recurrent depression slightly (before P for tertile trend 0.003 after 0.022 and 0.010, respectively). Similarly, associations with clinical depression weakened when participants with depression diagnosis at baseline were excluded (Model 0, Person observations = 573; cases = 78; P for tertile trend = 0.17).
Analysis of reverse causation
Sugar intake from sweet food/beverages decreased by 2.00 (SD 28.8; 95% CI 1.20, 2.79) grams per day from phase 3 to 5, by 3.44 (SD 28.0; 95% CI 2.59, 4.30) grams from phase 5 to 7 and by 1.57 (SD 26.0; 95% CI 0.91, 2.33) grams from phase 7 to 9, and was normally distributed. Mean 5-year change was approximately 31 g sugar from sweet food/beverages per day in the decrease group, −0.7 g in the stable intake group and 29 g in the increase group. Neither CMD, nor depression predicted 5-year changes in sugar intake (Table 5).
Table 5.
Association of common mental disorder and depression with subsequent 5-year change in sugar intake from sweet food/beverages.
| 5-year change in sugar intake | ||||
|---|---|---|---|---|
| No. of events | Participants | OR (95% CI) β-Coefficient a (95% CI) | P | |
| Common mental disorderb | ||||
| At phase 3 – Sugar intake change: phase 3 to 5 | ||||
| Reduction | 268 | 1201 | 1.0 (reference) | |
| No change | 584 | 2860 | 0.91 (0.77, 1.08) | 0.27 |
| Increase | 198 | 961 | 0.91 (0.74, 1.12) | 0.39 |
| Continuous change in grams per day | 1050 | 5022 | 0.08 (−1.89, 2.05) | 0.94 |
| At phase 5 – Sugar intake change: phase 5 to 7 | ||||
| Reduction | 210 | 1025 | 1.0 (reference) | |
| No change | 464 | 2410 | 0.93 (0.77, 1.11) | 0.41 |
| Increase | 176 | 734 | 1.21 (0.96, 1.53) | 0.10 |
| Continuous change in grams per day | 850 | 4169 | 1.18 (−0.97, 3.33) | 0.28 |
| At phase 7 – Sugar intake change: phase 7 to 9 | ||||
| Reduction | 200 | 744 | 1.0 (reference) | |
| No change | 505 | 2206 | 0.87 (0.73, 1.05) | 0.15 |
| I ncrease | 150 | 692 | 0.84 (0.66, 1.06) | 0.14 |
| Continuous change in grams per day | 855 | 4497 | −1.14 (−3.09, 0.82) | 0.26 |
| Depressionc | ||||
| At phase 7 – Sugar intake change: phase 7 to 9 | ||||
| Reduction | 116 | 764 | 1.0 (reference) | |
| No change | 340 | 2233 | 1.05 (0.83, 1.32) | 0.70 |
| Increase | 97 | 688 | 0.98 (0.73, 1.32) | 0.90 |
| Continuous change in grams per day | 533 | 4238 | 1.01 (−1.35, 3.36) | 0.40 |
Abbreviations: No. = number, CI = confidence interval.
aChange in sugar intake in cases compared with non-cases, adjusted for age, sex and ethnicity. bCommon mental disorder measured using the 30-item General Health Questionnaire. cDepression measured using 20-item the Centre of Epidemiologic Studies Depression Scale.
Discussion
The present long-term prospective study is the first to investigate the association of sugar consumption from sweet food/beverages with prevalent, incident and recurrent mood disorders, while also examining the effect these disorders might have on subsequent habitual sugar intake. We found an adverse effect of higher sugar intake on mental health cross-sectionally and 5 years later in a study based on 23,245 repeated measures in men and women aged between 39 and 83. Further, we found an increased likelihood for incident CMD in men and some evidence of recurrent depression in both sexes with higher intakes of sugar from sweet food/beverages. These associations with incident CMD could not be explained by socio-demo graphic factors, other diet-related factors, adiposity and other diseases although the association with recurrent depression was explained by other diet-related factors.
