

Abstract
A 34-year-old male presented with an 8-month history of passing increasingly painful ‘grit’ in his ejaculate. Semen analysis was normal as were urinary and blood tests. T1-weighted MRI revealed several bilateral high-signal areas measuring up to 1 cm in diameter, located in the seminal vesicles. These were confirmed as calculi on T2-weighted imaging and a seminal vesiculogram, with no drainage from the left ejaculatory duct and only minimal from the right duct. He is currently awaiting a robot-assisted laparoscopic vesiculotomy after completion of family.
Keywords: Urinary and genital tract disorders, Surgery, Urological surgery, Urology
Background
Seminal vesicle calculi are rare.1 2 A systematic review found only 213 reported cases of seminal vesicle calculi between 1928 and 2016.3 This is in comparison to ejaculatory duct calcifications which, in a recent retrospective study investigating seminal vesicle ultrasound characteristics reported a prevalence of 8.2%.4 Furthermore, a literature review in 2011 found only six reports of large, bilateral calculi.2 Literature shows that often, men present with haematospermia and ejaculatory pain and rarely report on passing calculi with their semen, defined as spermolithiasis.5 6 Altered fertility due to bilateral seminal vesicle calculi has not been frequently reported unless there is coexisting ejaculatory duct obstruction1 7; however one needs to consider that any surgical intervention for their management could result in impaired fertility. This case is not only a rare presentation but also presents a management challenge as preserving fertility was of paramount importance given that the patient’s family was not complete at the time of the diagnosis.
Case presentation
A 34-year-old male presented with an 8-month history of passing ‘grit’ in his ejaculate, which was becoming increasingly painful. He denied any haematospermia or haematuria and reported no lower urinary tract symptoms or history of urinary tract infections. He was in good general health with his medical history including only a right-sided inguinal hernia repair as a child. Neither he nor his family had any history of stone diseases and he was not diabetic. He was newly married and had no children.
Clinical examination revealed normal feeling testicles and he had a normal feeling prostate on digital rectal examination. Systematic examination of all organ systems did not reveal any abnormality.
Investigations
Routine urinalysis was normal and semen analysis detected normal sperm count (117 million/mL) with total motility of 63%, progressive motility 60% and normal morphology of 5%. This was normal according to WHO criteria 2010.8 Fourier transform infrared spectrometry of the semen sample showed features consistent with organic material, mainly protein and tested positive for blood. Routine blood tests including renal function tests, calcium, parathyroid hormone and uric acid were normal. An ultrasound of his scrotum was performed, which revealed normal testes and a small epididymal cyst on the right side. A transrectal ultrasound (TRUS) scan of his prostate and seminal vesicles, using a BK Falcon with biplanar probe reported a normal appearing prostate (volume 28.6 cm3) and a small calcified area near the prostatic urethra. Vas deferens was not explored by ultrasound. The seminal vesicles were not adequately visualised.
A decision was made to perform a MRI scan to delineate the anatomy of the seminal vesicles and the cause of the spermolithiasis. Precontrast T1-weighted images demonstrated several large high-signal areas within the seminal vesicles which did not enhance following contrast. T2-weighted images showed multiple areas within the seminal vesicles surrounded by the seminal vesicle fluid and measuring up to 1 cm suggestive of calculi (figure 1).
Figure 1.
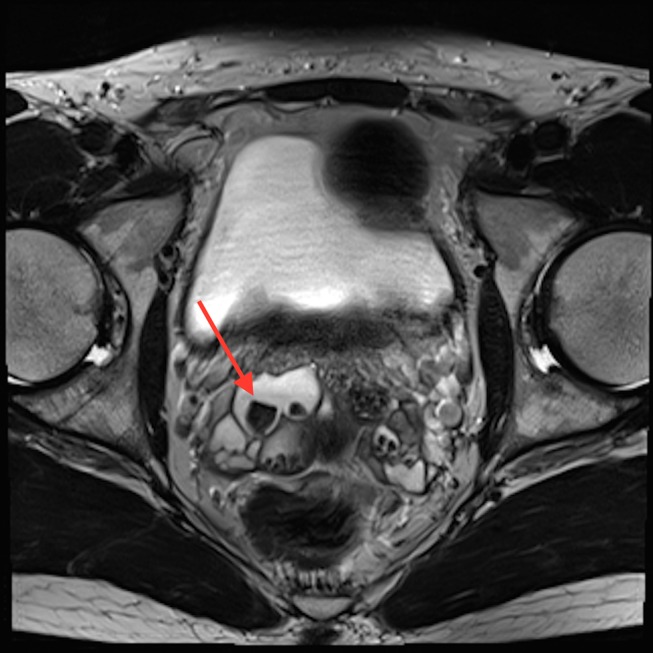
T2-weighted axial MRI showing multiple calculi within the seminal vesicles surrounded by seminal fluid. Arrow identifies one of the larger calculi seen,
A seminal vesiculogram was recommended following review of the images in a supraregional specialist multidisciplinary meeting. This confirmed the presence of bilateral seminal vesicle calculi and also the presence of a small calculus in the proximal right ejaculatory duct (figures 2 and 3). There were no anatomical abnormalities related to the seminal vesicles. This was performed under general anaesthetic with antibiotic cover and the patient made an uncomplicated recovery postprocedure.