In our study we were able to exclude potential ‘reverse causation’ as the reason for the observed link between high sugar intake and low mood. Over years and decades, it could be that those susceptible to depression tend to increase their sugar intake. This group may tend to report higher consumption at study baseline even in the absence of depression at the time of the questionnaire, while having an increased risk of future depression compared to other participants14, 15. However, there was no support for this alternative hypothesis, since the observed associations in our analysis were not the result of secondary changes in consumption of sugary food and drinks. Our study findings are consistent with the hypothesis that high sugar intake plays a causal role in the risks of both incident and recurrent depression and CMD.
Higher sugar intake from sweet food/beverages was associated with increased likelihood of incident CMD after 5 years in men. The association in men was in line with results from previous prospective studies in American and Spanish cohorts9–11. There are several potential explanations for the observed sex differences. First, the associations in men for incident CMD show a stronger effect with a bigger sample (comparing analysis of 2-year CMD with 5-year CMD), suggesting the lower number of female participants in our sample could have impaired the power of the analysis. Second, the results might reflect differences in pathways of depression by sex and type of depressive symptomatology52–54. Third, differences could be due to limitations of the study or to chance.
As described in the Introduction there are four potential mechanisms for an association of habitual sugar intake and subsequent depression risk. Sugar intake could increase depression risk over its potential influence on BDNF levels16 and inflammation20 which are both discussed as potential biological explanations for depression17, 21. Furthermore postprandial hypoglycaemia22 and addiction-like effects of sugar influencing neurotransmitters23–25 could link sugar intake with low mood. The pathway of postprandial hypoglycaemia is also relevant in the context of Glycaemic index, which has been shown to be associated with depression prevalence and incidence55, 56. However, it is a complex issue to tease apart the effects of a single nutrient in epidemiological studies since foods represent a mix of macro- and micronutrients. In this study associations were attenuated when adjusted for diet-related factors providing evidence of confounding and suggesting that the effect of sugar intake from sweet food/beverages could be partly explained by other components of the diet. Also, given that we analysed sugar intake from aggregated sweet foods and beverages we cannot rule out that certain types of foods and their particular components such as saturated fat content may have affected our findings. In our analysis, the association of sugar intake and recurrent depression was attenuated by measures of body fatness in participants without doctor diagnosis of depression at baseline supporting the hypothesis of an indirect effect mediated by adiposity26–28 driving the association of sugar intake and recurrent depression.
Meanwhile, there are several sources of possible error. Our study was based on an occupational cohort but sugar intakes from sweet food/beverages were close to those reported previously in a representative cohort in the UK (approximately 40 grams), and Batty et al. showed that effects found in Whitehall II were comparable to those observed in population-representative cohorts3, 57. A major limitation was the use of FFQ to derive diet data. FFQ data is subject to misreporting and underreporting, which have been found to differ by food group, depressive mood and BMI58–60. As reported previously in Whitehall, we showed a clear trend of lower sugar intake with higher BMI in men60. Nutrient content was based on food composition tables from 1991 and has to be considered as a source of error, since food composition especially of highly processed food is likely to change over the course of 18 years. In this long-term follow-up study, sugar intake from sweet food/beverages, which are consistently high in sugar content, has been used as the exposure measure. Compared to a measure of intake that includes processed foods61, this method may involve less information bias. Furthermore, this FFQ is meant to reflect habitual diet over the course of a year and therefore might not pick up short-term diet changes or occasional binge eating30. Although we adjusted for a number of potential confounders, we cannot rule out residual confounding through unknown or unmeasured factors. Finally, not all depression measures were obtained in all phases and selective dropout due to depressive symptoms might have influenced case numbers62.
In conclusion, our study provides evidence that sugar intake from sweet food/beverages increases the chance of incident mood disorders in men and limited evidence regarding recurrent mood disorders in both sexes. With a high prevalence of mood disorders, and sugar intake commonly two to three times the level recommended, our findings indicate that policies promoting the reduction of sugar intake could additionally support primary and secondary prevention of depression. To elucidate the association further, especially regarding observed sex differences our study should be replicated in representative prospective cohorts.
Electronic supplementary material
Acknowledgements
We thank all participating women and men in the Whitehall II Study, as well as all Whitehall II research scientists, study and data managers and clinical and administrative staff who make the study possible. The UK Medical Research Council, British Heart Foundation, and the US National Institutes of Health (R01HL36310, R01AG013196) have supported collection of data in the Whitehall II Study. This research is part of the Multi-country collaborative project on the role of Diet, Food-related behaviour, and Obesity in the prevention of Depression (MooDFOOD) and was supported by the Seventh Framework Programme of the European Commission (FP7-KKBE-2013-2-1-01). MJS is partly supported by the British Heart Foundation.
Author Contributions
E.J.B., A.K. and M.J.S. designed research; A.K. analysed the data; A.K., E.J.B., M.J.S., C.H.L. wrote the paper; E.B. had primary responsibility for final content. All authors read and approved the final manuscript.
Competing Interests
The authors declare that they have no competing interests.
Footnotes
Electronic supplementary material
Supplementary information accompanies this paper at doi:10.1038/s41598-017-05649-7
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- 1.WHO. Guideline: Sugar intake for adults and children. WHO Document Production Services (2015).
- 2.Public Health England. Sugar Reduction The evidence for action, https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/470179/Sugar_reduction_The_evidence_for_action.pdf (2015).
- 3.Public Health England. National Diet and Nutrition Survey: Results from Years 1–4 (combined) of the Rolling Programme (2008/2009 -2011/12) (2014).
- 4.Welsh JA, Sharma AJ, Grellinger L, Vos MB. Consumption of added sugars is decreasing in the United States. Am J Clin Nutr. 2011;94:726–734. doi: 10.3945/ajcn.111.018366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3:e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.El Ansari W, Adetunji H, Oskrochi R. Food and mental health: Relationship between food and perceived stress and depressive symptoms among university students in the United Kingdom. Cent. Eur. J. Public Health. 2014;22:90–97. doi: 10.21101/cejph.a3941. [DOI] [PubMed] [Google Scholar]
- 7.Yu B, et al. Soft drink consumption is associated with depressive symptoms among adults in China. Journal of Affective Disorders. 2015;172:422–427. doi: 10.1016/j.jad.2014.10.026. [DOI] [PubMed] [Google Scholar]
- 8.Westover AN, Marangell LB. A cross-national relationship between sugar consumption and major depression? Depression and Anxiety. 2002;16:118–120. doi: 10.1002/da.10054. [DOI] [PubMed] [Google Scholar]
- 9.Gangwisch JE, et al. High glycemic index diet as a risk factor for depression: analyses from the Women’s Health Initiative. Am J Clin Nutr. 2015;102:454–463. doi: 10.3945/ajcn.114.103846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Guo X, et al. Sweetened Beverages, Coffee, and Tea and Depression Risk among Older US Adults. PLoS ONE. 2014;9:e94715. doi: 10.1371/journal.pone.0094715. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Sánchez-Villegas A, et al. Fast-food and commercial baked goods consumption and the risk of depression. Public health nutrition. 2012;15:424–432. doi: 10.1017/S1368980011001856. [DOI] [PubMed] [Google Scholar]
- 12.Sanchez-Villegas A, et al. Validity of a self-reported diagnosis of depression among participants in a cohort study using the Structured Clinical Interview for DSM-IV (SCID-I) BMC psychiatry. 2008;8:1–8. doi: 10.1186/1471-244X-8-43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jeffery RW, et al. Reported food choices in older women in relation to body mass index and depressive symptoms. Appetite. 2009;52:238–240. doi: 10.1016/j.appet.2008.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Singh, M. Mood, food, and obesity. Frontiers in Psychology5 (2014). [DOI] [PMC free article] [PubMed]