Figure 2.
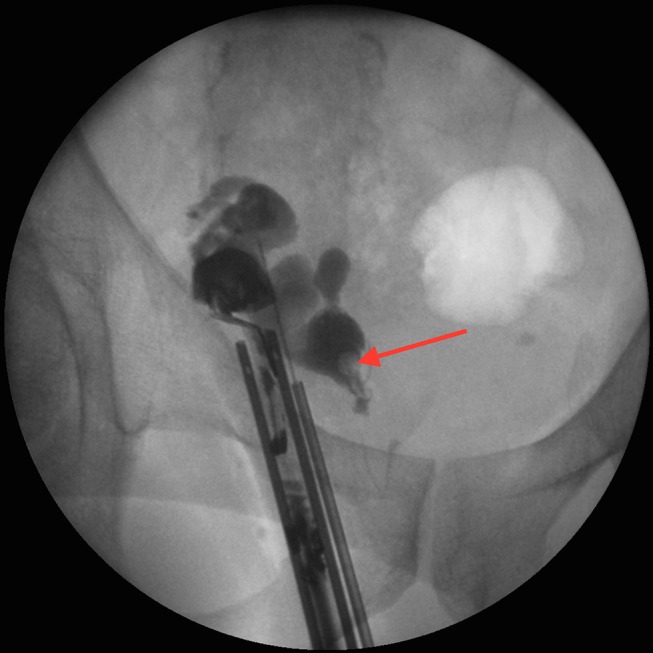
Antegrade seminal vesiculogram showing calculus proximal to the right ejaculatory duct (arrow).
Figure 3.
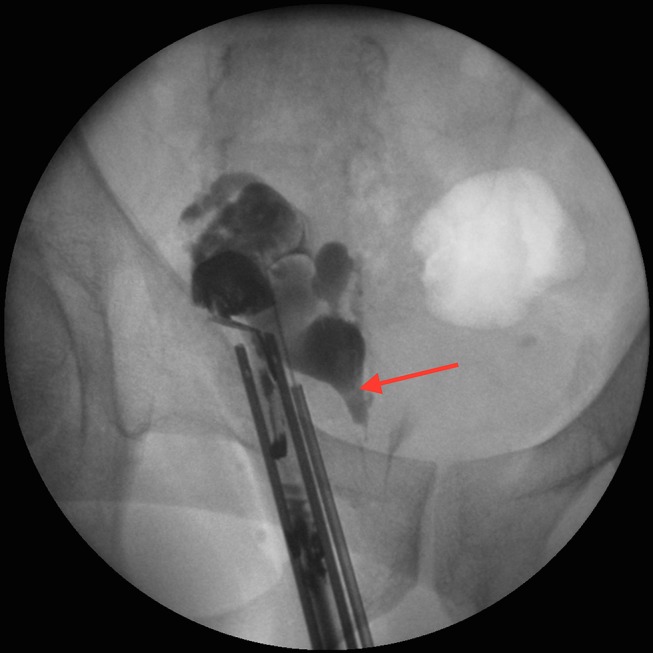
Antegrade seminal vesiculogram showing multiple calculi (arrow) within the right seminal vesicle.