- 15.Macht M. How emotions affect eating: A five-way model. Appetite. 2008;50:1–11. doi: 10.1016/j.appet.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 16.Sen S, Duman R, Sanacora G. Serum Brain-Derived Neurotrophic Factor, Depression, and Antidepressant Medications: Meta-Analyses and Implications. Biological Psychiatry. 2008;64:527–532. doi: 10.1016/j.biopsych.2008.05.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Molteni R, Barnard RJ, Ying Z, Roberts CK, Gomez-Pinilla F. A high-fat, refined sugar diet reduces hippocampal brain-derived neurotrophic factor, neuronal plasticity, and learning. Neuroscience. 2002;112:803–814. doi: 10.1016/S0306-4522(02)00123-9. [DOI] [PubMed] [Google Scholar]
- 18.Gainey SJ, et al. Short-Term High-Fat Diet (HFD) Induced Anxiety-Like Behaviors and Cognitive Impairment Are Improved with Treatment by Glyburide. Front Behav Neurosci. 2016;10:156. doi: 10.3389/fnbeh.2016.00156. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Heyward FD, et al. Adult mice maintained on a high-fat diet exhibit object location memory deficits and reduced hippocampal SIRT1 gene expression. Neurobiol Learn Mem. 2012;98:25–32. doi: 10.1016/j.nlm.2012.04.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Calder PC, et al. Dietary factors and low-grade inflammation in relation to overweight and obesity. British Journal of Nutrition. 2011;106:S1–S78. doi: 10.1017/S0007114511004193. [DOI] [PubMed] [Google Scholar]
- 21.Kivimaki M, et al. Long-term inflammation increases risk of common mental disorder: a cohort study. Mol Psychiatry. 2014;19:149–150. doi: 10.1038/mp.2013.35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Schwartz, N. S., Clutter, W. E., Shah, S. D. & Cryer, P. E. Glycemic thresholds for activation of glucose counterregulatory systems are higher than the threshold for symptoms. Journal of Clinical Investigation 79, 777–781 (1987). [DOI] [PMC free article] [PubMed]
- 23.Avena NM, Rada P, Hoebel BG. Evidence for sugar addiction: Behavioral and neurochemical effects of intermittent, excessive sugar intake. Neuroscience & Biobehavioral Reviews. 2008;32:20–39. doi: 10.1016/j.neubiorev.2007.04.019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Dunlop BW, Nemeroff CB. The role of dopamine in the pathophysiology of depression. Arch Gen Psychiatry. 2007;64:327–337. doi: 10.1001/archpsyc.64.3.327. [DOI] [PubMed] [Google Scholar]
- 25.Grant BF, Stinson FS, Dawson DA, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: Results from the national epidemiologic survey on alcohol and related conditions. Archives of General Psychiatry. 2004;61:807–816. doi: 10.1001/archpsyc.61.8.807. [DOI] [PubMed] [Google Scholar]
- 26.Te Morenga L, Mallard S, Mann J. Dietary sugars and body weight: systematic review and meta-analyses of randomised controlled trials and cohort studies. Bmj. 2013;346:e7492. doi: 10.1136/bmj.e7492. [DOI] [PubMed] [Google Scholar]
- 27.Luppino FS, de Wit LM, Bouvy PF, et al. Overweight, obesity, and depression: A systematic review and meta-analysis of longitudinal studies. Archives of General Psychiatry. 2010;67:220–229. doi: 10.1001/archgenpsychiatry.2010.2. [DOI] [PubMed] [Google Scholar]
- 28.Jackson SE, Beeken RJ, Wardle J. Obesity, perceived weight discrimination, and psychological well-being in older adults in England. Obesity (Silver.Spring) 2015;23:1105–1111. doi: 10.1002/oby.21052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Marmot M, Brunner E. Cohort Profile: The Whitehall II study. International Journal of Epidemiology. 2005;34:251–256. doi: 10.1093/ije/dyh372. [DOI] [PubMed] [Google Scholar]
- 30.Brunner E, Juneja M, Marmot M. Dietary assessment in Whitehall II: comparison of 7 d diet diary and food-frequency questionnaire and validity against biomarkers. British Journal of Nutrition. 2001;86:405–414. doi: 10.1079/BJN2001414. [DOI] [PubMed] [Google Scholar]
- 31.Willett WC, et al. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol. 1985;122:51–65. doi: 10.1093/oxfordjournals.aje.a114086. [DOI] [PubMed] [Google Scholar]
- 32.Bingham, S. A. et al. Validation of dietary assessment methods in the UK arm of EPIC using weighed records, and 24-hour urinary nitrogen and potassium and serum vitamin C and carotenoids as biomarkers International Journal of Epidemiology 26, S137 (1997). [DOI] [PubMed]
- 33.Holland, B., Unwin, I., Buss, D., Pauk, A. & Southgate, D. McCance and Widdowson’s The Composition of Foods, 5th edition. (Royal Society of Chemistry 1991).
- 34.Goldberg, D. P. The detection of psychiatric illness by questionnaire: A technique for the identification and assessment of non-psychotic psychiatric illness. (Oxford U. Press, 1972).
- 35.Radloff LS. The CES-D Scale: A Self-Report Depression Scale for Research in the General Population. Applied Psychological Measurement. 1977;1:385–401. doi: 10.1177/014662167700100306. [DOI] [Google Scholar]
- 36.Stansfeld S, Head J, Bartley M, Fonagy P. Social position, early deprivation and the development of attachment. Soc Psychiat Epidemiol. 2008;43:516–526. doi: 10.1007/s00127-008-0330-4. [DOI] [PubMed] [Google Scholar]
- 37.Lewis G, Pelosi AJ, Araya R, Dunn G. Measuring psychiatric disorder in the community: a standardized assessment for use by lay interviewers. Psychol Med. 1992;22:465–486. doi: 10.1017/S0033291700030415. [DOI] [PubMed] [Google Scholar]
- 38.Lewis G, et al. The development of a computerized assessment for minor psychiatric disorder. Psychological Medicine. 1988;18:737–745. doi: 10.1017/S0033291700008448. [DOI] [PubMed] [Google Scholar]
- 39.Head J, et al. Use of self-administered instruments to assess psychiatric disorders in older people: validity of the General Health Questionnaire, the Center for Epidemiologic Studies Depression Scale and the self-completion version of the revised Clinical Interview Schedule. Psychol Med. 2013;43:2649–2656. doi: 10.1017/S0033291713000342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Kumari M, Head J, Marmot M. Prospective Study of Social and Other Risk Factors for Incidence of Type 2 Diabetes in the Whitehall II Study. Archives of Internal Medicine. 2004;164:1873–1880. doi: 10.1001/archinte.164.17.1873. [DOI] [PubMed] [Google Scholar]
- 41.Schofield WN. Predicting basal metabolic rate, new standards and review of previous work. Hum Nutr Clin Nutr. 1985;39(Suppl 1):5–41. [PubMed] [Google Scholar]
- 42.Mosdøl, A., Witte, D. R., Frost, G., Marmot, M. G. & Brunner, E. J. Dietary glycemic index and glycemic load are associated with high-density-lipoprotein cholesterol at baseline but not with increased risk of diabetes in the Whitehall II study. The American Journal of Clinical Nutrition86, 988–994 (2007). [DOI] [PubMed]
- 43.Department of Health Great Britain. Dietary reference values for food energy and nutrients for the United Kingdom: Report of the Panel on Dietary Reference Values of the Committee on Medical Aspects of Food Policy. (H.M.S.O., 1991). [PubMed]
- 44.Willett, W. C., Howe, G. R. & Kushi, L. H. Adjustment for total energy intake in epidemiologic studies. Am J Clin Nutr 65, 1220S–1228S, discussion 1229S–1231S (1997). [DOI] [PubMed]
- 45.Fung TT, et al. Adherence to a DASH-style diet and risk of coronary heart disease and stroke in women. Arch Intern Med. 2008;168:713–720. doi: 10.1001/archinte.168.7.713. [DOI] [PubMed] [Google Scholar]
- 46.WHO. Obesity: preventing and managing the global epidemic. WHO Document Production Services (2000).