Outcome and follow-up
Following confirmation of the diagnosis of large bilateral seminal vesicle calculi and discussion at the multidisciplinary team meeting, a consultation took place with the patient. Treatment of these stones poses a surgical challenge due to difficult organ access as well as a risk of infertility. A literature review on the management of seminal vesicle calculi revealed that transutricular seminal vesiculoscopy and laser lithotripsy had become common practice in Asia for the management of multiple small ejaculatory duct and seminal vesicle calculi.9–12 However, this procedure is not approved by the National Institute for Health and Care Excellence in the UK and there is a lack of expertise in this technique.13 A consultation followed with the patient and he was offered sperm cryopreservation and robot-assisted laparoscopic vesiculotomy and stone retrieval in a UK specialist centre with advanced expertise in pelvic robotic surgery in men. The patient opted to delay treatment until after completion of his family and is currently undergoing interim follow-up for symptom monitoring.
Discussion
The first reported seminal vesicle calculus was in 1928 by White.9 Previous literature suggests that the pathogenesis behind formation of seminal vesicle calculi are variable. Proposed aetiologies include obstruction of the ejaculatory duct, infective processes, congenital anatomical anomalies (mullerian remnant cysts) and urinary reflux into the ejaculatory ducts (idiopathic or iatrogenic following transurethral resection of ejaculatory ducts).5 14 15 Lottie et al4 correlated the function of the seminal vesicles with their US features and reported patients with reduced seminal vesicle ejection fraction had increased US abnormalities including giant cysts of the seminal vesicles and ejaculatory duct dilatation and calcification. The presence of seminal vesicle calculi are also considered a sign of chronicity in male accessory gland infection (such as prostatitis or seminal vesiculitis)9 11 16–19. While hypercalcaemia is known to cause urinary tract calculi, there is currently no clear evidence to suggest it has a role in the formation of seminal vesicle calculi.20 Calcification within the seminal vesicles and vas deferens has been linked to metabolic conditions, most notably diabetes21 as well as chronic inflammation secondary to disease processes such as tuberculosis, schistosomiasis, chlamydia, gonorrhoea and prostatitis. Mechanical obstruction and invasive carcinoma are also associated aetiologies.22–25 It must be remembered however that calcification of seminal vesicle tissue is a separate pathology to seminal vesicle calculi.26 Stone analysis provides composition information and possible pathogenesis. In most cases, these stones are comprised of proteinaceous material but carbonate apatite, calcium oxalate and calcium fluorophosphate stones have also been reported.10 27 28
Primary symptoms vary but can consist of haematospermia, ejaculatory pain, perineal and testicular pain, lower urinary tract symptoms and less frequently subfertility and spermolithiasis.5 6 Indeed, Yang et al11 reported findings of seminal vesicle calculi in 16.2% of their case series of patients with persistent haematospermia. Ejaculatory duct obstruction secondary to calculi can occur in patients with seminal vesicle stones and can result in subfertility.17 29 Of note, in our case, the patient had no previous urological history, had normal fertility according to WHO 2010 criteria8 and presented only with painful, gritty ejaculation.
Beyond history and clinical examination, semen analysis should be performed as bilateral obstructive calculi could be a cause for obstructive azoospermia.7 30 Initial serum investigations include renal function tests, as well as calcium and uric acid levels to exclude predisposing conditions for stone formation. Methods used to identify abnormalities of the seminal vesicles include TRUS, CT and MRI. The merits of TRUS as an investigative imaging modality were first described by Littrup et al in 1988.31 Nowadays, ultrasound is the gold standard imaging modality for the evaluation of seminal vesicle diameters4 and TRUS is regularly used across urology centres, having high sensitivity for detecting abnormalities within the prostate and seminal vesicles. Indeed, a recent review demonstrates a rise in the diagnosis of seminal vesicle calculi since the introduction of TRUS to clinical practice.3 It is a cheaper investigation, easily available in a clinical setting and in experienced hands provides excellent views of the seminal vesicles, prostate and ejaculatory ducts. In comparison to MRI, it avoids the need for preparation or radiation exposure.12 However, currently features suggestive of ejaculatory duct obstruction (such as dilation) are not standardised and assessment of echotecture is best evaluated after ejaculation.4 In our case, the TRUS did not image the seminal vesicles adequately and the diagnosis of large bilateral calculi was concluded following MRI and antegrade seminal vesiculogram.
In our case, a vesiculogram added valuable information as to the patency of the ducts and location of calculi—the relative merits of this investigation have been previously reported.10 Formerly treatment mainly consisted of an open vesiculectomy, which was associated with significant morbidity due to the anatomical location of the organs and the need for extensive pelvic dissection.15 However, current practises in Asia consist of fertility-preserving and minimally invasive techniques such as transutricular seminal vesiculoscopy with ureteroscopes and subsequent lithotripsy with or without the use of laser.9–12 Laparoscopic or robot assisted vesiculectomy for larger calculi is feasible via a transperitoneal approach and is a more acceptable method for the management of larger seminal vesicle calculi.1 7 28 It also allows anatomical correction of the seminal vesicle as these often remain dilated after stone extraction or when the calculus has formed within a seminal vesicle cyst.7 28
Learning points.