- 47.Willett, W. Nutritional epidemiology (2013).
- 48.Twisk JW. Longitudinal data analysis. A comparison between generalized estimating equations and random coefficient analysis. Eur J Epidemiol. 2004;19:769–776. doi: 10.1023/B:EJEP.0000036572.00663.f2. [DOI] [PubMed] [Google Scholar]
- 49.Brunner EJ, et al. Depressive disorder, coronary heart disease, and stroke: dose-response and reverse causation effects in the Whitehall II cohort study. Eur J Prev Cardiol. 2014;21:340–346. doi: 10.1177/2047487314520785. [DOI] [PubMed] [Google Scholar]
- 50.Stata Statistical Software: Release 14 (StataCorp LP, College Station, TX, 2015).
- 51.Akbaraly TN, Sabia S, Shipley MJ, Batty GD, Kivimaki M. Adherence to healthy dietary guidelines and future depressive symptoms: evidence for sex differentials in the Whitehall II study. Am J Clin Nutr. 2013;97:419–427. doi: 10.3945/ajcn.112.041582. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Rahe C, et al. Associations between depression subtypes, depression severity and diet quality: cross-sectional findings from the BiDirect Study. BMC Psychiatry. 2015;15:38. doi: 10.1186/s12888-015-0426-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Agurs-Collins T, Fuemmeler BF. Dopamine polymorphisms and depressive symptoms predict foods intake. Results from a nationally representative sample. Appetite. 2011;57:339–348. doi: 10.1016/j.appet.2011.05.325. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Verhagen M, et al. Meta-analysis of the BDNF Val66Met polymorphism in major depressive disorder: effects of gender and ethnicity. Mol. Psychiatry. 2010;15:260–271. doi: 10.1038/mp.2008.109. [DOI] [PubMed] [Google Scholar]
- 55.Gopinath B, Flood VM, Burlutksy G, Louie JCY, Mitchell P. Association between carbohydrate nutrition and prevalence of depressive symptoms in older adults. British Journal of Nutrition. 2016;116:2109–2114. doi: 10.1017/S0007114516004311. [DOI] [PubMed] [Google Scholar]
- 56.Gangwisch, J. E. et al. High glycemic index diet as a risk factor for depression: analyses from the Women’s Health Initiative. Am. J. Clin. Nutr (2015). [DOI] [PMC free article] [PubMed]
- 57.Batty GD, et al. Generalizability of Occupational Cohort Study Findings. Epidemiology. 2014;25:932–933. doi: 10.1097/EDE.0000000000000184. [DOI] [PubMed] [Google Scholar]
- 58.Lutomski JE, van den Broeck J, Harrington J, Shiely F, Perry IJ. Sociodemographic, lifestyle, mental health and dietary factors associated with direction of misreporting of energy intake. Public health nutrition. 2011;14:532–541. doi: 10.1017/S1368980010001801. [DOI] [PubMed] [Google Scholar]
- 59.Millen AE, et al. Differences between Food Group Reports of Low-Energy Reporters and Non–Low-Energy Reporters on a Food Frequency Questionnaire. Journal of the American Dietetic Association. 2009;109:1194–1203. doi: 10.1016/j.jada.2009.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Stallone DD, Brunner EJ, Bingham SA, Marmot MG. Dietary assessment in Whitehall II: the influence of reporting bias on apparent socioeconomic variation in nutrient intakes. Eur J Clin Nutr. 1997;51:815–825. doi: 10.1038/sj.ejcn.1600491. [DOI] [PubMed] [Google Scholar]
- 61.Louie JC, et al. A systematic methodology to estimate added sugar content of foods. Eur J Clin Nutr. 2015;69:154–161. doi: 10.1038/ejcn.2014.256. [DOI] [PubMed] [Google Scholar]
- 62.Jokela M, et al. Natural course of recurrent psychological distress in adulthood. J Affect Disord. 2011;130:454–461. doi: 10.1016/j.jad.2010.10.047. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.