In a male presenting with painful, gritty ejaculation, seminal vesicle calculi must always be considered and the patient should be referred to an andrologist for assessment.
Interventional supplementary imaging such as seminal vesiculography can provide additional information of key importance when considering future surgical intervention in a tertiary centre.
Fertility preservation is of paramount importance prior to consideration of surgical treatment in a young male whose family is not yet complete.
Footnotes
Contributors: SAW was responsible for gaining the history of the case, the background research of the topic and the writing of the manuscript plus amendments. MC provided supervision and advice during the draft versions, made amendments and provided further relevant articles for additional evidence. RN provided guidance and supervision on how to present the case, provided imaging from investigations and oversaw the final edit prior to submission.
Competing interests: None declared.
Patient consent: Obtained.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1.Singh I, Ansari MS. Idiopathic bilateral giant seminal vesicle calculi and calcification of the male ejaculatory system: current review of diagnosis and management. Indian J Surg 2006;68:38–40. [Google Scholar]
- 2.Hadidi M, Hadidy A, Alrabadi AF, et al. Bilateral very large calcium oxalate stones in the seminal vesicles: case report and literature review. Urol Res 2011;39:509–13. 10.1007/s00240-011-0371-0 [DOI] [PubMed] [Google Scholar]
- 3.Christodoulidou M, Parnham A, Nigam R. Diagnosis and management of symptomatic seminal vesicle calculi. Scand J Urol 2017:1–8. 10.1080/21681805.2017.1295398 [DOI] [PubMed] [Google Scholar]
- 4.Lotti F, Corona G, Colpi GM, et al. Seminal vesicles ultrasound features in a cohort of infertility patients. Hum Reprod 2012;27:974–82. 10.1093/humrep/des032 [DOI] [PubMed] [Google Scholar]
- 5.Sandlow JI, Williams R. Surgery of the seminal vesicles : Walsh PC, Retik AB, Vaughan ED, Campbell’s Urology. 8th edn. Vol 4 Phildelphia: WB Saunders, 2002:3869–83. [Google Scholar]
- 6.Menon M, Parulkar BG, Drach GW, et al. Urinary lithiasis: etiology, diagnosis and medical management : Walsh PC, Retik AB, Vaughan ED, Campbell’s Urology. 7th edn. Vol 3 Phildelphia: WB Saunders, 1998:2661–733. [Google Scholar]
- 7.Gordon Z, Monga M. Endoscopic extraction of an ejaculatory duct calculus to treat obstructive azoospermia. J Endourol 2001;15:949–50. 10.1089/089277901753284206 [DOI] [PubMed] [Google Scholar]
- 8.Cooper TG, Noonan E, von Eckardstein S, et al. World Health Organization reference values for human semen characteristics. Hum Reprod Update 2010;16:231–45. 10.1093/humupd/dmp048 [DOI] [PubMed] [Google Scholar]
- 9.Ozgök Y, Kilciler M, Aydur E, et al. Endoscopic seminal vesicle stone removal. Urology 2005;65:591.e9–591.e12. 10.1016/j.urology.2004.09.015 [DOI] [PubMed] [Google Scholar]
- 10.Cuda SP, Brand TC, Thibault GP, et al. Case report: endoscopic laser lithotripsy of seminal-vesicle stones. J Endourol 2006;20:916–8. 10.1089/end.2006.20.916 [DOI] [PubMed] [Google Scholar]
- 11.Yang SC, Rha KH, Byon SK, et al. Techniques in endourology-transutricular seminal vesiculoscopy. J Endourol 2002;16:343–5. 10.1089/089277902760261347 [DOI] [PubMed] [Google Scholar]
- 12.Song T, Zhang X, Zhang L, et al. Transurethral seminal vesiculoscopy in the diagnosis and treatment of seminal vesicle stones. Chin Med J 2012;125:1475–8. [PubMed] [Google Scholar]
- 13.Improving health and social care through evidence-based guidance. www.nice.org.uk (accessed 1 Dec 2016).
- 14.Vellayappan BA, Tiong HY, Chua WJ, et al. Seminal vesicle calculus after transurethral resection of ejaculatory duct. Can J Urol 2007;14:3595–7. [PubMed] [Google Scholar]
- 15.Schwartz BF. Stones of the) urethra, prostate, seminal vesicle, bladder and encrusted foreign bodies : Stoller ML, Meng MV, Current clinical urology, urinary stone disease: a practical guide to medical and surgical management: Humana Press Incorporation, 2003:661–81. [Google Scholar]
- 16.Li YK. Diagnosis and management of large seminal vesicle stones. Br J Urol 1991;68:322–3. [DOI] [PubMed] [Google Scholar]
- 17.Modi PR. Case report: endoscopic management of seminal vesicle stones with cutaneous fistula. J Endourol 2006;20:432–5. 10.1089/end.2006.20.432 [DOI] [PubMed] [Google Scholar]
- 18.Liu B, Li J, Li P, et al. Transurethral seminal vesiculoscopy in the diagnosis and treatment of intractable seminal vesiculitis. J Int Med Res 2014;42:236–42. 10.1177/0300060513509472 [DOI] [PubMed] [Google Scholar]
- 19.Lotti F, Maggi M. Ultrasound of the male genital tract in relation to male reproductive health. Hum Reprod Update 2015;21:56–83. 10.1093/humupd/dmu042 [DOI] [PubMed] [Google Scholar]
- 20.Drach GW, et al. Urinary lithiasis: etiology, diagnosis and medical management : Walsh PC, Retik AB, Stamey TA, Campbell’s urology. 6th edn. 1993 Philadelphia: WB Saunders:2085–156. [Google Scholar]
- 21.Yadav R, Goel A, Sankhwar SN, et al. Incidentally detected bilaterally symmetrical seminal and vas calcification in young infertile male: a case report, literature review and algorithm for diagnosis. Can Urol Assoc J 2012;6:E206–E208. 10.5489/cuaj.12009 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Patel HR, Arya M, O'Donoghue EP. Calcified seminal vesicles and vasa deferentia: "beware or be aware". Scand J Urol Nephrol 2001;35:79–80. [DOI] [PubMed] [Google Scholar]
- 23.Vilana R, Corachán M, Gascón J, et al. Schistosomiasis of the male genital tract: transrectal sonographic findings. J Urol 1997;158:1491–3. 10.1016/S0022-5347(01)64251-4 [DOI] [PubMed] [Google Scholar]
- 24.Kuligowska E, Fenlon HM. Transrectal US in male infertility: spectrum of findings and role in patient care. Radiology 1998;207:173–81. 10.1148/radiology.207.1.9530314 [DOI] [PubMed] [Google Scholar]
- 25.Griffiths GJ, Clements R, Jones DR, et al. The ultrasound appearances of prostatic cancer with histological correlation. Clin Radiol 1987;38:219–27. 10.1016/S0009-9260(87)80048-X [DOI] [PubMed] [Google Scholar]
- 26.Stasinou T, Bourdoumis A, Owegie P, et al. Calcification of the vas deferens and seminal vesicles: a review. Can J Urol 2015;22:7594–8. [PubMed] [Google Scholar]
- 27.Yun SJ, Kim T-H, Kwon W-A, et al. A large stone in the dilated left seminal vesicle: laparoscopic removal and partial seminal vesiculectomy. Korean J Urol 2008;49:656–8. 10.4111/kju.2008.49.7.656 [DOI] [Google Scholar]
- 28.Han P, Yang YR, Zhang XY, et al. Laparoscopic treatment of a calcium fluorophosphate stone within a seminal vesicle cyst. Asian J Androl 2008;10:337–40. 10.1111/j.1745-7262.2008.00341.x [DOI] [PubMed] [Google Scholar]
- 29.Kilciler M, Sağlam M, Ozgök Y, et al. Giant seminal vesicle stones. Report of two cases. Urol Int 2002;69:250–1. [DOI] [PubMed] [Google Scholar]
- 30.Wang H, Ye H, Xu C, et al. Transurethral seminal vesiculoscopy using a 6F vesiculoscope for ejaculatory duct obstruction: initial experience. J Androl 2012;33:637–43. 10.2164/jandrol.111.013912 [DOI] [PubMed] [Google Scholar]
- 31.Littrup PJ, Lee F, McLeary RD, et al. Transrectal US of the seminal vesicles and ejaculatory ducts: clinical correlation. Radiology 1988;168:625–8. 10.1148/radiology.168.3.3043543 [DOI] [PubMed] [Google Scholar]